

To analyze the prevalence of ultra-processed food intake among children under one year of age and to identify associated factors.
MethodsA cross-sectional design was employed. We interviewed 198 mothers of children aged between 6 and 12 months in primary healthcare units located in a city of the metropolitan region of São Paulo, Brazil. Specific foods consumed in the previous 24h of the interview were considered to evaluate the consumption of ultra-processed foods. Variables related to mothers’ and children's characteristics as well as primary healthcare units were grouped into three blocks of increasingly proximal influence on the outcome. A Poisson regression analysis was performed following a statistical hierarchical modeling to determine factors associated with ultra-processed food intake.
ResultsThe prevalence of ultra-processed food intake was 43.1%. Infants that were not being breastfed had a higher prevalence of ultra-processed food intake but no statistical significance was found. Lower maternal education (prevalence ratio 1.55 [1.08–2.24]) and the child's first appointment at the primary healthcare unit having happened after the first week of life (prevalence ratio 1.51 [1.01–2.27]) were factors associated with the consumption of ultra-processed foods.
ConclusionsHigh consumption of ultra-processed foods among children under 1 year of age was found. Both maternal socioeconomic status and time until the child's first appointment at the primary healthcare unit were associated with the prevalence of ultra-processed food intake.
Analisar a prevalência do consumo de alimentos ultraprocessados entre crianças com menos de um ano e identificar os fatores associados.
MétodosFoi realizado um estudo transversal. Entrevistamos 198 mães de crianças com idades entre 6 e 12 meses em unidades de atenção primária à saúde localizadas em Embu das Artes, uma cidade da região metropolitana de São Paulo, Brasil. Alimentos específicos consumidos nas 24 horas anteriores à entrevista foram considerados para avaliar o consumo de alimentos ultraprocessados. As variáveis relacionadas às características das mães e crianças e as unidades de atenção primária à saúde foram agrupadas em três blocos de influência cada vez mais proximal com o resultado. Foi realizada uma análise de regressão de Poisson de acordo com um modelo estatístico hierárquico para determinar os fatores associados ao consumo de alimentos ultraprocessados.
ResultadosA prevalência de consumo de alimentos ultraprocessados foi 43,1%. As crianças que não eram amamentadas apresentaram maior prevalência de consumo de alimentos ultraprocessados, porém não foi encontrada diferença estatística. Menor nível de escolaridade materna (RP 1,55 [1,08–2,24]) e o fato de a primeira consulta da criança na unidade de atenção primária à saúde acontecer na primeira semana de vida (RP 1,51 [1,01–2,27]) foram fatores associados ao consumo de alimentos ultraprocessados.
ConclusõesFoi encontrado consumo elevado de alimentos ultraprocessados entre crianças com menos de um ano. A situação socioeconômica materna e o tempo da primeira consulta da criança na unidade de atenção primária à saúde foram associados à prevalência de consumo de alimentos ultraprocessados.
According to the World Health Organization (WHO), complementary feeding comprises the process of transition from exclusive breastfeeding to family foods. It should be timely and adequate, meaning that all infants from 6 months onwards should start receiving foods in addition to breast milk in amounts, frequency, consistency, and variety to cover the nutritional needs of the growing child.1 Introducing adequate complementary foods favors healthy feeding habits throughout life. The first two years of life represent a window of opportunity for infants to learn, accept, and like healthy foods as well as to establish long-term healthy dietary patterns.2,3 Besides, healthy feeding habits in early childhood can provide a lifetime of protection against chronic diseases, including overweight and obesity.4,5
Inadequate complementary feeding practices such as the early introduction of food (i.e. before 6 months of age), poorly diversified diet, inadequate frequency and consistency of food, and frequent consumption of unhealthy foods have become highly prevalent at the early ages of an infant's life.6–8 Recently, the concept of unhealthy foods has been modified by a new food classification system adopted by the Dietary Guidelines for the Brazilian Population.9NOVA is the new food classification that categorizes foods according to the extent and purpose of food processing, rather than in terms of nutrients.9 According to NOVA, ultra-processed food (UPF) and drink products are formulations made up mainly or solely of industrial ingredients. That includes biscuits, packaged snacks, soft drinks, and instant noodles, all of which are products that are not recommended to be offered before a child reaches the age of 2 years.10 A recent national survey unfortunately found that 70% of the Brazilian children between 9 and 12 months consumed some type of UPF on the day before the survey.8
Even though some studies have investigated the determinants for inadequate complementary feeding practices among children,6,7 there is a lack of studies exploring factors associated with consumption of UPF in infants specifically in the context of primary health care. Primary health care is a privileged setting for the development of interventions aimed at preventing unhealthy eating habits and promoting healthy ones.11 Thus, this study aimed to analyze the prevalence and factors associated with the consumption of UPF among children under 1 year of age in primary healthcare units.
