
The main purpose of the current study was to perform the cross cultural adaptation and validation of the Activities Scale for Kids (ASK) both in its capability and performance versions to the European Portuguese language so it can be used in Portugal by healthcare professionals in children from 5 to 15 years of age with functional disabilities related to specific health conditions.
MethodsThe cross-cultural adaptation of ASK followed the classic sequential methodology for linguistic equivalence. To test its validity, internal consistency, and reproducibility, the Portuguese version of ASK was administered together with the KINDL Questionnaire (KINDL) to 88 children (10±3 years of age) with functional limitations. The test–retest study was conducted two weeks apart.
ResultsAfter obtaining the semantic and content validity, the Portuguese version of ASK demonstrated good levels of reproducibility (performance: intraclass correlation coefficient [ICC]=0.99; capability: ICC=0.98) and internal consistency (performance: α=0.98; capability: α=0.97). The correlations between ASK and KINDL were positive and moderate.
ConclusionsThe Portuguese version of ASK showed acceptable levels of validity, internal consistency, and reproducibility; the authors recommend its use in clinical settings.
O principal objetivo deste estudo foi realizar a adaptação transcultural para o português europeu e a validação das versões de capacidade e desempenho da Escala de Atividades para Crianças (Activity Scale for Kids (ASK)), de forma que possa ser utilizada em Portugal por profissionais da saúde com crianças de 5 a 15 anos de idade com deficiências funcionais relacionadas a doenças específicas.
MétodosA adaptação transcultural da ASK seguiu a metodologia sequencial clássica para obter equivalência linguística. Para testar sua validade, coerência interna e reprodutibilidade, a versão em português da ASK foi administrada juntamente com o Questionário KINDL (KINDL) em 88 crianças (10±3 anos de idade) com limitações funcionais. O estudo de teste-reteste foi realizado com um intervalo de duas semanas.
ResultadosApós obter a validade semântica e de conteúdo, a versão em português da ASK demonstrou bons níveis de reprodutibilidade (desempenho: coeficiente de correlação intraclasse (CCI)=0,99; capacidade: CCI=0,98) e coerência interna (desempenho: α=0,98; capacidade: α=0,97). As correlações entre a ASK e o KINDL foram positivas e moderadas.
ConclusõesA versão em português da ASK apresentou níveis aceitáveis de validade, coerência interna e reprodutibilidade, e recomendamos seu uso em ambientes clínicos.
The World Health Organization estimated that 15% of the world population lives with disabilities.1 Therefore, measuring disability is essential for developing programs and policies to promote the integration and participation of these individuals.1 Similarly, to assess the effectiveness of healthcare interventions, it is necessary to quantify the impact of functional limitations on activity and participation of the individuals.2
Despite the efforts and the published studies, no measurement instrument covered all components of functionality.3,4 Recently, several outcome measures have been developed specifically for children with disabilities5; however, few are adapted for the Portuguese culture.
The Activity Scale for Kids (ASK) is a specific measure for the pediatric population, intended to assess the degree of disability in children aged 5–15 years with functional limitations, within a wide range of health conditions. Moreover, this measure has been shown to have good psychometric properties and significant clinical utility.2,5 Its clinical utility is important, being a valid measure with correlation values between 0.82 (ASK–Performance [ASKp]) and 0.85 (ASK–Capability [ASKc]) with the Childhood Health Assessment Questionnaire – CHAQ. It presents good reproducibility values at 2 weeks (ICC=0.97 for ASKp and ICC=0.98 for ASKc) and a Cronbach alpha value of 0.99. It was also shown to be able to discriminate among different levels of disability.6 It has been widely referenced in the literature.7–19
One of the few child outcome measures adapted for the Portuguese culture is the KINDL questionnaire. It is a generic instrument conceived to measure quality of life of sick or healthy children and adolescents, from 4 to 17 years of age. It is available to be used in three age groups (4–6, 7–13, and 14–17) and has five versions, depending on the age of the respondent and the information source (children or parents version).20
The Portuguese version of KINDL was shown to be semantically equivalent to the original measure; it offers good levels of reliability and acceptable levels of validity.20
The main objective of this study was to culturally adapt the ASKc and ASKp modules to European Portuguese and to evaluate their validity and reliability.
