

To assess the protective effect of exclusive breastfeeding and the effectiveness of maternal vaccination in reducing pertussis-like illness.
MethodThis was a case-control study conducted in sentinel hospitals for pertussis in Recife between July 2016 and July 2018. Cases included children aged under six months with symptoms compatible with pertussis (pertussis-like illness). Controls included children aged under six months, living in the metropolitan region of Recife with no diagnosis of pertussis-like illness and matched by the same hospital and birth date.
ResultsSeventy-three cases and 194 controls were included. The diagnosis of pertussis-like illness was predominantly clinical (97,2%). Amongst the main symptoms, paroxysmal cough was observed in 95.89% of cases and vomiting in 53.4%. There were 29 hospitalized cases and no deaths. Out of the 73 cases, 47 were born to mothers vaccinated against pertussis during pregnancy, and the mothers of 144 of the 194 controls had been vaccinated. The protective effect of breastfeeding was of 74% (95% CI;38%, 89%). Children younger than six months, who were exclusively breastfed and with mothers vaccinated against pertussis during pregnancy were 5 times less likely to develop pertussis-like illness, corresponding to a protection of 79% (95% CI;31%, 94%). The effectiveness of maternal vaccination against pertussis-like illness in children under six months was low (27%) and not statistically significant (CI 95%; −34% a 60%).
ConclusionsExclusive breastfeeding protects children under six months from pertussis-like illness and may be enhanced when associated with maternal vaccination. These strategies should be encouraged because they also protect against pertussis-like illnesses.
Pertussis is a highly contagious respiratory infection caused by Bordetella pertussis, also known as a long cough, which affects the respiratory tract and has a paroxysmal dry cough as its main clinical characteristic.1–3 Children and adults of all age groups may develop the disease4m although it is more severe in infants aged less than one year, at risk of complications, hospitalization and death.4,5
However, its clinical presentation is variable, and many patients may present similar or atypical symptoms, especially small babies. In these cases, the term pertussis-like illness (PLI) has been used for a clinical diagnosis in children who present signs compatible with pertussis, with no history of exposure to a confirmed case or in the absence of etiological confirmation.6
Currently, the Brazilian Ministry of Health's National Immunization Program (PNI) recommends the whole cell pertussis vaccine (Pw) as one of the components of the Pentavalent vaccine for children at two months of age, and then repeated at four and six months of age.1,7 Reinforcements are recommended by PNI with the triple bacterial vaccine at 15 months and 4 years of age1. Despite the good vaccination coverage, there has been a worldwide increase in the incidence of pertussis3 and several strategies have been proposed with the purpose of reducing the incidence of infection, especially in the first months of life, where the disease tends to be more severe and fatal.6–8
The strategy of vaccinating pregnant women in order to protect the newborn through the passage of antibodies as a transplacental route has been shown to be more promising, and has even been approved by the World Health Organization (WHO), the Advisory Committee Immunizations Practices (ACIP) – USA, the American college of obstetricians and Gynecologist, the American Academy of Pediatricians of the USA and the Technical Advisory Committee on Immunizations (CTAI).6–8 The recommendation of these institutions is the vaccination of all pregnant women during each pregnancy with the triple bacterial acellular (Tdap), from the 27th to the 36th gestational week in order to reduce morbidity and mortality in children younger than six months.7–10
In Brazil, the recommendations of the Ministry of Health (MH) was updated based on the reference protocols for pertussis in the United Kingdom,8 which recommends the triple bacterial acellular for pregnant women between the 20th and 36th weekly that should be repeated for every pregnancy.7 The vaccine, in this period, ensures the transfer of high and sufficient levels of antibodies against pertussis through the placenta, providing passive immunity to the fetus and resulting in the protection of the newborn until the vaccine regimen against pertussis is complete.7–9,11–14 After this period, the vaccine does not offer an adequate level of antibodies sufficient for the passive protection of the child.14
The exclusive breastfeeding strategy (EBF) continues to be encouraged for providing all fluids, nutrients and energy exclusively through breast milk during the first six months of life, with no formulas or other dietary supplements.15 WHO and MH have recommended that breastfeeding should be exposed in the delivery room during the first hour of life and maintained in the form of exclusive breastfeeding, without the addition of any type of solid, semi-solid or liquid food during the first six months of life. In the after period, it should be continued in conjunction with complementary feeding until the second year of life or more.15,16 EBF in addition to being an important protective factor against various pathologies, due to nonspecific anti-infectious factors and specific protective immunoglobulins in its composition,10,12 is highly beneficial. This is shown especially in relation to infant morbidity and mortality when associated with fewer episodes of diarrhea, acute respiratory changes and other infectious diseases.15 No other strategy achieves the same impact as exclusive breastfeeding on reducing mortality in children aged under six months.15
Studies show the effectiveness of vaccination in pregnant women in the protection of pertussis in children younger than two months.17–21 However, the vaccine has not yet shown to be enough to eradicate the infection. In this sense, children diagnosed with pertussis may have passively received, via the transplacental route and breast milk, enough immunity to reduce the typical symptoms of pertussis. Therefore, this study aims to evaluate the protective effect of exclusive breastfeeding and the effectiveness of maternal vaccination in reducing PLI in children under six months of age, from July 2016 to July 2018, in the Metropolitan Region of Recife, Brazil.
