
This study investigated the presence of musculoskeletal symptoms in high school adolescents from public schools and its association with electronic device use.
MethodsThe sample consisted of 961 boys and girls aged 14–19 years who answered a questionnaire regarding the use of computers and electronic games, and questions about pain symptoms and physical activity. Furthermore, anthropometric assessments of all volunteers were performed. The chi-squared test and a multiple logistic regression model were used for the inferential analysis.
ResultsThe presence of musculoskeletal pain symptoms was reported by 65.1% of the adolescents, being more prevalent in the thoracolumbar spine (46.9%), followed by pain in the upper limbs, representing 20% of complaints. The mean time of use for computers and electronic games was 1.720 and 583minutes per week, respectively. The excessive use of electronic devices was demonstrated to be a risk factor for cervical and lumbar pain. Female gender was associated with the presence of pain in different body parts. Presence of a paid job was associated with cervical pain.
ConclusionA high prevalence of musculoskeletal pain in adolescents, as well as an increased amount of time using digital devices was observed. However, it was only possible to observe an association between the increased use of these devices and the presence of cervical and low back pain.
Este estudo investigou a presença de sintomas musculoesqueléticos em adolescentes estudantes do ensino médio em escolas públicas e sua associação com o uso de dispositivos eletrônicos.
MétodoA amostra foi composta por 961 meninos e meninas com idade entre 14 e 19 anos que responderam questionário sobre o uso de computadores, jogos eletrônicos e questões relacionadas a sintomas dolorosos e atividade física. Além disso, todos os voluntários foram submetidos à avaliação antropométrica. Para análise inferencial foram utilizados os testes de qui-quadrado e modelo múltiplo de regressão logística.
ResultadosA presença de sintomas de dor musculoesquelética foi reportada por 65.1% dos adolescentes, sendo mais prevalente na coluna toracolombar (46,9%), seguida por dor nos membros superiores, representando 20% das queixas. O tempo médio de uso de computador e jogos eletrônicos foi 1720 e 583 minutos por semana, respectivamente. O uso excessivo dos dispositivos eletrônicos mostrou-se como fator de risco para dor cervical e lombar. O sexo feminino apresentou associação com a presença de dor em diferentes partes do corpo. A atividade profissional esteve associada com a dor cervical.
ConclusãoObservou-se alta prevalência de dor musculoesquelética nos adolescentes e elevado tempo de uso dos dispositivos eletrônicos. Entretanto, foi possível observar somente a associação do uso excessivo desses dispositivos e a presença de dor cervical e lombar.
The use of electronic devices has, in recent years, become an important part in the lives of adolescents, who regularly use computers to carry out academic and leisure activities.1,2 Other resources used by this population include the different types of electronic games, which, just like computers, have attracted an exaggerated interest, causing children and adolescents to spend hours being entertained by such technologies, often interfering with their social relationships.3,4
The excessive use of these devices has been associated with several health problems, such as obesity, headaches, anxiety, stress, sleep disorders, musculoskeletal pain, and decreased physical activity levels.1,2,5,6
Musculoskeletal symptoms are a major cause of acute, chronic, and recurrent pain in children and adolescents, significantly affecting the psychosocial status and considered a public health problem.7–11 Their prevalence in recent studies with adolescents has ranged between 19.5% and 56%.2,8–11
Studies have shown that prolonged periods in a static position may result in spinal column pain and increase the risk of developing complaints in other body partss.12–15 A study carried out with Finnish adolescents suggested that musculoskeletal symptoms that cause moderate to severe pain are common among computer users.2
The association between computer use and the presence of musculoskeletal pain in adolescents was not demonstrated in a study conducted in Brazil in 2004.12 However, studies performed in developed countries have demonstrated an association between time of computer use and painful symptoms in the lower limbs and cervical spinal column of adolescents.13,16,17 Therefore, it can be observed that the time factor, added to the technological development and socioeconomic level of a region, may have influenced these results.
Considering the recent technological and economic growth observed in Brazil and that concomitant to this fact, there has been an increase in access to these technologies, it is believed that today's adolescents are more exposed to these resources. Additionally, in 2012, the State Secretariat of Education (Secretaria Estadual de Educação – SEE) of Pernambuco, using a strategy considered to be innovative, distributed laptops to all high school students, thereby increasing access to this type of technology. The aim of this study was to determine the prevalence of musculoskeletal pain in adolescents and its association with the use of electronic devices.