MethodsThe present study proceeded in two phasesThe first phase followed the sequential approach, commonly used in these type of studies to obtain a linguistically equivalent version.9,21,22 It includes the authorization given by the author of the original instrument2 and its adaptation for European Portuguese language and culture.
A formal permission for the cross-cultural adaptation to Portuguese was obtained from Nancy Young, the developer of ASK. This process was performed according to the stages guideline used in self-report measures.6
- •
Forward translation. The original version of ASK was translated into Portuguese by two independent Portuguese translators fluent in English.
- •
Consensus version. A panel composed by three experts from the Center for Health Studies and Research of the University of Coimbra developed a consensus version from both translations (first preliminary version). This synthesis process was documented in a written report.
- •
Back-translation. A translator, native in English and fluent in Portuguese, translated the consensus version back into English. This back-translation and all previous translations of ASK were taken into consideration to reach a consensus, obtaining the second preliminary version. This process was documented in a written report.
- •
Content validity. An expert review committee, composed by two pediatric physical therapists and a physician specialized in pediatric physical medicine and rehabilitation, reached a consensus on the translation of ASK. This expert committee meeting resulted in a pre-final version. The final stage of the cross-cultural adaptation of ASK was to cognitively pre-test the questionnaire. Children and parents were interviewed to assess whether the items were understandable. To obtain a general representation of the population, the initial panel was composed by 15 children with different characteristics and a parents’ panel composed by four parents of children less than 10 years old; two of these children were healthy. After filling the questionnaire, each participant was asked to point out any difficulties in understanding or ambiguities in the translation.
This stage completed the creation of the Portuguese version of both ASKp and ASKc.
The second phase examined the validity and reliability tests of the Portuguese version. Specifically, the authors assessed construct validity, internal consistency, and reproducibility.
ParticipantsA convenience sample collected at 11 healthcare institutions (hospitals and patient associations) was used, including 88 children aged between 5 and 15 years with various types of functional disorders (neuromuscular, orthopedic/traumatology and/or rheumatology, cardio-respiratory, or others). Children with cognitive deficits and children with sensorial changes that would prevent them from answering or understanding the measure were excluded from the analysis.2
The healthcare institutions obtained approval from their respective institutional review boards, and consent was obtained from the different participants. Before each face-to-face interview there was a explanation of the study, including its goals, confidentiality and participation conditions.
Data collectionThe protocols were mailed to the institutions that had agreed to participate, along with pre-stamped envelopes for the answers. One physiotherapist of each institution was responsible for selecting the sample elements and for administering the protocols during the defined periods.
Children up to 10 years responded to the questionnaire in the presence of adults (physical therapist, parents, or caregivers); nonetheless, the answer always came from the child. Children older than 10 years read and responded by themselves, except in the case of those who had visual or motor disabilities that would prevent them from responding.
The data collection protocol contained both ASK modules, the Portuguese version of KINDL, and a form to collect some questions of patient characteristics, including two clinical questions (regarding mobility needs and health conditions). The ASK was applied twice to the same participants with an interval of one to two weeks, to assess reproducibility.
InstrumentsThe Portuguese versions of both ASK and KINDL were administered.
The ASK is a specific pediatric measure composed of two modules: ASKc, which reflects what the child is able to do in his/her daily environment, and ASKp, which reflects what the child actually does on his/her daily environment.
Both modules are organized in seven domains (personal care, dressing, other skills, locomotion, play, standing skills, and transfers) containing 30 items each, identical but with different answer options.5 This instrument is self-administered for children aged 10 years or older. Children under 10 years of age have to be helped by their caregivers, but the answers have to be exclusively given by the children. The ASK cannot be applied on children that are unable to understand what is being asked.