MethodsA case-control study was conducted in the Metropolitan Region of Recife (RMR) between July 2016 and July 2018. All children aged under six months diagnosed with a clinical syndrome compatible with pertussis infection with no history of exposure to a confirmed case or in the absence of etiological confirmation6 were included in the study. This definition corresponds to the definition of cases clinically confirmed by the Brazilian Ministry of Health, which includes children aged under six months with a cough of any type for 10 days or more, associated with one or more of the following symptoms: paroxysmal cough, inspiratory whoop, post-vomiting cough, cyanosis, apnea or choking1.<-- --> The controls were defined as children aged under six months, living in the metropolitan region of Recife, with no diagnosis of PLI (matched by the same maternity hospital and date of birth+or ˗ 2 days), and who presented no characteristic symptoms of PLI and did not become a case and were not notified as cases to SINAN. Data were collected from medical records acquired at the Medical and Statistical Archive Service of the participating maternity hospitals. In maternity hospitals where the number of control babies born on the same date of the case was insufficient, control babies were recruited within two days of the date of birth.
Health professionals from the epidemiology centers of the study hospitals were responsible for collecting nasopharynx secretion for pertussis and filling out the records of the National Notifiable Disease Surveillance System (SINAN). The samples were sent to the Central Laboratory of Pernambuco (LACEN-PE) for analysis.
Immunocompromised babies with congenital diseases, chronic respiratory diseases that develop cough or using coughing drugs and other respiratory infections were excluded.
The sample size was calculated by estimating the efficacy of maternal vaccination of 93%17 and a vaccination coverage of 71.5%. An alpha error of 0.05 and a power of 0.95 were calculated by EPIINFO.22 The ratio of four controls per case was used. A minimum sample size of 40 cases and 160 controls was estimated. Seventy-three cases and 194 controls were included in the study.
The main exposures were pertussis vaccination (Tdap) during pregnancy and breastfeeding, information that was obtained from maternal vaccination card records or medical records. The following variables were also obtained from the medical records: mother's age, schooling, number of prenatal consultations, type of delivery, place of residence, sex of the baby, birth weight, exclusive breastfeeding, gestational age at birth and vaccination of babies.
Only children of women whose vaccination status was known were included in the study. Mothers with Tdap registered on the current vaccination card administered in the previous period (postpartum, previous or last pregnancy) were classified as non-vaccinated.
A composite variable was constructed based on breastfeeding and maternal vaccination and stratified into four levels: not vaccinated and not exclusively breastfed for six months, not vaccinated and exclusively breastfed for six months, vaccinated and not exclusively breastfed for six months and vaccinated and exclusively breastfed for six months.
To test the association between the independent variables and the outcome we estimated the OR, the respective confidence interval and the p-value. The analysis was performed using conditional logistic regression with STATA 14.23 Maternal vaccination, breastfeeding (main exposures) and the variables that presented a p-value <0,20 in the bivariate analysis (potential confounders) were introduced into the multivariate model (Table 1). Maternal vaccination, breastfeeding (main exposures) and variables with p-value <0,10 remained in the final model (Table 2). The efficacy of vaccinating pregnant women in reducing PLI in children aged under six months was estimated by calculating 1 - OR×10020 (Table 3).