MethodsDesign and study settingThis study was carried out in 13 urban primary healthcare units (PHU) in Embu das Artes, Brazil. This municipality is part of the metropolitan region of São Paulo and has a total population of 240,230 inhabitants.
The data used for this analysis was taken from a baseline survey of a before-and-after intervention study. In brief, the educational intervention conducted with primary healthcare professionals aimed to promote breastfeeding and complementary feeding activities, and findings from its assessment will be described elsewhere. Before the intervention, a survey on infant feeding practices was conducted among mothers of children under 1 year attending PHUs.
Sampling frameworks and analytic sampleThe sample size was calculated assuming a margin of error of 5% and a statistical power of 90%; it was determined on a prevalence of intake of sandwiches, cookies, chips or savory biscuits (among children aged between 6 and 9 months) estimated at 67%.12 It resulted in a sample size of 161 children between 6 and 12 months of age.
Ethical considerationsThe research protocol was approved by the Research Ethics Committee of the Public Health School of Universidade de São Paulo–Brazil (protocol 43317315.0.0000.5421, approved on July 5, 2015). All participants received an explanation of the study objectives and signed an informed consent form.
Data collectionParticipants were mothers of children under 1 year of age who attended PHUs on the period between June to September 2015. Interviews were conducted by trained staff. The data collection instrument was composed of two parts. The first part comprised closed-ended questions related to the socioeconomic, demographic, and biomedical conditions of mothers and children, as well as to the performance of the PHU by checking standard recommendations of the Brazilian Ministry of Health to support breastfeeding and complementary feeding (i.e. first appointment at the PHU [first week/after first week]; receiving home visits from health team [y/n]; regular appointments scheduled by the PHU [y/n]; attendance without appointment provided by the PHU [y/n]; receiving counseling on complementary feeding [y/n]).13 The second part comprised questions related to food consumption in the 24h prior to the interview; for those, the Food Intake Markers Questionnaire for infants aged between 6 and 24 months, proposed by the Brazilian Food and Nutrition Surveillance System (SISVAN), was adopted. This questionnaire consists of “yes” or “no” questions about food items or groups such as: fruits; vegetables; rice, pasta, and potatoes; beans; meat; breast milk; other milk and dairy products; and ultra-processed foods. It can be used to assess complementary feeding practices as well as the intake of ultra-processed foods. While it enables the assessment of markers of healthy and unhealthy food consumption, it does not evaluate the amount of food consumed.14
Outcome variableThe consumption of UPF in the previous 24h was determined for children aged between 6 and 12 months who had eaten at least one of the following foods, organized in four groups categorized as ultra-processed food products according to the NOVA classification9: (a) burgers, processed meat, or sausages; (b) sugary beverages (soft drinks, processed juices and other drinks with added sugar); (c) instant noodles, chips or savory biscuits; and (d) sandwich cookies, chocolates or candies. The use of “current status” of food consumption in the last 24h is recommended by the WHO to minimize recall bias in cross-sectional studies.1
CovariatesThe covariates included are described in Fig. 1. Maternal education was used as a proxy for socioeconomic status. Providing healthcare assistance on the first week of the child's life was used as a proxy for assessing the performance of the PHUs. The “First Week Integral Health” is a recommendation of the Ministry of Health in place since 2004 and it aims to improve maternal and child's health during the postpartum period.15 The variable “primary healthcare model” corresponds to the model of healthcare assistance offered at the PHUs: traditional – teams consisting of general practitioners, pediatricians, gynecologists, and nurses; Family Health Strategy – teams consisting of family physician, nurses, nursing technicians and community health workers; and mixed – primary healthcare units where both models coexist.