MethodsThis was an epidemiological, correlational, and cross-sectional study, which was approved by the Research Ethics Committee of the Universidade de Pernambuco under protocol No. CAAE 13598313.5.0000.5207.
The study population consisted of adolescents aged 14–19, enrolled in public high schools in the city of Recife, state of Pernambuco, Brazil. According to data provided by the SEE, in 2012 an estimated 55,058 adolescents were enrolled in 108 public high schools. The following criteria were used to quantify sample size: estimated population of 55,058 students; 95% confidence interval; sampling error of five percentage points; estimated prevalence of 50%; sample loss of 20% and a two-fold design effect.
The sample selection procedure followed a sequence of steps aiming to obtain a representative sample regarding the distribution of students according to geographic region and school size. Initially, the number of schools that had high school classes was observed. Then, taking into account the geographical and organizational distribution, schools were divided into each of the Regional Education Offices. Finally, schools were divided into three categories: small (up to 200 students), medium-sized (201–499 students), and large (500 or more students).18,19
In the second stage, the cluster sampling was performed in two steps, considering the school and the class as sampling units. In the first step, school proportionality was considered by size; in the second step, the proportionality of classes was considered.19 Therefore, the authors found a minimum number of 23 schools and 96 classes, which represent 20% of public schools in Recife and a total of 954 adolescents.
Inclusion criteria included attending one of the selected schools and age between 14 and 19 years. Exclusion criteria comprised the inadequate completion of the questionnaire or refusal to undergo anthropometric measurements. Pregnant women and students who had musculoskeletal pain or injuries due to infectious, genetic, or traumatic disorders were excluded from the study.
Data were collected through a constructed and adapted questionnaire aimed to assess sociodemographic variables (age, gender, school year, presence of a paid job, and family income), data on the use of computer and video games (age of onset of use, weekly frequency, and time of use), presence of musculoskeletal pain (location and use of pain medications), and physical activity level.
A self-administered questionnaire was used to evaluate the use of electronic devices and painful symptoms, which included aspects of the musculoskeletal system painful symptoms, body diagram for symptom location, and questions related to the use of computer and video games. This tool has excellent interday reliability (Kappa>0.72).11,12
To evaluate the pain symptoms, the adolescents were asked to indicate in the body chart the regions where they had experienced pain in the last six months. As for the pain symptoms, the adolescents answered the questions related to the use of electronic devices, always considering the six months prior to the day of data collection. Time periods greater than 4h/day for the use of all electronic equipment, 3h/day for computers, and 1h/day for video games were considered excessive. These cutoff points were determined by the median value found in the assessed sample.
The level of physical activity was assessed based on the answers to the International Physical Activity Questionnaire (IPAQ) – Short Form,20 and volunteers were classified as active or insufficiently active. The anthropometric data were recorded using a G-THEC portable electronic scale with 150kg capacity (Camry Electronic, USA) and a WCS portable stadiometer (Cardiomed Comércio de Equipamentos Médicos LTDA, Brazil). These data were used to calculate body mass index (BMI) and to perform overweight and obesity classification.21
Data analysis was performed using SPSS software (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0; USA). Bivariate logistic regression models were constructed to test the isolated association between the dependent variable and each independent variable, as well as to analyze the variables in the model, to explore the possible confounding factors and identify the need for statistical adjustment of analysis. Multiple logistic regression was used through the estimate of odds ratio and 95% confidence intervals (95% CI) to express the degree of association between the independent variables and the presence of pain.
For the final multiple model, the selected variables were those whose p-value was <0.20. In all tests, a p-value <0.05 was considered statistically significant. Considering the sampling design used in the study (cluster sampling in two stages), it was decided to perform inferential statistics using the “complex sampling mode” of SPSS to apply the correction of estimates for the design effect.
