
The aim of this research was to examine the association between body mass index, physical activity, adherence to the Mediterranean diet, and health-related quality of life in a sample of Spanish adolescents.
MethodThe study involved 456 adolescents aged between 11 and 14 years. They completed questionnaires on the Mediterranean diet (KIDMED), physical activity (Physical Activity Questionnaire for Older Children [PAQ-C]), and quality of life (KIDSCREEN-27). Body mass index was calculated. Hierarchical linear regression analyses were used to determine whether health-related quality of life could be predicted by the measured variables. The variables were analyzed in a stepwise manner, with Mediterranean diet entered in the first step, body mass index in the second, and physical activity in the third.
ResultsMediterranean diet accounted for 4.6% of the variance in adolescent's health-related quality of life, with higher adherence to the Mediterranean diet predicting higher health-related quality of life-scores. Body mass index accounted for a further 4.1% of the variance, with a higher body mass index predicting lower health-related quality of life scores. Finally, physical activity explained an additional 11.3% of the variance, with a higher level of physical activity being associated with higher health-related quality of life scores. Together, these variables explained 20% of the variance in the adolescents’ health-related quality of life.
ConclusionsPhysical activity, body mass index, and adherence to the Mediterranean diet are important components to consider when targeting improvements in the health-related quality of life of adolescents, with physical activity representing the component with the greatest influence.
O objetivo desta pesquisa foi examinar a associação entre o índice de massa corporal, a atividade física, a adesão à dieta mediterrânea e a qualidade de vida relacionada à saúde em uma mostra de adolescentes espanhóis.
MétodoO estudo envolveu 456 adolescentes com idades entre 11 e anos. Eles preencheram questionários sobre a dieta mediterrânea (KIDMED), atividade física (Questionário de Atividade Física para Crianças mais velhas, PAQ-C) e qualidade de vida (KIDSCREEN-27). Foi calculado o índice de massa corporal. Análises de regressão linear hierárquica foram utilizadas para determinar se a qualidade de vida relacionada à saúde pode ser prevista pelas variáveis medidas. As variáveis foram introduzidas de forma gradual com a dieta mediterrânea na primeira etapa, índice de massa corporal na segunda etapa e atividade física na terceira.
ResultadosA dieta mediterrânea representou 4,6% da variância na qualidade de vida relacionada à saúde dos adolescentes, e uma maior adesão à dieta mediterrânea foi preditiva de maiores escores de qualidade de vida relacionada à saúde. O índice de massa corporal representou um adicional de 4,1% de variância, e um maior índice de massa corporal foi preditivo de menores escores de qualidade de vida relacionada à saúde. Por fim, a atividade física representou um adicional de 11,3% da variância, e um maior nível de atividade física foi associado a maiores escores de qualidade de vida relacionada à saúde. Juntas, essas variáveis representam 20% da variância na qualidade de vida relacionada à saúde dos adolescentes.
ConclusõesA atividade física, o índice de massa corporal e a adesão à dieta mediterrânea são importantes componentes para considerar ao visar melhorias na qualidade de vida relacionada à saúde dos adolescentes, sendo a atividade física o componente com maior influência.
During adolescence, cognitive, physical, psychological, and emotional changes take place that can affect health and well-being.1 Health-related quality of life (HRQoL) is a multi-dimensional construct that describes well-being in physical, psychological, and social terms.2
The World Health Organization estimates that 35 million children in developing countries are overweight or obese.3 Compared to healthy weight children and adolescents, those who are obese are more likely to develop several chronic diseases, such as an unhealthy lipid profile, insulin resistance, and metabolic syndrome.4 Also, evidence suggests that adolescents with excess weight report poor overall HRQoL relative to healthy weight adolescents.5
Levels of physical activity (PA) have been shown to decline during adolescence, making this an important life-stage during which to focus research.6 Some of the benefits of PA include reductions in blood cholesterol, hypertension, metabolic syndrome, obesity, and reduced risk of premature death in adolescents. Participation in PA can also be important for ensuring good mental health.7 More intense and frequent PA is associated with lower depression, tension, and fatigue in children and adolescents.8 Although few studies have investigated the relationship between PA and HRQoL in adolescents, some evidence exists relating high PA with high HRQoL.9
Establishing healthy nutritional behaviors is also important during adolescence, since the healthy nutrition practices established in this period often persist into adulthood.10 Following a Mediterranean diet (MD), characterized by high consumption of olive oil, fruits, vegetables, whole grains, moderate to high consumption of fish, moderate consumption of milk and dairy products, and low consumption of meat and meat products has been related with weight loss, reduced abdominal obesity and insulin resistance, and lower risk of diabetes mellitus and cardiovascular diseases. Only a few studies have investigated the association between MD and HRQoL in adults11 or adolescents,12 finding MD to be positively associated.