Diversity and adequacy of complementary feeding were defined based on the proposed Food Intake Markers by the Brazilian Ministry of Health,14 as follows: (1) minimum food diversity was considered when a child aged at 6–11 months received at least one of the six food groups (yes/no): (i) complex carbohydrates (like rice, roots and tubers), (ii) breast milk or dairy products, (iii) meats or eggs, (iv) beans, (v) vitamin-A-rich fruits and vegetables, and (vi) other fruits or vegetables; (2) food adequacy (yes/no) was calculated based on the minimum food diversity, minimum frequency and proper consistency indicators. Minimum frequency and proper consistency were considered when a 6-month-old child received solid, semi-solid, or soft foods once a day whether in a mashed consistency or in chunks; and when a 7–11-month-old child received solid, semi-solid, or soft foods twice a day whether in a mashed consistency or in chunks.
Data analysesStata software (version 14.1) was used to conduct the statistical analyses. Firstly, a descriptive analysis explored ultra-processed food (UPF) consumption (i.e. the consumption of at least one UPF assessed) and computed the proportion of UPFs as well as its distribution across the levels of covariates. In order to test the hypothesis that breastfeeding might influence UPF consumption we analyzed the four UPF groups by type of feeding (breastfed or not breastfed).
Secondly, the individualized effect of the covariables on the outcome was evaluated by multiple Poisson regression with a robust variance. Poisson regression has been described to be the adequate alternative for analyzing cross-sectional studies with binary outcomes.16
Thirdly, the covariates were grouped into three blocks of increasingly proximal influence with the outcome. A statistical hierarchical modeling was used to select variables for inclusion in the regression model following the theoretical model presented in Fig. 1.
Initially, a bivariate analysis was carried out to estimate the prevalence ratio (PR) and confidence intervals (95% CI) for each covariate and outcome (step 1). Covariates with p<0.20 were included in the multiple internal analysis of each block (step 2). In block 2, none of the covariates met the inclusion criteria for step 2 (p<0.20), and in this case maternal age was chosen to represent this block and adjusted to the next step. Covariates with p<0.20 in an internal analysis of each block were used as control in step 3, as follows. The proxy for socioeconomic status (maternal education level) adjusted to infant's age was the first covariate to be included in the model and it was used as an adjustment for the other hierarchically inferior covariates. Similarly, covariates of the distal block (1), “Characteristics of health unit during the infant's follow-up” were the second covariates to be included in the model and were used as an adjustment for the hierarchically inferior covariates. Analogously, the covariates of the intermediate block (2), “Family and Maternal characteristics”, which met the inclusion criteria of the multivariate model after adjusting for the distal block, became the control for the subsequent block. A similar procedure was adopted to analyze the proximal block (3), “Child characteristics and feeding practices”. The selected covariates were maintained in the model despite having lost statistical significance after the inclusion of the inferior blocks. After adjusting for the covariates of the same block and the superior blocks, the correlation between the covariates and the outcome was considered significant by adopting a significance level of 5% (p<0.05).