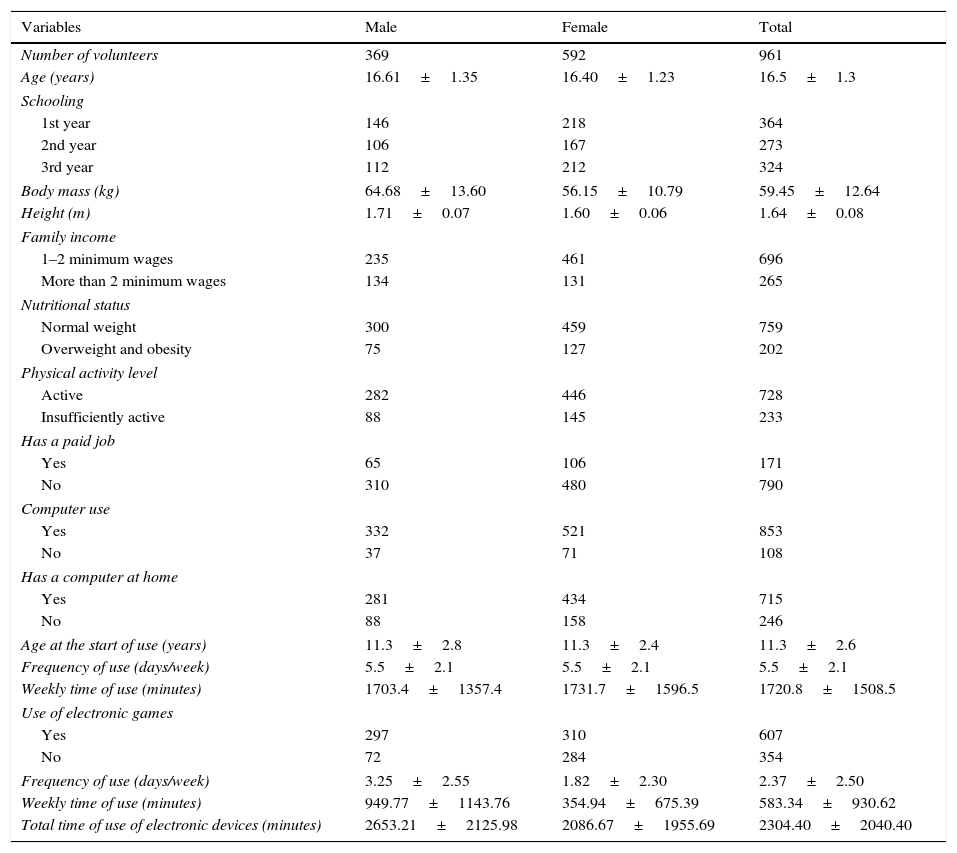
ResultsIn total, 1020 adolescents were included in the study. However, 59 individuals were excluded due to errors when completing the questionnaire. The final sample consisted of 961 adolescents. The sociodemographic and anthropometric characteristics, nutritional status, physical activity level, presence of a paid job, and data related to the use of electronic devices are described in Table 1.
Sociodemographic, anthropometric characteristics, nutritional status, physical activity level, and occupation of adolescents from public schools in Recife, stratified by gender.
| Variables | Male | Female | Total |
|---|---|---|---|
| Number of volunteers | 369 | 592 | 961 |
| Age (years) | 16.61±1.35 | 16.40±1.23 | 16.5±1.3 |
| Schooling | |||
| 1st year | 146 | 218 | 364 |
| 2nd year | 106 | 167 | 273 |
| 3rd year | 112 | 212 | 324 |
| Body mass (kg) | 64.68±13.60 | 56.15±10.79 | 59.45±12.64 |
| Height (m) | 1.71±0.07 | 1.60±0.06 | 1.64±0.08 |
| Family income | |||
| 1–2 minimum wages | 235 | 461 | 696 |
| More than 2 minimum wages | 134 | 131 | 265 |
| Nutritional status | |||
| Normal weight | 300 | 459 | 759 |
| Overweight and obesity | 75 | 127 | 202 |
| Physical activity level | |||
| Active | 282 | 446 | 728 |
| Insufficiently active | 88 | 145 | 233 |
| Has a paid job | |||
| Yes | 65 | 106 | 171 |
| No | 310 | 480 | 790 |
| Computer use | |||
| Yes | 332 | 521 | 853 |
| No | 37 | 71 | 108 |
| Has a computer at home | |||
| Yes | 281 | 434 | 715 |
| No | 88 | 158 | 246 |
| Age at the start of use (years) | 11.3±2.8 | 11.3±2.4 | 11.3±2.6 |
| Frequency of use (days/week) | 5.5±2.1 | 5.5±2.1 | 5.5±2.1 |
| Weekly time of use (minutes) | 1703.4±1357.4 | 1731.7±1596.5 | 1720.8±1508.5 |
| Use of electronic games | |||
| Yes | 297 | 310 | 607 |
| No | 72 | 284 | 354 |
| Frequency of use (days/week) | 3.25±2.55 | 1.82±2.30 | 2.37±2.50 |
| Weekly time of use (minutes) | 949.77±1143.76 | 354.94±675.39 | 583.34±930.62 |
| Total time of use of electronic devices (minutes) | 2653.21±2125.98 | 2086.67±1955.69 | 2304.40±2040.40 |
Dichotomous categorical variables are shown as absolute frequency values.