To gain a better understanding of HRQoL during adolescence, it is important to explore factors that predict it. The aim of this study was to examine the association between body mass index (BMI), PA, adherence to the MD, and HRQoL in a sample of Spanish adolescents. This study may provide evidence and a theoretical basis on which to develop strategies to improve the HRQoL of Spanish adolescents.
MethodsSubjectsParticipants were recruited from their schools to participate in this cross-sectional research. Between 2014 and 2015, there were 20,929 adolescents enrolled in schools across Granada. The study involved 456 adolescents aged between 11 and 14 years, of whom 235 were girls and 221, boys. Data were collected between March and May in 2014. Power analysis suggested that the study required a minimum sample of 378 adolescent to achieve sufficient power with a 95% confidence interval (α: 0.05; β: 0.2). Five of the 55 public schools in the city center of Granada (Spain) were randomly selected to participate in this research. All participating schools were in a medium-high socioeconomic area based on information contained in the Educational Project of the center or school. All adolescents from the five schools aged between 11 and 14 years (n=511) were invited to take part in this study. Of these, 480 agreed to participate and written informed consent was received from their parent or guardian. Twenty-four adolescents were excluded for failing to complete some element of testing, or because they failed to attend class on their testing day. Both the adolescents and their parents or guardians were informed of the objectives and methods of the study and told that they could withdraw at any time. Participants were instructed on how to complete the questionnaires and how to conduct the tests. All tests were conducted during the participants’ physical education lessons during school time. No incentives were provided to adolescents or parents. A research assistant was also on hand to provide guidance on the completion of questionnaires and conduct physical testing. Ethical approval was granted by the Ethics Committee of the University of Granada. The ethical principles of the Declaration of Helsinki for medical research were adhered to.
HRQoLTo assess HRQoL, the KIDSCREEN-27 questionnaire was used. This internationally validated instrument13 is applicable for healthy and chronically ill children and adolescents aged from 8 to 18 years. The KIDSREEN-27 consists of 27 items across five components (physical well-being, psychological well-being, autonomy and parent's relation, social support and peers, and school environment). Internal consistency of the subscales was between 0.81 and 0.84, and test-retest reliability ranged from 0.61 to 0.74.14 The responses were scored and analyzed according to standard algorithms. The recommended syntax steps were performed, including transforming Rasch person parameter estimates into z-values, yielding scale scores as T-values with mean(±SD) scores of 50±10 define normality for children and adolescents aged 8–18 years across Europe. Higher scores indicate higher HRQoL.
Anthropometric measurementHeight and weight were measured following the protocols established by the International Society for the Advancement of Kinanthropometry15 using a stadiometer (GPM, Seritex, Inc., NJ, USA) with ±1mm accuracy) and an electronic scale model 707 (Seca®, MD, USA) with ±50g accuracy; BMI was calculated as weight divided by height squared (kg/m2). Overweight and obesity were defined according to international criteria.16
PA, maximal oxygen uptake, and screen timePA levels were evaluated using the Physical Activity Questionnaire for Older Children (PAQ-C). The questionnaire provides a general measure of PA for 8–20 year-olds. The PAQ-C is a self-administered questionnaire consisting of nine items rated on a five-point scale. The final PAQ-C activity summary score was calculated from the mean of the nine items. Five was therefore the highest possible score and one the lowest, with a score of five indicating high PA and one indicating low PA. Respondents are asked to recall the frequency and type of PA they have engaged in on each of the seven days prior to completing the questionnaire. Validation studies have found the PAQ-C to be highly reliable.17 Based on these scores, the sample was classified into PA tertiles (low, medium, and high).