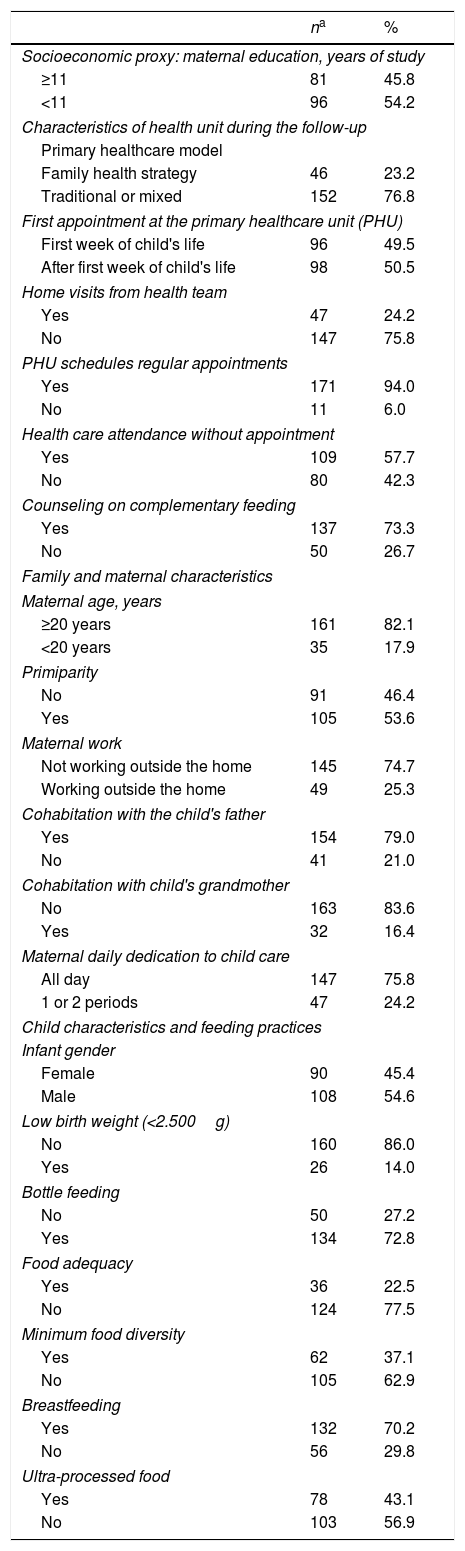
ResultsWe interviewed 198 mothers of children aged between 6 and 12 months. Most mothers (54.2%) had less than 11 years of schooling, 54.6% of the children were male, and the most frequent primary healthcare model was the traditional/mixed (76.8%). Considering feeding practices, 70.2% had been breastfed in the last 24h, 37.1% had complementary feeding diversity, and only a quarter had complementary feeding adequacy (Table 1).
Population description by study variables. Embu das Artes, São Paulo, Brazil, 2015.
| na | % | |
|---|---|---|
| Socioeconomic proxy: maternal education, years of study | ||
| ≥11 | 81 | 45.8 |
| <11 | 96 | 54.2 |
| Characteristics of health unit during the follow-up | ||
| Primary healthcare model | ||
| Family health strategy | 46 | 23.2 |
| Traditional or mixed | 152 | 76.8 |
| First appointment at the primary healthcare unit (PHU) | ||
| First week of child's life | 96 | 49.5 |
| After first week of child's life | 98 | 50.5 |
| Home visits from health team | ||
| Yes | 47 | 24.2 |
| No | 147 | 75.8 |
| PHU schedules regular appointments | ||
| Yes | 171 | 94.0 |
| No | 11 | 6.0 |
| Health care attendance without appointment | ||
| Yes | 109 | 57.7 |
| No | 80 | 42.3 |
| Counseling on complementary feeding | ||
| Yes | 137 | 73.3 |
| No | 50 | 26.7 |
| Family and maternal characteristics | ||
| Maternal age, years | ||
| ≥20 years | 161 | 82.1 |
| <20 years | 35 | 17.9 |
| Primiparity | ||
| No | 91 | 46.4 |
| Yes | 105 | 53.6 |
| Maternal work | ||
| Not working outside the home | 145 | 74.7 |
| Working outside the home | 49 | 25.3 |
| Cohabitation with the child's father | ||
| Yes | 154 | 79.0 |
| No | 41 | 21.0 |
| Cohabitation with child's grandmother | ||
| No | 163 | 83.6 |
| Yes | 32 | 16.4 |
| Maternal daily dedication to child care | ||
| All day | 147 | 75.8 |
| 1 or 2 periods | 47 | 24.2 |
| Child characteristics and feeding practices | ||
| Infant gender | ||
| Female | 90 | 45.4 |
| Male | 108 | 54.6 |
| Low birth weight (<2.500g) | ||
| No | 160 | 86.0 |
| Yes | 26 | 14.0 |
| Bottle feeding | ||
| No | 50 | 27.2 |
| Yes | 134 | 72.8 |
| Food adequacy | ||
| Yes | 36 | 22.5 |
| No | 124 | 77.5 |
| Minimum food diversity | ||
| Yes | 62 | 37.1 |
| No | 105 | 62.9 |
| Breastfeeding | ||
| Yes | 132 | 70.2 |
| No | 56 | 29.8 |
| Ultra-processed food | ||
| Yes | 78 | 43.1 |
| No | 103 | 56.9 |
One hundred and eighty-one responses were registered for the analysis of UFP consumption. The prevalence of UPF consumption was 43.1% (i.e. consumption of at least one UPF assessed in the previous 24h) (Table 1). In the evaluation per groups of UPFs the highest prevalence of consumption was that of sandwich cookies/chocolates/candies (21.8%), followed by sugary beverages (20.0%) and instant noodles/chips/savory biscuits (18.5%). The least consumed UPF group was hamburgers and processed meats. The analysis by type of feeding showed that infants who were not breastfed tended to have higher UPF consumption compared to those who were being breastfed (53.8% vs 38.9%), but no statistical significance was found.