Continuous variables are shown as mean and standard deviation.
The presence of pain symptoms was reported by 626 (65.1%) adolescents. The anatomical region with the highest prevalence of pain complaints was the thoracolumbar spine (n=451; 46.9% [95% CI: 43.7–50.1%]), followed by the upper limbs (n=192; 20% [95% CI: 17.5–22.7%]), cervical spine (n=178; 18.5% [95% CI: 16.1–21.1%]), and scapular region (n=152; 15.8% [95% CI: 13.5–18.3%]).
It was observed that 199 adolescents (31.8% [95% CI: 28.2–35.6%]) reported that using the computer was the triggering factor for at least one symptom. Other factors cited as triggers were physical exercise in 128 (20.5% [95% CI: 17.6–23.8%]) and the use of electronic games in 18 adolescents (2.9% [95% CI: 1.7–4.5%]).
Another assessed aspect was the influence of pain symptoms when performing activities of daily living, with the adolescents reporting that at least one of the pain symptoms interfered with or hindered the accomplishment of study tasks (143; 22.8% [95% CI: 19.7–26.3%]), sleeping (115; 18.4% [95% CI: 15.4%–21.6%]), and playing sports (110; 17.6% [95% CI: 14.7–20.8%]). Additionally, 186 (29.7% [95% CI: 26.2–33.5%]) adolescents said that the presence of pain made them more nervous. Finally, 201 (32.1% [95% CI: 28.5–35.9%]) adolescents reported that they made sporadic use of analgesics, while another 70 (11.1% [95% CI: 8.8–13.9%]) reported that they frequently used these drugs.
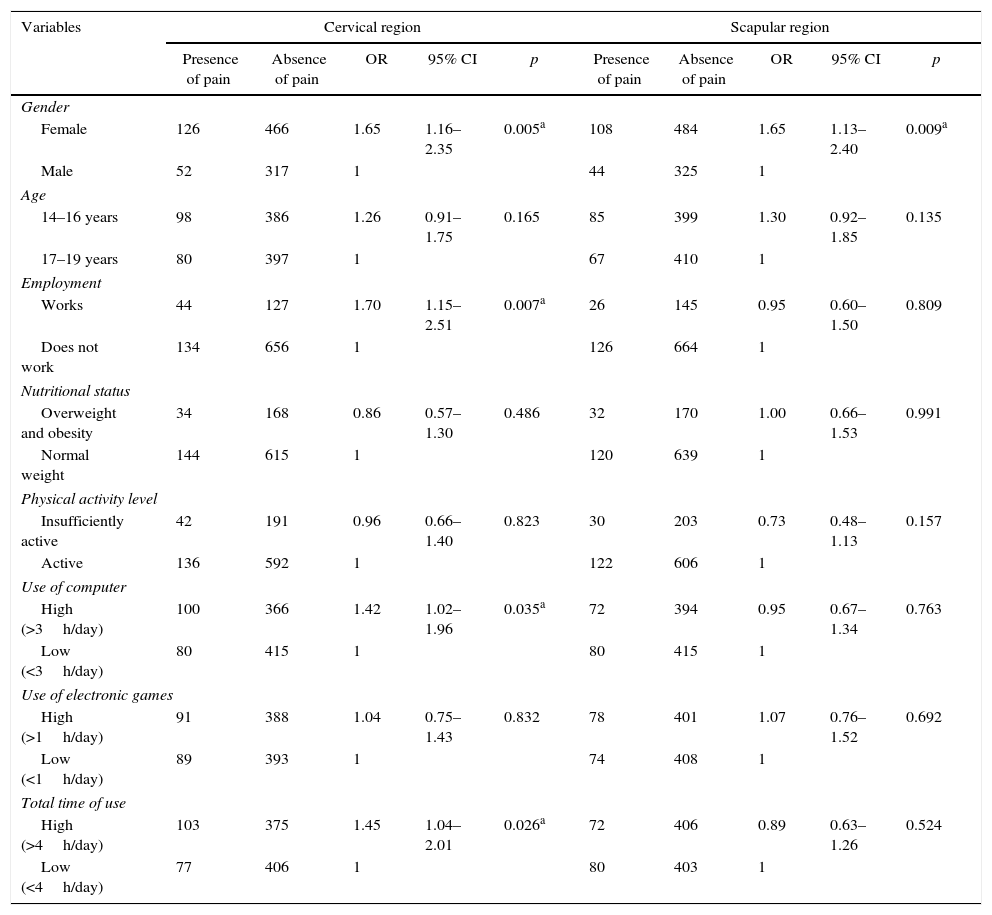
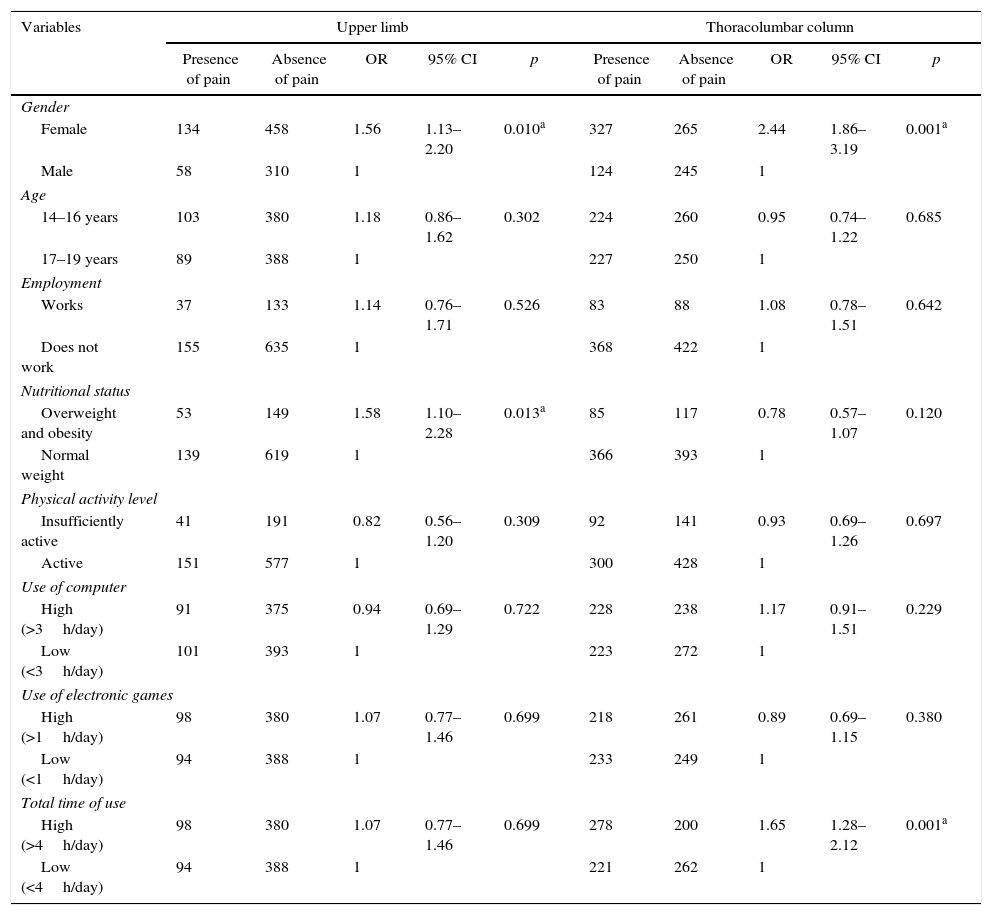
The results of the bivariate regression analysis showed that female gender was associated with musculoskeletal pain in all assessed anatomical regions. An association was observed between the presence of cervical pain and having a paid job as well as high amount of time using electronic devices (Table 2). High amount of time using electronic devices was associated with pain symptoms in the thoracolumbar region and excess weight was associated with pain symptoms in the upper limbs (Table 3).
Sociodemographic variables, physical activity level, nutritional status, and use of electronic devices and their association with complaints of pain in the cervical and scapular regions.