Maximal oxygen uptake (VO2max) was estimated using a 20m incremental-maximum effort shuttle run field test. The test involves running to and fro between two lines placed 20m apart. Participants start at an initial velocity of 8.5km/h and increase their speed by 0.5km/h/min until they can no longer reach the line on two consecutive occasions or when the participant can no longer maintain the physical effort required to continue. VO2max relative to body mass (mL/kg/min) was calculated using the established formula.18
To determine sedentary screen time, participants were asked to report the number of hours per day they spent watching TV/DVDs, computer screens, smartphones, tablets, or other devices.
Adherence to the MDAdherence to the MD was assessed using the Evaluation of the Mediterranean Diet Quality Index (KIDMED),19 which was created to estimate adherence to the MD in children and young adults. The test is comprised of 16 dichotomous items (yes/no), of which twelve items describe behaviors consistent with the MD, e.g., “do you use olive oil at home?” and four items describe behaviors inconsistent with the MD, e.g., “do you consume sweets and candy several times every day?” Affirmative answers to MD-consistent and inconsistent behaviors were scored +1 and −1, respectively, giving a maximum possible score of 12. According to the KIDMED score, children's diets were classified as optimal (≥8 points), in need of improvement (4–7 points), or low quality (≤3 points).
Statistical analysisMeans and standard deviations are reported for all variables. Normality of the data was tested using the Kolmogorov–Smirnov test with the Lilliefors correction and homoscedasticity was assessed using the Levene test. After verifying that the variables were not normally distributed, the data were analyzed using the Mann–Whitney U-test for two-group comparison and the Kruskal–Wallis test for three-group comparisons. Hierarchical linear regression analyses were used to determine whether HRQoL in children could be predicted by the measured variables. MD was entered in a stepwise manner in the first step, BMI in the second step, and PA in the third step. The SPSS Statistics for Windows (IBM SPSS Statistics for Windows, version 22.0. NY, USA) was used to analyze the data with α set at 0.05.
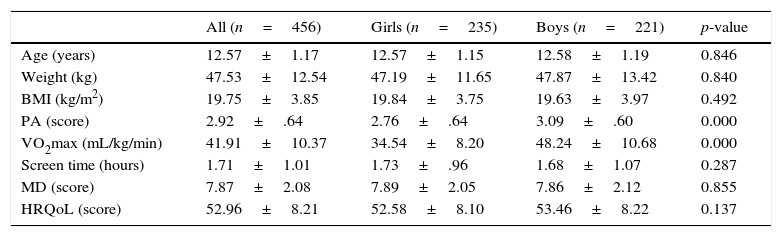
ResultsDescriptive characteristics for the study sample are shown in Table 1. The Mann–Whitney U-test showed that reported scores for PAQ-C and VO2max were significantly lower in girls than in boys. No significant differences were found for the other variables.
Baseline characteristics of adolescents.
| All (n=456) | Girls (n=235) | Boys (n=221) | p-value | |
|---|---|---|---|---|
| Age (years) | 12.57±1.17 | 12.57±1.15 | 12.58±1.19 | 0.846 |
| Weight (kg) | 47.53±12.54 | 47.19±11.65 | 47.87±13.42 | 0.840 |
| BMI (kg/m2) | 19.75±3.85 | 19.84±3.75 | 19.63±3.97 | 0.492 |
| PA (score) | 2.92±.64 | 2.76±.64 | 3.09±.60 | 0.000 |
| VO2max (mL/kg/min) | 41.91±10.37 | 34.54±8.20 | 48.24±10.68 | 0.000 |
| Screen time (hours) | 1.71±1.01 | 1.73±.96 | 1.68±1.07 | 0.287 |
| MD (score) | 7.87±2.08 | 7.89±2.05 | 7.86±2.12 | 0.855 |
| HRQoL (score) | 52.96±8.21 | 52.58±8.10 | 53.46±8.22 | 0.137 |
Data shown as mean±SD.