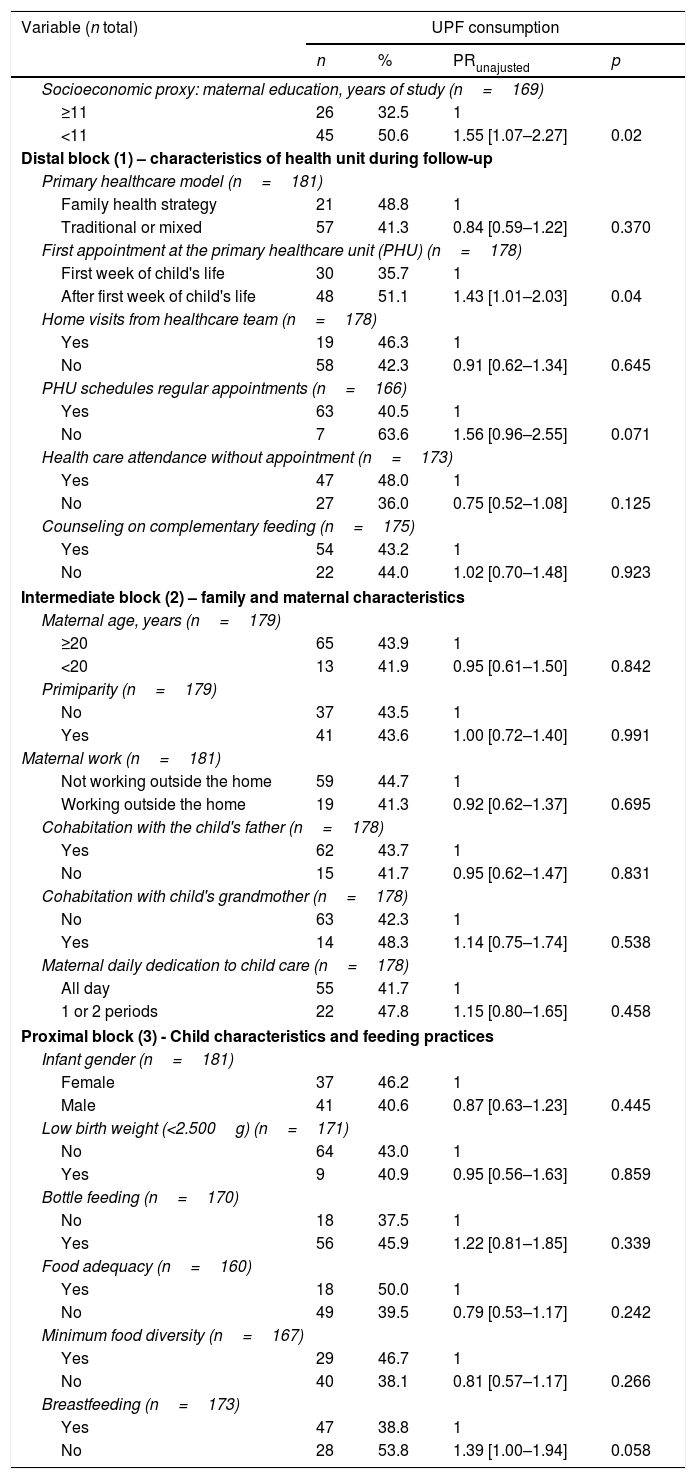
Table 2 presents the bivariate analysis. The highest prevalence of UPF consumption was observed among those infants whose mothers had lower education, infants who did not receive early assistance at the PHU, infants followed by a PHU that did not schedule appointments regularly, and infants who were not being breastfed in the previous 24h.