| Variables | Cervical region | Scapular region | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Presence of pain | Absence of pain | OR | 95% CI | p | Presence of pain | Absence of pain | OR | 95% CI | p | |
| Gender | ||||||||||
| Female | 126 | 466 | 1.65 | 1.16–2.35 | 0.005a | 108 | 484 | 1.65 | 1.13–2.40 | 0.009a |
| Male | 52 | 317 | 1 | 44 | 325 | 1 | ||||
| Age | ||||||||||
| 14–16 years | 98 | 386 | 1.26 | 0.91–1.75 | 0.165 | 85 | 399 | 1.30 | 0.92–1.85 | 0.135 |
| 17–19 years | 80 | 397 | 1 | 67 | 410 | 1 | ||||
| Employment | ||||||||||
| Works | 44 | 127 | 1.70 | 1.15–2.51 | 0.007a | 26 | 145 | 0.95 | 0.60–1.50 | 0.809 |
| Does not work | 134 | 656 | 1 | 126 | 664 | 1 | ||||
| Nutritional status | ||||||||||
| Overweight and obesity | 34 | 168 | 0.86 | 0.57–1.30 | 0.486 | 32 | 170 | 1.00 | 0.66–1.53 | 0.991 |
| Normal weight | 144 | 615 | 1 | 120 | 639 | 1 | ||||
| Physical activity level | ||||||||||
| Insufficiently active | 42 | 191 | 0.96 | 0.66–1.40 | 0.823 | 30 | 203 | 0.73 | 0.48–1.13 | 0.157 |
| Active | 136 | 592 | 1 | 122 | 606 | 1 | ||||
| Use of computer | ||||||||||
| High (>3h/day) | 100 | 366 | 1.42 | 1.02–1.96 | 0.035a | 72 | 394 | 0.95 | 0.67–1.34 | 0.763 |
| Low (<3h/day) | 80 | 415 | 1 | 80 | 415 | 1 | ||||
| Use of electronic games | ||||||||||
| High (>1h/day) | 91 | 388 | 1.04 | 0.75–1.43 | 0.832 | 78 | 401 | 1.07 | 0.76–1.52 | 0.692 |
| Low (<1h/day) | 89 | 393 | 1 | 74 | 408 | 1 | ||||
| Total time of use | ||||||||||
| High (>4h/day) | 103 | 375 | 1.45 | 1.04–2.01 | 0.026a | 72 | 406 | 0.89 | 0.63–1.26 | 0.524 |
| Low (<4h/day) | 77 | 406 | 1 | 80 | 403 | 1 | ||||
OR, odds ratio; 95% CI, 95% confidence interval.
Sociodemographic variables, level of physical activity, nutritional status, and use of electronic devices and their association with complaints of pain in the thoracolumbar region and upper limbs.
| Variables | Upper limb | Thoracolumbar column | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Presence of pain | Absence of pain | OR | 95% CI | p | Presence of pain | Absence of pain | OR | 95% CI | p | |
| Gender | ||||||||||
| Female | 134 | 458 | 1.56 | 1.13–2.20 | 0.010a | 327 | 265 | 2.44 | 1.86–3.19 | 0.001a |
| Male | 58 | 310 | 1 | 124 | 245 | 1 | ||||
| Age | ||||||||||
| 14–16 years | 103 | 380 | 1.18 | 0.86–1.62 | 0.302 | 224 | 260 | 0.95 | 0.74–1.22 | 0.685 |
| 17–19 years | 89 | 388 | 1 | 227 | 250 | 1 | ||||
| Employment | ||||||||||
| Works | 37 | 133 | 1.14 | 0.76–1.71 | 0.526 | 83 | 88 | 1.08 | 0.78–1.51 | 0.642 |
| Does not work | 155 | 635 | 1 | 368 | 422 | 1 | ||||
| Nutritional status | ||||||||||
| Overweight and obesity | 53 | 149 | 1.58 | 1.10–2.28 | 0.013a | 85 | 117 | 0.78 | 0.57–1.07 | 0.120 |
| Normal weight | 139 | 619 | 1 | 366 | 393 | 1 | ||||
| Physical activity level | ||||||||||
| Insufficiently active | 41 | 191 | 0.82 | 0.56–1.20 | 0.309 | 92 | 141 | 0.93 | 0.69–1.26 | 0.697 |
| Active | 151 | 577 | 1 | 300 | 428 | 1 | ||||
| Use of computer | ||||||||||
| High (>3h/day) | 91 | 375 | 0.94 | 0.69–1.29 | 0.722 | 228 | 238 | 1.17 | 0.91–1.51 | 0.229 |
| Low (<3h/day) | 101 | 393 | 1 | 223 | 272 | 1 | ||||
| Use of electronic games | ||||||||||
| High (>1h/day) | 98 | 380 | 1.07 | 0.77–1.46 | 0.699 | 218 | 261 | 0.89 | 0.69–1.15 | 0.380 |
| Low (<1h/day) | 94 | 388 | 1 | 233 | 249 | 1 | ||||
| Total time of use | ||||||||||
| High (>4h/day) | 98 | 380 | 1.07 | 0.77–1.46 | 0.699 | 278 | 200 | 1.65 | 1.28–2.12 | 0.001a |
| Low (<4h/day) | 94 | 388 | 1 | 221 | 262 | 1 | ||||
OR, odds ratio; 95% CI, 95% confidence interval.