BMI, body mass index; PA, physical activity; VO2max, maximal oxygen uptake; MD, Mediterranean diet; HRQoL, health-related quality of life.
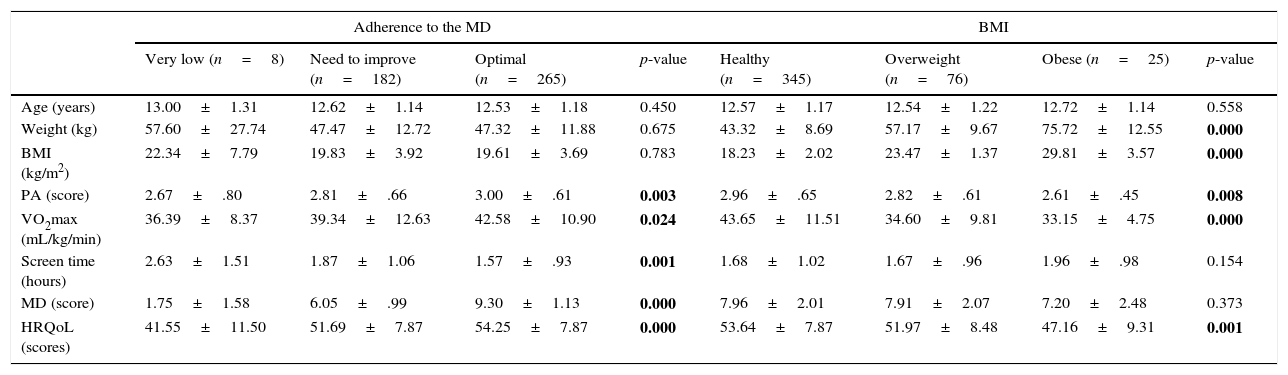
Table 2 shows the descriptive characteristics of the sample according to adherence to the MD, BMI, and PA. Analysis according to adherence to the MD revealed significant differences for PA, VO2max, and HRQoL, with higher MD adherence showing a positive relationship in all cases. Adolescents with higher adherence to the MD also reported lower screen time. Analysis according to BMI showed significantly higher values of PA, VO2max, and HRQoL in healthy weight adolescents in comparison with overweight or obese adolescents. In terms of PA, adolescents who engaged in more PA presented significantly higher VO2max, adherence to the MD, and HRQoL, as well as significantly lower weight, BMI, and screen time.
Characteristic of the adolescents by adherence to the Mediterranean diet, body mass index, and physical activity.