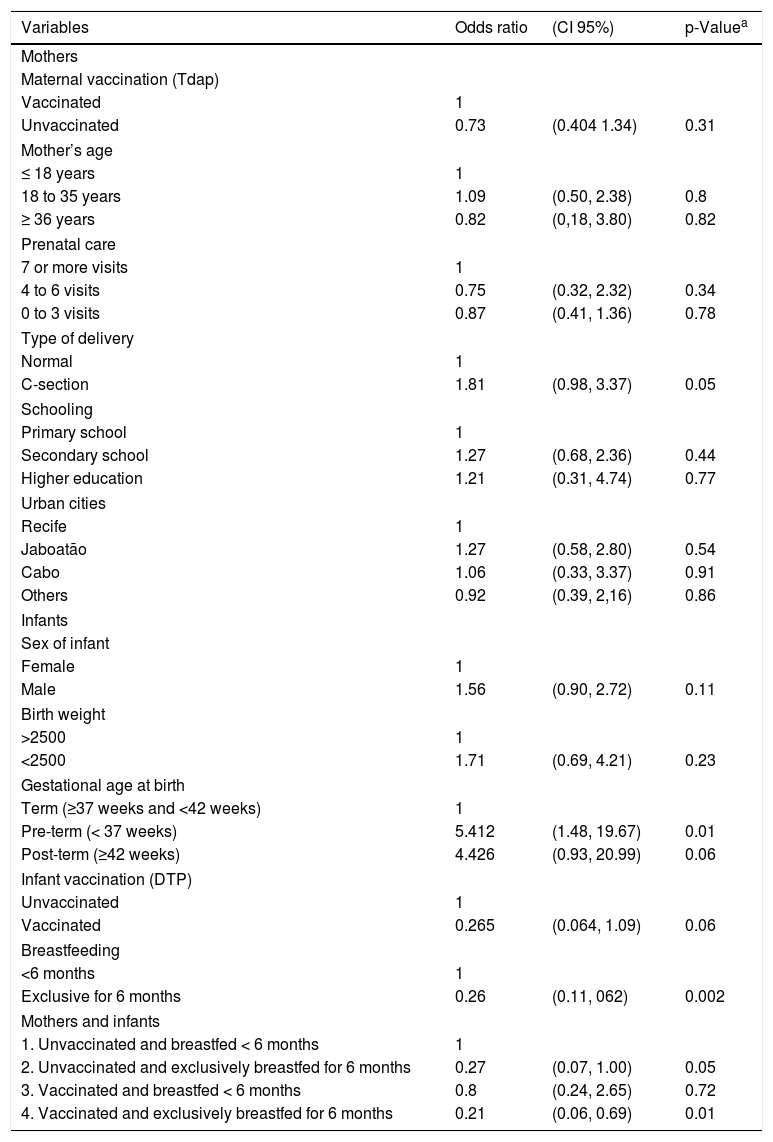
The univariate analysis of the association between pertussis-like illness, maternal vaccination and potential confounders in infants aged under six months born in the Metropolitan Region of Recife from July 2016 to July 2018.
| Variables | Odds ratio | (CI 95%) | p-Valuea |
|---|---|---|---|
| Mothers | |||
| Maternal vaccination (Tdap) | |||
| Vaccinated | 1 | ||
| Unvaccinated | 0.73 | (0.404 1.34) | 0.31 |
| Mother’s age | |||
| ≤ 18 years | 1 | ||
| 18 to 35 years | 1.09 | (0.50, 2.38) | 0.8 |
| ≥ 36 years | 0.82 | (0,18, 3.80) | 0.82 |
| Prenatal care | |||
| 7 or more visits | 1 | ||
| 4 to 6 visits | 0.75 | (0.32, 2.32) | 0.34 |
| 0 to 3 visits | 0.87 | (0.41, 1.36) | 0.78 |
| Type of delivery | |||
| Normal | 1 | ||
| C-section | 1.81 | (0.98, 3.37) | 0.05 |
| Schooling | |||
| Primary school | 1 | ||
| Secondary school | 1.27 | (0.68, 2.36) | 0.44 |
| Higher education | 1.21 | (0.31, 4.74) | 0.77 |
| Urban cities | |||
| Recife | 1 | ||
| Jaboatão | 1.27 | (0.58, 2.80) | 0.54 |
| Cabo | 1.06 | (0.33, 3.37) | 0.91 |
| Others | 0.92 | (0.39, 2,16) | 0.86 |
| Infants | |||
| Sex of infant | |||
| Female | 1 | ||
| Male | 1.56 | (0.90, 2.72) | 0.11 |
| Birth weight | |||
| >2500 | 1 | ||
| <2500 | 1.71 | (0.69, 4.21) | 0.23 |
| Gestational age at birth | |||
| Term (≥37 weeks and <42 weeks) | 1 | ||
| Pre-term (< 37 weeks) | 5.412 | (1.48, 19.67) | 0.01 |
| Post-term (≥42 weeks) | 4.426 | (0.93, 20.99) | 0.06 |