Bivariate Poisson analysis of ultra-processed food (UPF) consumption in infants aged between 6 and 12 months. Embu das Artes, São Paulo, Brazil, 2015.
| Variable (n total) | UPF consumption | |||
|---|---|---|---|---|
| n | % | PRunajusted | p | |
| Socioeconomic proxy: maternal education, years of study (n=169) | ||||
| ≥11 | 26 | 32.5 | 1 | |
| <11 | 45 | 50.6 | 1.55 [1.07–2.27] | 0.02 |
| Distal block (1) – characteristics of health unit during follow-up | ||||
| Primary healthcare model (n=181) | ||||
| Family health strategy | 21 | 48.8 | 1 | |
| Traditional or mixed | 57 | 41.3 | 0.84 [0.59–1.22] | 0.370 |
| First appointment at the primary healthcare unit (PHU) (n=178) | ||||
| First week of child's life | 30 | 35.7 | 1 | |
| After first week of child's life | 48 | 51.1 | 1.43 [1.01–2.03] | 0.04 |
| Home visits from healthcare team (n=178) | ||||
| Yes | 19 | 46.3 | 1 | |
| No | 58 | 42.3 | 0.91 [0.62–1.34] | 0.645 |
| PHU schedules regular appointments (n=166) | ||||
| Yes | 63 | 40.5 | 1 | |
| No | 7 | 63.6 | 1.56 [0.96–2.55] | 0.071 |
| Health care attendance without appointment (n=173) | ||||
| Yes | 47 | 48.0 | 1 | |
| No | 27 | 36.0 | 0.75 [0.52–1.08] | 0.125 |
| Counseling on complementary feeding (n=175) | ||||
| Yes | 54 | 43.2 | 1 | |
| No | 22 | 44.0 | 1.02 [0.70–1.48] | 0.923 |
| Intermediate block (2) – family and maternal characteristics | ||||
| Maternal age, years (n=179) | ||||
| ≥20 | 65 | 43.9 | 1 | |
| <20 | 13 | 41.9 | 0.95 [0.61–1.50] | 0.842 |
| Primiparity (n=179) | ||||
| No | 37 | 43.5 | 1 | |
| Yes | 41 | 43.6 | 1.00 [0.72–1.40] | 0.991 |
| Maternal work (n=181) | ||||
| Not working outside the home | 59 | 44.7 | 1 | |
| Working outside the home | 19 | 41.3 | 0.92 [0.62–1.37] | 0.695 |
| Cohabitation with the child's father (n=178) | ||||
| Yes | 62 | 43.7 | 1 | |
| No | 15 | 41.7 | 0.95 [0.62–1.47] | 0.831 |
| Cohabitation with child's grandmother (n=178) | ||||
| No | 63 | 42.3 | 1 | |
| Yes | 14 | 48.3 | 1.14 [0.75–1.74] | 0.538 |
| Maternal daily dedication to child care (n=178) | ||||
| All day | 55 | 41.7 | 1 | |
| 1 or 2 periods | 22 | 47.8 | 1.15 [0.80–1.65] | 0.458 |
| Proximal block (3) - Child characteristics and feeding practices | ||||
| Infant gender (n=181) | ||||
| Female | 37 | 46.2 | 1 | |
| Male | 41 | 40.6 | 0.87 [0.63–1.23] | 0.445 |
| Low birth weight (<2.500g) (n=171) | ||||
| No | 64 | 43.0 | 1 | |
| Yes | 9 | 40.9 | 0.95 [0.56–1.63] | 0.859 |