| Adherence to the MD | BMI | |||||||
|---|---|---|---|---|---|---|---|---|
| Very low (n=8) | Need to improve (n=182) | Optimal (n=265) | p-value | Healthy (n=345) | Overweight (n=76) | Obese (n=25) | p-value | |
| Age (years) | 13.00±1.31 | 12.62±1.14 | 12.53±1.18 | 0.450 | 12.57±1.17 | 12.54±1.22 | 12.72±1.14 | 0.558 |
| Weight (kg) | 57.60±27.74 | 47.47±12.72 | 47.32±11.88 | 0.675 | 43.32±8.69 | 57.17±9.67 | 75.72±12.55 | 0.000 |
| BMI (kg/m2) | 22.34±7.79 | 19.83±3.92 | 19.61±3.69 | 0.783 | 18.23±2.02 | 23.47±1.37 | 29.81±3.57 | 0.000 |
| PA (score) | 2.67±.80 | 2.81±.66 | 3.00±.61 | 0.003 | 2.96±.65 | 2.82±.61 | 2.61±.45 | 0.008 |
| VO2max (mL/kg/min) | 36.39±8.37 | 39.34±12.63 | 42.58±10.90 | 0.024 | 43.65±11.51 | 34.60±9.81 | 33.15±4.75 | 0.000 |
| Screen time (hours) | 2.63±1.51 | 1.87±1.06 | 1.57±.93 | 0.001 | 1.68±1.02 | 1.67±.96 | 1.96±.98 | 0.154 |
| MD (score) | 1.75±1.58 | 6.05±.99 | 9.30±1.13 | 0.000 | 7.96±2.01 | 7.91±2.07 | 7.20±2.48 | 0.373 |
| HRQoL (scores) | 41.55±11.50 | 51.69±7.87 | 54.25±7.87 | 0.000 | 53.64±7.87 | 51.97±8.48 | 47.16±9.31 | 0.001 |
| PA (tertiles) | ||||
|---|---|---|---|---|
| Low (n=150) | Mid (n=154) | High (n=151) | p-value | |
| Age (years) | 12.93±1.14 | 12.53±1.16 | 12.26±1.11 | 0.000 |
| Weight (kg) | 50.42±12.90 | 48.06±13.61 | 44.07±10.10 | 0.000 |
| BMI (kg/m2) | 20.45±4.22 | 19.90±4.21 | 18.87±2.86 | 0.003 |
| PA (score) | 2.21±.32 | 2.92±.18 | 3.63±.31 | 0.000 |
| VO2max (mL/kg/min) | 37.17±8.46 | 42.18±10.15 | 46.19±10.52 | 0.000 |
| Screen time (hours) | 1.84±.99 | 1.77±1.03 | 1.51±1.00 | 0.002 |
| MD (score) | 7.40±2.06 | 7.93±2.15 | 8.26±1.95 | 0.001 |
| HRQoL (scores) | 49.70±7.48 | 52.48±8.21 | 56.83±7.19 | 0.000 |
Data shown as mean±SD.
BMI, body mass index; PA, physical activity; VO2max, maximal oxygen uptake; MD, Mediterranean diet; HRQoL, health-related quality of life. bold: significant differences.
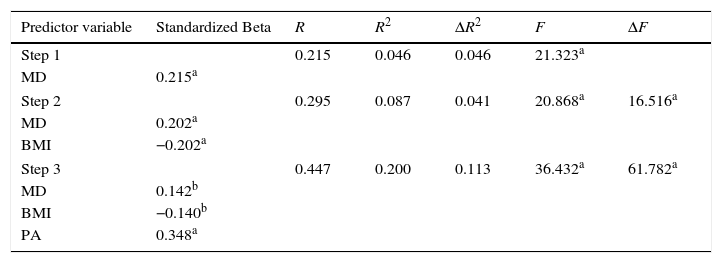
Table 3 presents results from the hierarchical regression. MD accounted for 4.6% of the variance in adolescent's HRQoL. Higher adherence to the MD was associated with higher HRQoL scores. BMI accounted for a further 4.1% of the variance, with a higher BMI predicting lower HRQoL among adolescents. Finally, PA explained an additional 11.3% of the variance in adolescent's HRQoL, with a higher level of PA being associated with higher HRQoL scores. Together, these variables explained 20% of the variance in the adolescents’ HRQoL.
Factors associated with health-related quality of life (total score) in children – multiple hierarchical regression analysis (n=456).
| Predictor variable | Standardized Beta | R | R2 | ΔR2 | F | ΔF |
|---|---|---|---|---|---|---|
| Step 1 | 0.215 | 0.046 | 0.046 | 21.323a | ||
| MD | 0.215a | |||||
| Step 2 | 0.295 | 0.087 | 0.041 | 20.868a | 16.516a | |
| MD | 0.202a | |||||
| BMI | −0.202a | |||||
| Step 3 | 0.447 | 0.200 | 0.113 | 36.432a | 61.782a | |
| MD | 0.142b | |||||
| BMI | −0.140b | |||||
| PA | 0.348a | |||||
BMI, body mass index; PA, physical activity; MD, Mediterranean diet.