In both modules, the summary scores were calculated by the mean of the answers (0–4 points), and the result was reported as a percentage score (range 0–100), where 100% indicates full physical function.6
The KINDL measures six dimensions of quality of life (physical and emotional well-being, self-esteem, family, friends, and school). Regarding the age group, three versions of the questionnaire were used: Kiddy, for children aged 4–6 years (interview); Kid, for children aged 7–13; and Kiddo, for teenagers (14–17).20
Individual dimension scores can be calculated by adding the responses given to the questions transformed to a positive scale of 0–100, according to the KINDL manual.23 The total score can be obtained by the sum of the dimension scores, where higher values indicated better quality of life. Reverse scoring was applied to some items, so that higher item scores represent better quality of life.20
Statistical analysisThe characteristics of study participants were summarized using descriptive statistics of central tendency, dispersion, frequencies, and percentages, according to the type of variables.
The construct validity was assessed analyzing Pearson's correlation coefficients (r) obtained between the dimensions of KINDL and ASK. The interpretation of the correlation values was performed based on Cohen's criteria: very low correlation (≤0.19); low (between 0.20 and 0.39); moderate (between 0.40 and 0.69); high (between 0.70 and 0.89), and very high (for values ≥0.90).24 Student's t-test was also used to compare the means of ASK dimensions between groups formed by the two clinical questions.
It was hypothesized that the best scores on quality of life would correspond to a better physical function. Similarly, individuals with neuromuscular conditions and/or needing support to move should have worse ASK scores.
To calculate the reproducibility we used the intraclass correlation coefficient (ICC) for agreement, formula 2.1. Values higher than or equal to 0.70 were considered acceptable.25 The internal consistency of ASK was tested using Cronbach's alpha. Values higher than or equal to 0.70 were considered acceptable.25
For the statistical analysis, SPSS version 18.0 for Windows was used (Inc. Released 2009. PASW Statistics for Windows, version 18.0, IL, USA). p-Values lower than 0.05 were considered statistically significant.
ResultsCross-cultural adaptationASK was successfully cross-culturally adapted into European Portuguese. The children panel was composed of 15 children (eight females), and nine of whom had unilateral or bilateral spastic cerebral palsy. The ASK was completed by the children in 34±9min. However, during this process some minor difficulties were observed regarding the meaning of the terms “blouse,” “shirt,” and “brace”. In these cases, multiple synonyms were used, to include all options, for both Portuguese versions of ASK. The item 29 of ASKc created some disagreement in the translation process concerning the sentence structure. As the recommendations of the translators were not fully accepted, it was decided to combine the proposals into a new solution, more simple and clear. Finally, all the members of the expert committee agreed with the pre-final version.
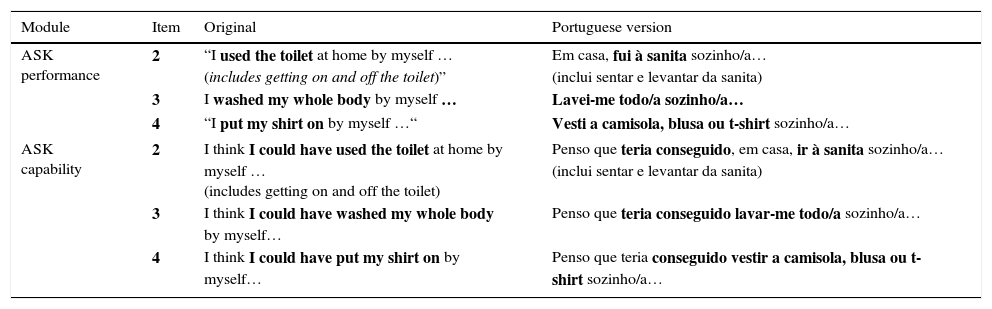
No changes resulted from either the expert committee, children panel, or parents panel (Table 1). The length of the protocol might have been, in some cases, considered inconvenient, but it was generally considered easy to understand and respond.