| Bottle feeding (n=170) | ||||
| No | 18 | 37.5 | 1 | |
| Yes | 56 | 45.9 | 1.22 [0.81–1.85] | 0.339 |
| Food adequacy (n=160) | ||||
| Yes | 18 | 50.0 | 1 | |
| No | 49 | 39.5 | 0.79 [0.53–1.17] | 0.242 |
| Minimum food diversity (n=167) | ||||
| Yes | 29 | 46.7 | 1 | |
| No | 40 | 38.1 | 0.81 [0.57–1.17] | 0.266 |
| Breastfeeding (n=173) | ||||
| Yes | 47 | 38.8 | 1 | |
| No | 28 | 53.8 | 1.39 [1.00–1.94] | 0.058 |
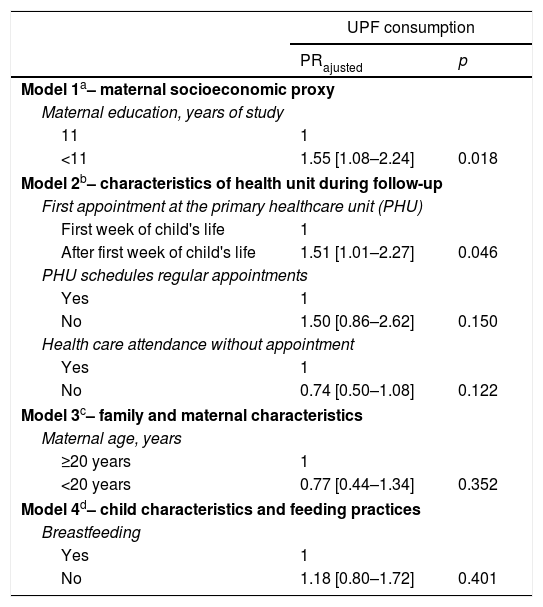
Hierarchical multivariate analysis indicated that lower maternal education and lack of early assistance at the primary health care – used in this study as proxies for socioeconomic status and performance of the PHU, respectively – were independent factors for UPF consumption (Table 3).
Multivariate Poisson regression models age-adjusted to identify the factors associated with ultra-processed food (UPF) consumption in infants aged between 6 and 12 months, following a hierarchical approach. Embu das Artes, São Paulo, Brazil, 2015.
| UPF consumption | ||
|---|---|---|
| PRajusted | p | |
| Model 1a– maternal socioeconomic proxy | ||
| Maternal education, years of study | ||
| 11 | 1 | |
| <11 | 1.55 [1.08–2.24] | 0.018 |
| Model 2b– characteristics of health unit during follow-up | ||
| First appointment at the primary healthcare unit (PHU) | ||
| First week of child's life | 1 | |
| After first week of child's life | 1.51 [1.01–2.27] | 0.046 |
| PHU schedules regular appointments | ||
| Yes | 1 | |
| No | 1.50 [0.86–2.62] | 0.150 |
| Health care attendance without appointment | ||
| Yes | 1 | |
| No | 0.74 [0.50–1.08] | 0.122 |
| Model 3c– family and maternal characteristics | ||
| Maternal age, years | ||
| ≥20 years | 1 | |
| <20 years | 0.77 [0.44–1.34] | 0.352 |
| Model 4d– child characteristics and feeding practices | ||
| Breastfeeding | ||
| Yes | 1 | |
| No | 1.18 [0.80–1.72] | 0.401 |
This study investigated complementary feeding practices among children aged 6–12 months living in a city of the metropolitan region of São Paulo, Brazil, focusing on the consumption of UPFs and its associated factors. Despite the increased interest in UPF intake, few studies were dedicated to identifying factors associated with it, especially among young children. Our study found that UPFs are largely consumed among children. The intake of UPF among children under 1 year of age was associated with lower maternal education and poor performance of PHUs.