| Infant vaccination (DTP) | |||
| Unvaccinated | 1 | ||
| Vaccinated | 0.265 | (0.064, 1.09) | 0.06 |
| Breastfeeding | |||
| <6 months | 1 | ||
| Exclusive for 6 months | 0.26 | (0.11, 062) | 0.002 |
| Mothers and infants | |||
| 1. Unvaccinated and breastfed < 6 months | 1 | ||
| 2. Unvaccinated and exclusively breastfed for 6 months | 0.27 | (0.07, 1.00) | 0.05 |
| 3. Vaccinated and breastfed < 6 months | 0.8 | (0.24, 2.65) | 0.72 |
| 4. Vaccinated and exclusively breastfed for 6 months | 0.21 | (0.06, 0.69) | 0.01 |
CI, confidence interval.
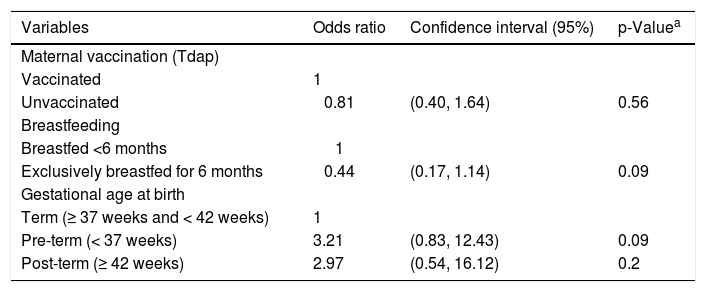
The multivariate analysis of the association between pertussis-like illness, maternal vaccination, and potential confounders in infants aged under six months born in the Metropolitan Region of Recife from July 2016 to July 2018.
| Variables | Odds ratio | Confidence interval (95%) | p-Valuea |
|---|---|---|---|
| Maternal vaccination (Tdap) | |||
| Vaccinated | 1 | ||
| Unvaccinated | 0.81 | (0.40, 1.64) | 0.56 |
| Breastfeeding | |||
| Breastfed <6 months | 1 | ||
| Exclusively breastfed for 6 months | 0.44 | (0.17, 1.14) | 0.09 |
| Gestational age at birth | |||
| Term (≥ 37 weeks and < 42 weeks) | 1 | ||
| Pre-term (< 37 weeks) | 3.21 | (0.83, 12.43) | 0.09 |
| Post-term (≥ 42 weeks) | 2.97 | (0.54, 16.12) | 0.2 |
This study was approved by the Oswaldo Cruz Hospital Ethics Committee, CAAE: 83156018.9.0000.5192, Pernambuco, Brazil.