Example of a sub-sample of the original ASK and adapted ASK items.
| Module | Item | Original | Portuguese version |
|---|---|---|---|
| ASK performance | 2 | “I used the toilet at home by myself … (includes getting on and off the toilet)” | Em casa, fui à sanita sozinho/a… (inclui sentar e levantar da sanita) |
| 3 | I washed my whole body by myself … | Lavei-me todo/a sozinho/a… | |
| 4 | “I put my shirt on by myself …“ | Vesti a camisola, blusa ou t-shirt sozinho/a… | |
| ASK capability | 2 | I think I could have used the toilet at home by myself … (includes getting on and off the toilet) | Penso que teria conseguido, em casa, ir à sanita sozinho/a… (inclui sentar e levantar da sanita) |
| 3 | I think I could have washed my whole body by myself… | Penso que teria conseguido lavar-me todo/a sozinho/a… | |
| 4 | I think I could have put my shirt on by myself… | Penso que teria conseguido vestir a camisola, blusa ou t-shirt sozinho/a… | |
ASK, Activities Scale for Kids.
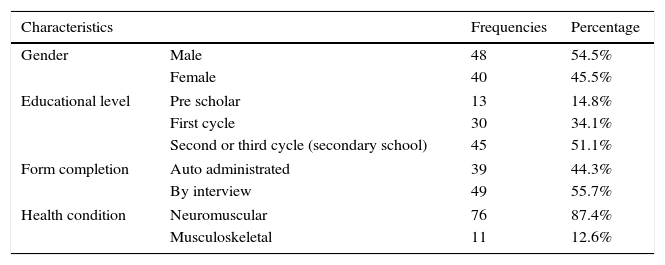
For the validity study, a sample of 88 children aged 10.2±3.2 years was used. Table 2 presents the main characteristics of the sample.
Sample validation study (n=88).
| Characteristics | Frequencies | Percentage | |
|---|---|---|---|
| Gender | Male | 48 | 54.5% |
| Female | 40 | 45.5% | |
| Educational level | Pre scholar | 13 | 14.8% |
| First cycle | 30 | 34.1% | |
| Second or third cycle (secondary school) | 45 | 51.1% | |
| Form completion | Auto administrated | 39 | 44.3% |
| By interview | 49 | 55.7% | |
| Health condition | Neuromuscular | 76 | 87.4% |
| Musculoskeletal | 11 | 12.6% | |
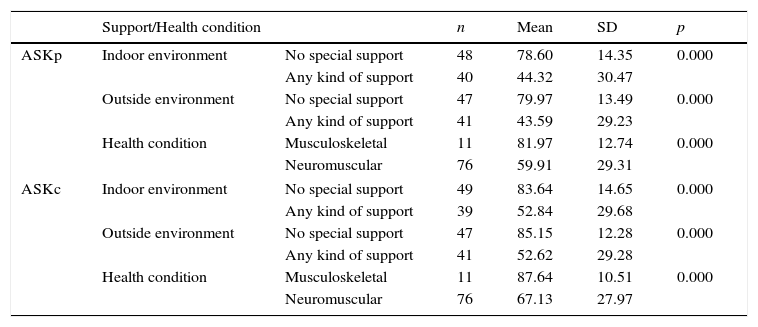
To address construct validity, the ASK scores were compared with two clinical outcomes: need for mobility support and health conditions, as well as the correlations between ASK and KINDL different dimensions.
The study of the relationship between ASK responses and the need for support (Table 3) showed that individuals with higher ASK scores (ASKp and ASKc) were less likely to require any type of support to move.