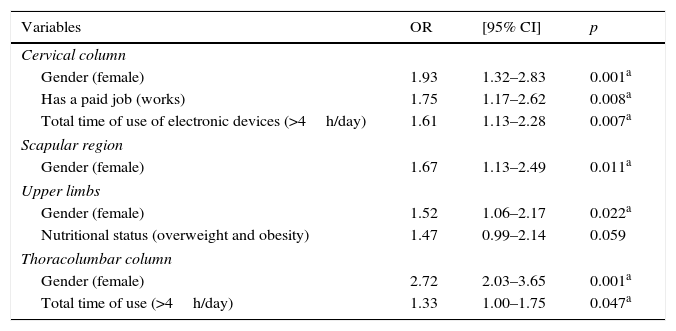
The multivariate model results for the pain symptoms in the four assessed areas are shown in Table 4. The variable gender remained associated in the final model of the four assessed areas. The total time of electronic device use remained associated with pain in the cervical and thoracolumbar regions. Presence of a paid job remained associated with the presence of pain in the cervical region and the nutritional status remained in the final model of upper limb pain, although without a significant association.
Multiple association model of musculoskeletal pain in high school adolescents.
| Variables | OR | [95% CI] | p |
|---|---|---|---|
| Cervical column | |||
| Gender (female) | 1.93 | 1.32–2.83 | 0.001a |
| Has a paid job (works) | 1.75 | 1.17–2.62 | 0.008a |
| Total time of use of electronic devices (>4h/day) | 1.61 | 1.13–2.28 | 0.007a |
| Scapular region | |||
| Gender (female) | 1.67 | 1.13–2.49 | 0.011a |
| Upper limbs | |||
| Gender (female) | 1.52 | 1.06–2.17 | 0.022a |
| Nutritional status (overweight and obesity) | 1.47 | 0.99–2.14 | 0.059 |
| Thoracolumbar column | |||
| Gender (female) | 2.72 | 2.03–3.65 | 0.001a |
| Total time of use (>4h/day) | 1.33 | 1.00–1.75 | 0.047a |
OR, odds ratio; 95% CI, 95% confidence interval.
A high prevalence of musculoskeletal pain was observed among the adolescents, higher than that shown in previous studies in Brazil11,12 and in other countries.2,22 This evidence alone reinforces the importance of such investigation of factors associated with this problem and thus, it becomes essential to provide health assessment and comprehensive health care.
As for symptom location, the region with the highest prevalence of pain complaints was the thoracolumbar spine (46.9%). Recent studies with Brazilian23 and Chinese students8 showed a prevalence rate close to 32% for low back pain. Although these findings were lower, they still seem to corroborate the present results, as this study also included symptoms related to the thoracic spine, which may explain this difference. The second most prevalent pain was in the upper limbs, followed by the cervical spine. These findings corroborate previous studies,2,3 which reported prevalence of pain in the cervical and shoulder regions in approximately 21–22% of adolescents.
Regarding the use of electronic devices, several studies have shown increased computer use, as demonstrated in this study, with prevalence ranging between 74% and 99% of adolescents.1,11,14 This result may be associated with the implemented government program, which distributed the equipment to all high school students and contributed to increasing access to this technology, which was previously only associated with families of higher socioeconomic level.4,5,24 According to previous studies, the total weekly time spent by adolescents using computers ranged from 80 to 840min.2,4,5,24–27 Nonetheless, the present study showed time spent at the computer close to 1720minutes per week, raising questions about that time, as several studies have emphasized the association of several health complaints with excessive use of such devices.2,28
Regarding the use of electronic games, Milde-Busch et al.1 reported a low frequency (27%) among adolescents, which differs from the results of this study. This higher frequency is probably due to the fact that electronic games have become increasingly popular, representing one of the most important leisure activities for adolescents, regardless of age and socioeconomic strata.25,26 This finding is reinforced by the data found in relation to the weekly time of use, which averaged close to 583min, higher than the 390min described in previous studies.4,5,12
Regarding the analysis of factors associated with pain complaints, it was observed that the female gender, total time of electronic device use, nutritional status, and presence of a paid job remained in the final statistical models.