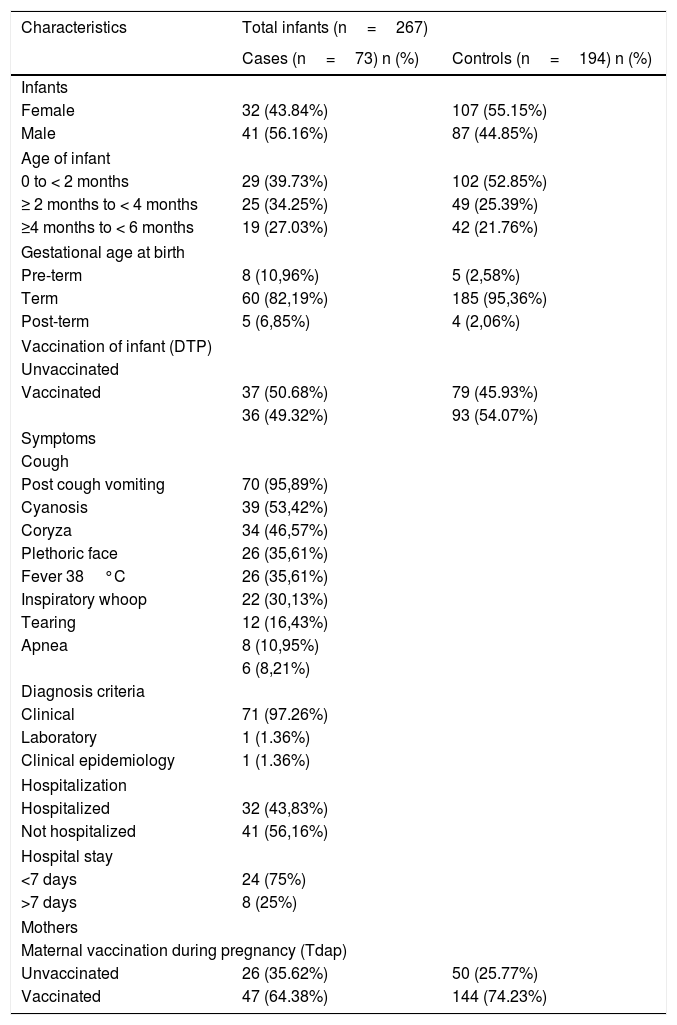
ResultsWe identified 108 PLI cases potentially eligible for the study. Of these, 35 were excluded. Twenty-four cases were excluded due to a lack of information on the maternal vaccine and 11 in the controls, due to a lack of information on the maternal vaccine. In these situations, the match was not possible. Out of the 432 controls, 60 were not included because they did not live in the MRR and 178 were not included because they did not present information on maternal vaccination. The sample totaled 73 cases and 194 controls. The distribution by gender, age group, maternal vaccination and childhood vaccination between cases and controls were similar. The diagnosis of Pertussis-Like Illness was predominantly clinical (97,2%) with 29 hospitalized cases and no deaths. Of the hospitalized cases, 24 children were hospitalized, at most for up to 7 days and 8 were hospitalized for more than 7 days. Amongst the main symptoms of PLI, paroxysmal cough was observed in 95.89% of cases. Inspiratory whoop was only present in 16.43% (Table 4). Prematurity was the only underlying disease found and was observed in 10.96% of cases and in 2.58% of controls (Table 4). Among the 73 cases, 47 were born to mothers who were vaccinated against pertussis during pregnancy and 144 out of 194 controls had their mother vaccinated (Table 4). In the univariate analysis, by conditional logistic regression, the following items were associated with the PLI: type of delivery, gestational age at birth, exclusive breastfeeding for six months and a composite variable that combines vaccination status and exclusive breastfeeding (Table 1).
Maternal vaccination status (Tdap) and characteristics of cases (pertussis-like illness) and controls aged under six months in the Metropolitan Region of Recife.
| Characteristics | Total infants (n=267) | |
|---|---|---|
| Cases (n=73) n (%) | Controls (n=194) n (%) | |
| Infants | ||
| Female | 32 (43.84%) | 107 (55.15%) |
| Male | 41 (56.16%) | 87 (44.85%) |
| Age of infant | ||
| 0 to < 2 months | 29 (39.73%) | 102 (52.85%) |
| ≥ 2 months to < 4 months | 25 (34.25%) | 49 (25.39%) |
| ≥4 months to < 6 months | 19 (27.03%) | 42 (21.76%) |
| Gestational age at birth | ||
| Pre-term | 8 (10,96%) | 5 (2,58%) |
| Term | 60 (82,19%) | 185 (95,36%) |
| Post-term | 5 (6,85%) | 4 (2,06%) |
| Vaccination of infant (DTP) | ||
| Unvaccinated | ||
| Vaccinated | 37 (50.68%) | 79 (45.93%) |
| 36 (49.32%) | 93 (54.07%) | |
| Symptoms | ||
| Cough | ||
| Post cough vomiting | 70 (95,89%) | |
| Cyanosis | 39 (53,42%) | |
| Coryza | 34 (46,57%) | |
| Plethoric face | 26 (35,61%) | |
| Fever 38°C | 26 (35,61%) | |
| Inspiratory whoop | 22 (30,13%) | |
| Tearing | 12 (16,43%) | |
| Apnea | 8 (10,95%) | |
| 6 (8,21%) | ||
| Diagnosis criteria | ||
| Clinical | 71 (97.26%) | |
| Laboratory | 1 (1.36%) | |
| Clinical epidemiology | 1 (1.36%) | |
| Hospitalization | ||
| Hospitalized | 32 (43,83%) | |
| Not hospitalized | 41 (56,16%) | |
| Hospital stay | ||
| <7 days | 24 (75%) | |
| >7 days | 8 (25%) | |
| Mothers | ||
| Maternal vaccination during pregnancy (Tdap) | ||
| Unvaccinated | 26 (35.62%) | 50 (25.77%) |
| Vaccinated | 47 (64.38%) | 144 (74.23%) |
aX2 Chi-square or Fisher’s tests 1.