ASK vs need of support and health condition (n=88).
| Support/Health condition | n | Mean | SD | p | ||
|---|---|---|---|---|---|---|
| ASKp | Indoor environment | No special support | 48 | 78.60 | 14.35 | 0.000 |
| Any kind of support | 40 | 44.32 | 30.47 | |||
| Outside environment | No special support | 47 | 79.97 | 13.49 | 0.000 | |
| Any kind of support | 41 | 43.59 | 29.23 | |||
| Health condition | Musculoskeletal | 11 | 81.97 | 12.74 | 0.000 | |
| Neuromuscular | 76 | 59.91 | 29.31 | |||
| ASKc | Indoor environment | No special support | 49 | 83.64 | 14.65 | 0.000 |
| Any kind of support | 39 | 52.84 | 29.68 | |||
| Outside environment | No special support | 47 | 85.15 | 12.28 | 0.000 | |
| Any kind of support | 41 | 52.62 | 29.28 | |||
| Health condition | Musculoskeletal | 11 | 87.64 | 10.51 | 0.000 | |
| Neuromuscular | 76 | 67.13 | 27.97 | |||
ASK, Activities Scale for Kids.
Table 3 also presents the relationship between ASK scores and individuals’ health condition. It was evident that those who had higher ASK scores were also more likely to have musculoskeletal disorders.
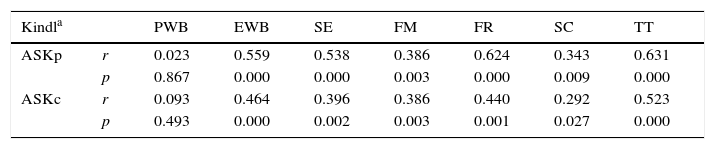
When confronting ASK and KINDL, positive correlations were observed between ASKp and ASKc and all the KINDL dimensions, with the exception of the physical well-being dimension. Most of these correlations were low and/or moderate (Table 4).
ASK vs KINDL (n=57).
| Kindla | PWB | EWB | SE | FM | FR | SC | TT | |
|---|---|---|---|---|---|---|---|---|
| ASKp | r | 0.023 | 0.559 | 0.538 | 0.386 | 0.624 | 0.343 | 0.631 |
| p | 0.867 | 0.000 | 0.000 | 0.003 | 0.000 | 0.009 | 0.000 | |
| ASKc | r | 0.093 | 0.464 | 0.396 | 0.386 | 0.440 | 0.292 | 0.523 |
| p | 0.493 | 0.000 | 0.002 | 0.003 | 0.001 | 0.027 | 0.000 |
ASK, Activities Scale for Kids.
Regarding the internal consistency of ASK Portuguese version, acceptable values were found for both for ASKp and ASKc.
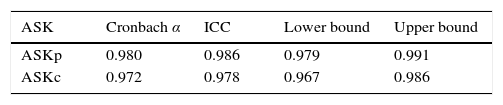
The reproducibility values of ASKp and ASKc were also found to be acceptable (Table 5), after the questionnaires were completed twice, one or two weeks apart.
DiscussionConsidering the results from the consensus panels, clinical review panel, and the panels of children and parents, it can be affirmed that semantic and content equivalence between the translated version of ASK and the original version were reached.
In general, this measure was considered clear, understandable, and appropriate for a pediatric population. The only downside was the fact that it is a relatively extensive measure, especially when applying both versions together, as shown by the mean time for completion of the two versions (33.4min). The authors conclude that the Portuguese version of ASK presents an acceptable level of content validity.
Regarding the existence of support received by children to move, it was observed that both in ASKp and ASKc, the majority of individuals (between 53% and 56%) reported not to use any support for moving both indoors and outside. These findings appear to indicate a correlation between what children really do in their day-to-day and what they think they can do.
To assess the validity of ASK, the authors assumed that it could allow to discriminate among different levels of capability (ASKc) and performance (ASKp) among groups that would hypothetically have these differences. These hypotheses were confirmed between individuals using or not any type of support to move, for both versions of ASK. Therefore, individuals who used support to move are expected to show a lower degree of functionality and therefore have lower scores in ASK (Table 3).
It was also expected to find statistically significant differences between children with musculoskeletal disorders and children with neuromuscular conditions, assuming that neuromuscular conditions result in more incapacitating stages.5 The results obtained for both versions of ASK did not reject this hypothesis.
