

To estimate the past-year prevalence of parental use of verbal and physical discipline in an urban sample.
MethodA cross-sectional study was conducted in two underprivileged neighborhoods with nearly 80,000 inhabitants. Complex sampling was used. The households were selected by applying two-stage probabilistic sampling with stratification. A total of 401 households (sample error=0.1) were selected by maximizing the variance (p=0.5). The cluster sampling indicated 33 census units (sample error=0.05). The Brazilian Portuguese version of the WorldSAFE Core Questionnaire was used to assess parental use of moderate verbal discipline, harsh verbal discipline, moderate physical discipline, and harsh physical discipline. This questionnaire asks how often mothers (respondent) and/or their husband or partner use specific disciplinary tactics.
ResultsThe mean age of children and adolescents was 9 years (SD: 4.5). The prevalence of harsh verbal discipline was approximately 37% (28.3% [95% CI: 23.4–33.3%] for more than three times). The prevalence of harsh physical discipline was approximately 30% (21.8% [CI: 18.2–25.4%] for more than three times). Boys had higher odds of receiving harsh physical discipline [OR: 1.56, p<0.05]. Children and adolescents with learning problems and developmental delays had higher odds of being exposed to harsh discipline than their peers without these problems. Children and adolescents with chronic health conditions (e.g., asthma) had lower odds of receiving harsh physical discipline (OR: 0.4; p<0.05).
ConclusionsParental abuse was embedded within children and adolescents rearing practices in these two underprivileged neighborhoods.
Estimar a prevalência no último ano de crianças e adolescentes expostos a disciplinas físicas e verbais pelos pais e mães.
MetodologiaEstudo transversal conduzido em dois bairros vulneráveis que possuem aproximadamente 80.000 habitantes. Amostragem complexa foi utilizada. As casas foram selecionadas por amostragem probabilística em duas fases. O número de 401 casas (erro amostral=0,1) foi definido pela variância maximizada (p=0,5). A amostragem por cluster permitiu obter o total de 33 cluster selecionados (erro amostral=0.05). Usamos a versão brasileira do WorldSAFE Core Questionnaire para identificar disciplinas verbais moderadas, disciplinas verbais severas, disciplinas físicas moderadas e disciplinas físicas severas. O questionário pergunta a frequência que as mães (respondentes) e seus maridos/companheiros utilizaram táticas disciplinares especificas.
ResultadosA média de idade das crianças e adolescentes foi de nove anos (DP: 4,5). A prevalência de disciplinas verbais severas foi de aproximadamente 37% (sendo 28,3% [95% CI: 23,4–33,3%] expostas a mais de três vezes no último ano). A prevalência disciplinas físicas severas foi de aproximadamente 30% (sendo 21,8% [CI: 18,2–25,4%] expostas mais de três vezes). Meninos tem maior chance de disciplinas físicas severas [OR: 1,56, p<0,05]. Crianças e adolescentes com problemas de aprendizagem e atrasos no desenvolvimento apresentam maior chance quando comparado com seus pares sem problemas. Crianças e adolescentes com problema crônico de saúde tiveram chance menor de disciplinas físicas severas (OR: 0,4; p<0,05).
ConclusõesAbuso paterno e materno está contido nas práticas cotidianas de educação nestes dois bairros vulneráveis.
Child and adolescent (CA) protection has been greatly enhanced in the past century. After the 1924 Declaration of the Rights of the Child, a number of other actions followed, aiming to ensure the safe and healthy development of CAs at the international level.1 In Brazil, especially after the 1980s, many policies and regulations were implemented to guarantee the protection of CAs.2 These efforts were guided by the Statute of the Child and Adolescent, which indicates that family, community, and public authorities must ensure CA rights.
However, parental use of harsh physical and verbal discipline when raising CAs remains a global challenge across different social classes, cultures, languages, religions, and ethnicities.3 In a series of meta-analyses on the global prevalence of child maltreatment, the prevalence of physical abuse alone was estimated to be 22.6% (85% CI: 20.3–25.1) from self-reported accounts and 0.3% (85% CI: 0.1–1.2) from informant responses.4 Despite the efforts to reduce the number, severity, and consequences of parental abuse, a large number of CAs continue to be exposed to this abuse, especially among low-income families. Low income has been strongly associated with parental abuse (i.e., CAs living in families with limited economic resources are at higher risk of harsh discipline). However, it is not fully clear why and how these factors are associated.5 Additionally, CAs who are maltreated miss more school days than their peers who are not, and thus school performance might emerge as a sentinel event associated with parental abuse.6
Most studies on this topic have been conducted in Europe and in North America, and research from low- and middle-income countries, including Brazil, is lacking.4,7 Thus, studies that measure the extent of parental abuse in underprivileged regions are needed. In this article, the authors focused on the past-year prevalence of parental use of moderate and harsh verbal and physical discipline in an urban population. The study also investigated whether school performance and mothers’ perceptions of CA health are associated with any type of discipline.