Exclusive breastfeeding in children younger than six months born to unvaccinated mothers had a protective effect with OR of 0.27 (95% CI; 0.07, 1.00), while exclusive breastfeeding in children younger than six months born to vaccinated mothers had a protective effect with an OR of 0.21 (95% CI; 0.06, 0.69) (Table 1).
The multivariate model included maternal vaccination, exclusive breastfeeding and variables with p-value <0,20 (type of delivery, sex of infant, gestational age at birth, infant vaccination and breastfeeding) (Table 1). In the multivariate analysis, only the variables exclusive breastfeeding for six months (p=0.09) and gestational age at birth (p=0.09) presented a statistically significant association with PLI and remained in the final model (Table 2).
Among the 194 controls, 144 pregnant women were vaccinated against pertussis during pregnancy, determining a vaccination coverage of 74.2%.
The efficacy of maternal vaccination in reducing PLI in children younger than six months was 27% for univariate analysis* (Table 3).
DiscussionThe aim of this study developed in the metropolitan Recife region was to evaluate the protective effect of exclusive breastfeeding and the effectiveness of maternal vaccination in reducing PLI in children under six months of age. Exclusive breastfeeding for six months had a protective effect against PLI in children under six months of age, with a slight increase in this effect when associated with maternal vaccination. A result consistent with the absence or low effectiveness of maternal vaccination was observed; as the protective effect of exclusive breastfeeding and its potentiation when associated with maternal vaccination.
The effectiveness of vaccination of pregnant women in the reduction of PLI in children under six months of age was estimated at 27% (95% CI; −34%, 60%). A similar estimate has been reported in Australia, in which the efficacy of the vaccine to vaccinate pregnant women against pertussis in the protection of infants under six months was 39% (95% CI; −12%, 66%).24 The authors have suggested that the low efficacy of vaccination is due to the reduction of vaccine immunity in which protection is partially offered. Thus, the vaccine administered during pregnancy would protect children only against the severe form of pertussis, it doesn't prevent infection. However, studies report that the maternal vaccine is ineffective in preventing mild forms of the disease, as in cases classified as PLI.4,6,11,24–26 Low VE may also be associated with the presence of multiple Bordetella pertussis clones circulating in Brazil, or different strains used in vaccine production.4,13 Bacterial antigens are known for their virulence capacity and do not correspond to the antigenic profile of current vaccines.13 The Tdap vaccine may not have the expected efficacy against all strains circulating in the state of Pernambuco, which would explain the low efficacy observed in this study.
In Brazil, the pertussis vaccine used in pregnant women is composed of three antigens.7 The number of antigens that make up acellular pertussis vaccines could be another possible cause of low efficacy. Vaccines composed of 3 antigens (Td3ap) may be 5% less effective compared to those composed of 5 antigens (Td5ap).27 Studies conducted with acellular vaccines composed of 5 types of antigens showed high vaccine efficacy (82–91%) in infants under two months.17–20 However, those with an acellular vaccine composed of 3 antigens showed reduced vaccine efficacy for infants younger than two months (VE=69%) and for infants under six months (VE=39%).20 This result suggests that vaccines composed of fewer antigens produce a smaller range of specific antibodies and are, therefore, possibly less effective.