For the assessment of validity, the relations between ASK and KINDL were also analyzed. The assumption was the existence of positive correlation values between the confronted constructs, supporting the hypothesis that more favorable health conditions should correspond to better levels of capacity and performance.
The choice of KINDL was due to the lack of a standard measure suitable for the Portuguese language and culture. Furthermore, a Portuguese version of the KINDL is available, covering the required ages. Additionally, a similar strategy was used in the study of the original version.2
When analyzing the values of the correlations between KINDL Total and both ASKp and ASKc scores, the existence of positive and moderate correlations was observed (Table 5), thus confirming the hypothesis that children with better degree of functionality also present a better level of quality of life. A correlation of the two versions of ASK with all dimensions of the KINDL was also observed, except for the physical well-being dimension. To try to explain this finding, the authors compared the questions of the physical well-being dimension of KINDL and the items of the ASK, and observed that the four questions of physical well-being dimension of KINDL regard feeling ill, body aches, tired, or strong, while the items of ASK are related with the performance of daily activities. However, the KINDL physical dimension can match concepts in some way different from ASK ones. In turn, the fact that the sample comprised approximately 18% individuals with cerebral palsy may represent a bias in the results. It is known that children tend to overvalue their health status, in particular those with cerebral palsy, who have a different expectation in relation to their physical abilities in comparison to individuals who have an acquired disability.
Despite not including questions related to KINDL emotional well-being and self-esteem dimensions, the correlation values obtained for both ASKp and ASKc, albeit weak to moderate, were acceptable (Table 4). These values can be justified by the difference of constructs and by the fact that the sample was composed of children who perceived their incapacities as slight to moderate, leading to the hypothesis of good levels of self-esteem and emotional well-being. Bjorson13 corroborates this assumption, evidencing that the performance of activities positively influence physical health, behavior, and emotional condition in children with cerebral palsy.
In the family dimension, there was a weak correlation for both ASKp and ASKc (r=0.386). This type of correlation was already expected, since ASK does not consider issues directly related to the family. In the friends dimension, moderate correlation values (r between 0.624 and 0.440) were observed for both ASKc and ASKp. This result was expected, given that ASK has questions that directly focus on the child's friends. Finally, in the school dimension, only a weak correlation with ASKp was observed (r=0.343), something that was also expected, since ASK does not present questions related to school performance.
Regarding the internal consistency and reproducibility of ASK, the results showed acceptable values. The values of the ICC obtained for both ASKc (ICC=0.978) and ASKp (ICC=0.986) were in agreement, representing a high reproducibility according to the criteria previously listed.25 When compared with the reproducibility levels of the original version, it was verified that the results of the test–retest were consistent, since the value of the ICC in the original study was 0.97 for both versions.2,6 It can be considered that the Portuguese version of ASK shows good levels of reproducibility.
Regarding internal consistency, results for each ASK version (α=0.980 for ASKp and α=0.972 for ASKc) were similar to the original results, which were considered to be high.25 These figures suggest that all items of the scale measure the same constructs.
The main limitations of this study were related to the extension of the protocol used, including both ASK versions, KINDL questionnaire, and socio-demographic questions. Furthermore, the sample size did not allow for the performance of a factor analysis to test the construct validity.
Given the results, the authors conclude that the Portuguese ASK versions present semantic and content equivalences with the original version, as well as acceptable values of validity and reliability. Finally, they propose further studies to deepen the present findings and to further explore the psychometric characteristics of the measure, including the assessment of its responsiveness.
The authors consider that the Portuguese ASK versions can be used both in clinical practice and research.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the staff from the health care institutions. Furthermore, the children and parents who participated in this study deserve deep recognition.
Please cite this article as: Paixão D, Cavalheiro LM, Gonçalves RS, Ferreira PL. Portuguese cultural adaptation and validation of the Activities Scale for Kids (ASK). J Pediatr (Rio J). 2016;92:367–73.
Study conducted at Polytechnic Institute of Coimbra, Coimbra Health School, Coimbra, Portugal.