According to WHO recommendations, infants should start receiving adequate complementary foods in addition to breast milk at 6 months of age. Complementary feeding practices that are not timely and adequate may result in poor outcomes related to the health and development of children.1 In our study, only a quarter of infants have met the food adequacy criterium, an indicator that summarizes three dimensions of optimum complementary feeding (frequency, consistency, and diversity); this demonstrates that we fall short of WHO recommendations and raises concerns about the quality of complementary feeding already verified in the literature.6
The early and high UPF consumption found in our study corroborates previous national and international studies.17–19 Our findings support the importance of understanding the role of UPF consumption as an early dietary determinant of chronic diseases, once evidence showed that inadequate complementary feeding influences the onset of obesity in children,4 and UPF consumption may lead to changes in the lipoprotein profile of children.20
Despite the fact that UPF consumption was more frequent among non-breastfed children, the statistical association was not found. Even though the relationship between UPF and breastfeeding has not been specifically studied, epidemiological findings indicate that breastfeeding is associated with a best profile of infant feeding.21,22 The non-association found between UPF consumption and breastfeeding practices in our study could potentially be due to stronger mediator confounding factors such as mother's education. In our study, higher educated mothers were less likely to offer UPFs to their infants, in the same way that evidence has shown that higher educated mothers are more likely to breastfeed,23 and breastfeeding babies have better a profile of infant feeding.21,22
The association between lower maternal education and higher UPF intake and other poor complementary feeding practices has been previously reported.8,24,25 A Brazilian national survey identified an association between low maternal education and a high frequency of consumption of unhealthy foods among children under one-year-old.8 Coelho et al.25 found that lower maternal education (<8 years), a lower income household and being enrolled in conditional cash transfer programs were factors that increased the intake of UPFs in children under 24 months of age. A higher maternal educational level can be correlated with higher family income, which can potentially facilitate the access to expensive foods such as vegetables and meat.26 On the other hand, the increase in UPF consumption in Brazil affects both lower and higher income populations.27
To our knowledge, this is the first time that the performance of PHUs is associated with UPF consumption. The performance of PHUs has been related to the improvement in infant mortality28 as well as to other infant feeding practice outcomes such as exclusive breastfeeding, introduction of complementary feeding and consumption of non-recommended food among infants.29,30 Our hypothesis to explain the association found in our study is that early care at PHUs in the first week of the infant's life may be an indicator of the family's bond with the healthcare team. The bond between the family and the PHUs allows professionals to be better acquainted with their patients as well as with the individuals’ priorities, thus facilitating access and improving the quality of the assistance delivered.11 This early assistance is considered a good time to encourage and to assist families with breastfeeding difficulty, immunizations, and neonatal screening, as well as to establish or strengthen the family's support network, including the relationship with the PHU.15 It is important to acknowledge that another covariable related to the performance of PHUs that investigated “counseling on complementary feeding” was not significantly associated with the outcome, which may be related to memory bias.
Our study has the limitation of including a single municipality, thus limiting the generalizability of our findings. On the other hand, this type of study is useful to formulate new hypotheses about this subject. In addition, the data collection instrument did not allow the detailing of frequency and age of food introduction. On the other hand, the questionnaire has important advantages: it has an easy and quick application; it shows food intake markers with less chance of memory bias; and it has been used by health teams to monitor infant feeding indicators in PHUs in Brazil, thus allowing comparability with other studies and with data produced by the PHUs.14
Our study showed that higher maternal education and better performance of PHUs decrease UPF intake among children under 1 year of age, which informs some policy recommendations. First, effective interventions in the primary healthcare settings aiming to improve infant feeding practices should include strategies to strengthen the bond between mothers and caregivers, especially from a lower socioeconomic status. Second, healthcare professional counseling has a key role in listening and understanding the factors that influence mothers during the transition to child's complementary feeding. Third, a way forward is to strengthen the implementation of the national policy “Estratégia Amamenta e Alimenta Brasil”, which aims to promote continuing education for health professionals on breastfeeding and complementary feeding in primary health settings through a problem-posing methodology.13 Fourth, the need for a push to incorporate the Brazilian Food and Nutrition Surveillance System (SISVAN) as a routine in the primary health care in order to systematically monitor infant feeding indicators.
FundingSecretaria de Estado de Saúde de Mato Grosso – SES/MT.
Conflicts of interestThe authors declare no conflicts of interest.
We wish to thank Lucimeire de Sales Magalhães Brockveld (Health Secretariat of Embu das Artes, Brazil) for her unconditional support with the data collection; Regina Tomie Ivata Bernal (University of São Paulo) for her assistance with the sample calculation; and Milena Nardocci Fusco (School of Public Health, University of Montreal, Canada) for her contribution with the English revision. We also wish to thank the managers of the Health Secretariat of Embu das Artes and the staff of the Brazilian Ministry of Health for supporting the research project.
Please cite this article as: Relvas GR, Buccini GS, Venancio SI. Ultra-processed food consumption among infants in primary health care in a city of the metropolitan region of São Paulo, Brazil. J Pediatr (Rio J). 2019;95:584–92.
Study conducted at Universidade de São Paulo, Faculdade de Saúde Pública, Programa de Pós-Graduação Nutrição em Saúde Pública, São Paulo, SP, Brazil