The frequency of maternal vaccination during pregnancy among the controls was 74.2%. This result is understood as the estimation of vaccination coverage (VC) in pregnant women against pertussis. However, it is lower than the percentage defined as adequate by the MH (VC≥95%).1
EBF during a period of six months offers children all the exact properties to meet their needs, adequately supplying their nutritional, metabolic and physiological deficiencies.15,16 Children who are exclusively breastfed are less likely to become ill because this strategy offers immunological and protective factors for infections, particularly respiratory and gastrointestinal.10,12,15,16 Early exposure to complementary foods, before six months of age, causes harm to children, increasing the risk of morbidity and mortality, since it makes them more susceptible to the development of diarrhea, infections and even malnutrition, compromising their growth and development.15,16
Breast milk in this study had a protective effect in children younger than six months against PLI and this effect of 74% was identified from exclusive breastfeeding for six months (95% CI; 38%, 89%). In addition to vaccination of pregnant women, WHO recommends exclusive breastfeeding for six months as part of its strategy to protect against various infectious diseases.14,15,28 Studies indicate that exclusive breast milk for six months, without formula or other dietary supplements, is a protective factor due to the presence of natural components or nonspecific anti-infecting factors and specific protective immunoglobulins (anti-PT sIgA) against pertussis.10,12,13,20 These components are protective enough because they neutralize the pathogenesis of Bordetella pertussis by inhibiting its adherence to the ciliated epithelium of the respiratory tract.10,12–14 This mechanism suggests that women are able to passively protect their babies both through serum (transplacental) and in a secretory way (breast milk).
In studies associating the pertussis vaccination strategy in pregnancy and breastfeeding, research has validated a significant increase in anti-PT sIgA immunoglobulin levels (2.56 IU/mg) in breast milk, in contrast to women without vaccination during pregnancy (0.96 IU/mg).12,13,18 These increased levels of anti-PT sIgA in the breast milk of vaccinated women can be observed up to eight weeks after delivery.10,14,28 This association suggests that children of mothers vaccinated and exclusively breastfed for six months may benefit from the additional protection offered by breast milk when compared to babies born to mothers who were not vaccinated during pregnancy.10,13,14,26
However, the increase in specific anti-pertussis antibodies (sIgA) in breast milk may also be related to previous maternal infection. Although disease-induced immunity is not permanent, it lasts from 4 to 20 years and may induce a specific immune response to pertussis.13,29 Although information on natural maternal infection is unavailable in SINAN or in the medical records, during the study period there was an outbreak of a pertussis epidemic, which makes it possible that these pregnant women had come into contact with this infectious agent. These data allow the hypothesis that pregnant women were infected and naturally immunized during the 2014 epidemic, leading to a distortion in the estimation of vaccine effectiveness.
Exclusive breastfeeding for six months in children born to unvaccinated mothers had a protective effect with an OR of 0.27 (95% CI; 0.07, 1.00), i.e., the chance of PLI in exclusively breastfed children is 3.7 times lower. However, exclusive breastfeeding for six months in children of vaccinated mothers had a protective effect with an OR of 0.21 (95% CI; 0.06; 0.69), i.e., 4.7 times lower. Children born to mothers vaccinated during pregnancy and exclusively breastfed will possibly present greater protection against PLI, since through exclusive breastfeeding specific antibodies from breast milk and antibodies induced by the vaccine will be transferred to children.10,12,20 However, the protective effect of exclusive breastfeeding in babies born to vaccinated mothers presented a slight increase when associated with maternal vaccination during pregnancy and should be assessed further with larger samples and at different epidemiological moments.
A possible limitation of this study was the confirmation of cases by clinical criteria. Perhaps the reason why a good effectiveness of maternal vaccination was not found in the prevention of PLI. On the other hand, if this error occurred, it is expected to be of lesser magnitude, because the clinical criterion is used by the WHO and the Brazilian MH to define cases of pertussis.1,3 Another limitation would be the losses due to the lack of information related to the vaccination situation of the pregnant women, especially in controls, which may have led to a selection bias. However, there are no indicators of greater loss of control in which pregnant women were vaccinated and that the losses of pregnant women presented different characteristics for the pregnant women included in the study.
Exclusive breastfeeding protects children under six months from PLI and can be enhanced when associated with maternal vaccination. These strategies should be encouraged because they also protect against pertussis-like illnesses.
FundingThis study was supported of the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES) - funding code 001 and with the support of the National Council for Scientific and Technological Development (CNPq) of the Universal Notice 14 -2013 Band C - code 487030702013-3 APQ
Conflicts of interestThe authors declare no conflicts of interest.
Study conducted at Universidade de Pernambuco, Pós-Graduação em Ciências da Saúde, Faculdade de Ciências Médicas, Recife, PE, Brazil.