Female gender was associated with pain complaints in all anatomical regions and was considered a risk factor. The presence of pain complaints in different body regions by the adolescents was also demonstrated in a study carried out in Finland, in which girls reported pain in all anatomical sites and, consequently, more disruption to daily life.2
The gender question can be explained by the fact that women complain more than men, often reporting more relevant health information due to social and educational issues, as well as the presence of hormonal changes during puberty.9 These findings have been demonstrated by other studies in the literature.16,23 Costigan et al.29 reported that girls show lower levels of physical activity and increased time spent in sedentary behaviors associated with hormonal variations, which negatively contribute to several health indicators, including musculoskeletal pain.
Another sociodemographic factor associated with pain symptoms, specifically cervical pain, was presence of a paid job. Although studies conducted with adolescents about pain symptoms have similar characteristics to those of the present study, regarding the assessment of schoolchildren2,14,22,23 and the prevalence of adolescent females,2,16 many of these studies2,22,23 disregarded data related to having a paid job and employment. Zapata et al.12 reported that less than 1% of the assessed adolescents had a job.
In the present study, approximately 18% of the adolescents reported having a job, differing from the results found in the literature.13 This finding can be explained by differences in socioeconomic status of the assessed samples, as previous studies2,12,14,22,23 reported assessing middle-class adolescents or students from private schools, whereas in this study the majority of assessed students had low family income. Possibly due to this situation, this sample had to work to help with family expenses, which can contribute to greater physical and mental stress.
The use of electronic devices was only associated with pain complaints in the spinal column. In this respect, it was observed that the isolated use of computers or electronic games showed no association with pain complaints; however, when assessing the combined use of these devices, it became clear that the elevated total time of use is characterized as a risk factor for the presence of cervical and thoracolumbar pain.
Corroborating these results, Hakala et al.2 also found that computer use is associated with cervical pain; however, with a mean time of use of 2h daily. Another study showed that the longer the time of screen exposure, the greater the chances of developing spinal column pain.22 Zapata et al.12 found no association between pain and the use of electronic games and computers, differing from the results found in this study. This difference is possibly due to the characteristics related to the time of the study, given that the access and screen time reported by Zapata et al.,12 ten years ago, was lower than that found in the present study and in others.2,22
In addition to the presence of pain and its location, the assessment of its intensity is also recommended. However, the study by Hakala et al.2 is the only one that assessed the association between computer use and the location and intensity of pain symptoms in the spinal column of adolescents. Although the authors reported that excessive use of these devices is related to moderate and severe intensity, they point out that these data should be analyzed with caution, considering that the study cross-sectional design does not allow for inference of causality, as well as the fact that a self-report evaluation may show recall bias. The authors also showed that the subjective nature of pain assessment can generate incorrect information and/or overestimation of the responses. Corroborating this information, Rothaug et al.30 described that pain assessment with binary responses is a more practical method for pain assessment when compared to the use of numerical scales, with the binary method being preferred by most patients.
Considering this information, it was decided not to use pain intensity assessment in this study, as all these possible limitations, in addition to the six-month recall, could generate a significant bias, thus affecting the results. The authors considered the possibility that, in six months, the adolescents could have had more than one episode of pain, and these episodes could have had variations in their duration; therefore, the report of pain intensity would be complex, subjective, and subject to considerable variation.
Although no association was verified between the use of electronic devices and other pain complaints, it was observed that 31.8% of the adolescents reported that using a computer was a triggering factor of at least one symptom. Another important aspect refers to the report that the presence of pain symptoms interfered with many daily activities, such as performing tasks, sleep, and practicing sports, as well as being responsible for self-medication in a significant number of subjects, which can cause health problems or even mask symptoms of more important diseases.
This study has some sample-related limitations, as these were public school students and, therefore its generalization to other populations is not possible. The data were obtained from students’ self-reports and, thus, recall bias may be possible; it is important to exercise caution when interpreting these data. However, these results are relevant, as they suggest that technological development, which society is facing, can have significant effects, requiring constant monitoring of health indicators and associated factors.
Finally, the results showed a high prevalence of musculoskeletal pain and the high amount of time spent using electronic devices. However, the increased use of these devices only showed an association with pain in the cervical and thoracolumbar regions.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silva GR, Pitangui AC, Xavier MK, Correia-Júnior MA, Araújo RC. Prevalence of musculoskeletal pain in adolescents and association with computer and videogame use. J Pediatr (Rio J). 2016;92:188–96.