To the authors’ knowledge, this is the first study to analyze the association between a combination of adherence to MD, BMI, and PA on HRQoL during the first stage of adolescence. The main finding of the present study is that healthy lifestyle behaviors are reasonably good predictors of HRQoL during adolescence (together accounting for 20% of the variance). In addition, the strongest measured predictor of HRQoL was PA, which explained 11.3% of the variance, more than adherence to MD and BMI combined.
Few studies have studied the association between adherence to the MD and HRQoL. Previous studies in adults have found self-perceived mental and physical function to be directly associated with adherence to the MD.11 During the period of adolescence, only one recent study conducted in Greece has revealed a significant positive association between adherence to the MD and HRQoL (Beta=0.210).12 Consuming a MD has been inversely associated with various chronic diseases.20 Furthermore, adolescents who do not typically consume a MD tend to have a lower socioeconomic status.19 As a result, they tend to have less access to some of the healthy components of the MD, such as fruits, vegetables, fish, or olive oil. Lower socioeconomic status has been associated with poorer physical and general health.21 Considering that the majority of the present sample lived in medium-high socioeconomic areas, these factors are unlikely have exerted a large influence on the findings. Individuals following a MD are also more likely to engage in other aspects of the Mediterranean lifestyle, such as using lunchtime for social communication with family and friends. This may at least partially explain the relationships between adherence to the MD and social aspects of the HRQoL.
The results regarding BMI and HRQoL are controversial. This study found a higher BMI to be related with lower HRQoL. Previous studies comparing pediatric HRQoL across different BMI weight categories of adolescents have not found significant differences according to weight category.22 In contrast, other studies have found that obese adolescents have lower HRQoL than healthy weight adolescents.23 Many overweight adolescents may experience weight-related stigma and social discrimination as a result of carrying excess weight, which could diminish their HRQoL.24
The present study also identified high levels of PA to be related to high HRQoL, in congruence with other published research.25 One previous prospective study showed a bidirectional association between PA and HRQoL in adolescents in which total PA engagement strongly predicted high HRQoL, and positive HRQoL predicted engagement in recommended PA levels.26 This may be a result of the positive influence of PA on psychological and social functioning, and protection from depression.27
PA had a stronger influence than adherence to the MD and BMI and should be considered as the main focus of intervention targeting HRQoL in adolescents. A recent intervention study involving overweight and obese adolescents investigated correlations between changes in HRQoL and BMI or PA after a 24-month weight-loss program. Results showed that long-term changes in PA explained 30% of the variation in overall HRQoL (p=.01), whereas changes in BMI were not associated with a change in HRQoL. This indicates that PA may have a positive influence on HRQoL even without a substantial change in body composition.28
One limitation of the present research is its cross-sectional design, which inhibits the investigation of causal relationships. Furthermore, the use of self-report to assess a number of the variables increases the possibility of measurement error. However, as both the PAQ-C and KIDMED have previously demonstrated high validity and reliability in this population, this should have little impact on the conclusions made. Also, it was not possible to evaluate the socioeconomic status (SES) of individuals in the study. All schools were situated in a medium-high socioeconomic area based on information contained in the Educational Project of the center or school. As a result, the schools should at least be comparable; however, future studies should measure SES where possible.
Despite these limitations, to the best of the authors’ knowledge, this is the first study to analyze associations between MD adherence, PA, and BMI on HRQoL in adolescents.
This study suggests that PA, BMI, and adherence to the MD are important components to consider when targeting improvements in the HRQoL of adolescents, with PA representing the component with the greatest influence. Policies that promote the MD and recommend PA are expected to improve HRQoL in adolescents. Longitudinal studies are needed to further explore the association between these components with regards to HRQoL.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Muros JJ, Pérez FS, Ortega FZ, Sánchez VM, Knox E. The association between healthy lifestyle behaviors and health-related quality of life among adolescents. J Pediatr (Rio J). 2017;93:406–12.