MethodsDesign and samplingThis was a cross-sectional study in the surroundings of the federal capital of Brazil, Brasília. Two underprivileged neighborhoods in the city of Ceilândia were studied. According to the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística [IBGE]), these two neighborhoods have nearly 80,000 inhabitants and approximately 19,000 households, and were divided by the national census into 83 census units. This region is characterized by poor-quality housing and few resources including only one school, insufficient healthcare services, and unreliable public transportation.8 A complex sampling design was used to reflect the population structure in a representative sample; this type of design includes at least one of the following characteristics: (i) stratification, (ii) clustering, or (iii) unequal probability of selection.9 The stratum was defined by each of the two neighborhoods (Pôr do Sol and Sol Nascente). The census units represented the primary units (cluster), and households were the secondary unit. The cluster sampling approach led to the inclusion of 33 total census units (sample error=0.05).10 Households were selected by probabilistic two-stage cluster sampling with census unit stratification and selection probability proportional to size. The number of households was defined by maximizing the variance using a Bernoulli distribution (p=0.5).10 A total of 401 households were selected (sample error=0.1). This variance maximization approach was used because the prevalence of moderate and harsh discipline in these communities was unknown. Proportional sample allocation was applied to determine the distribution of census units and households. To cover a large spatial area in each region, the primary units in each neighborhood were selected using systematic sampling with probability of selection proportional to size.11 The households were selected by systematic sampling with equiprobability. The SURVEYSELECT Procedure from Statistical Analysis Software (SAS Institute Inc./STAT 2011, version 9.3, NC, USA) was used in the sampling.12 When more than one eligible woman or CA was present in a household, the participants were randomly selected by equal chance. The IBGE provided the geographic coordinates and maps for each census sector, enabling more accuracy in data collection. To confirm the use of sampling procedures, unannounced field visits were made and nearly 40% of participants were contacted to verify that they had actually participated in the data collection.
ParticipantsThe authors aimed to interview mothers of CAs (individuals up to 18 years old). When the mother was not the main individual responsible for the CA, the interview was conducted with the actual/legal female who had been responsible for the CA in the previous year. After identifying the selected households (401), the visits were initiated. When the selected respondent was not available at the time of initial contact, up to five callback visits were made to conduct the interview. A total of 397 women agreed to participate in this research.
Measurement toolsSocio-economic sample profileFamily's socioeconomic status was assessed using the classification system developed by the Brazilian Association of Market Research Companies (Associação Brasileira de Empresas de Pesquisa [ABEP]).13 Women were asked how difficult raising their CA was compared to raising other CAs (easy to take care of; the same as other CA; difficult to take care of). School attendance and performance in the past year were also assessed. Additionally, the mothers completed a series of yes or no questions, as follows: “Does she/he (referring to the CA) have any chronic health problems (such as asthma)?,” “Does she/he have any hearing, speaking or seeing disorders?,” “Does she/he have any physical impairments or disability?,” “Does she/he have any emotional or behavioral problems?,” “Does she/he have any developmental delays?,” “Does she/he have mental retardation?,” and “Does she/he have any learning problems?”
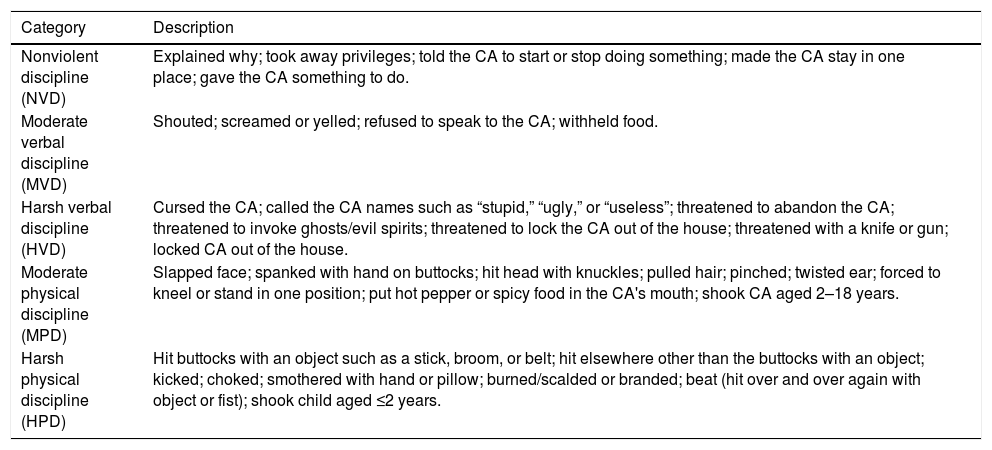
WorldSAFE core questionnaireTo assess the use of discipline, the Brazilian Portuguese version of the WorldSAFE core Questionnaire was used.14 This questionnaire was developed based on the Parent–Child Conflict Tactics Scale (PC-CTS) and on consensus among WorldSAFE steering committee members; the items included behaviors that were considered to reflect nonviolent discipline (NVD), moderate verbal discipline (MVD), harsh verbal discipline (HVD), moderate physical discipline (MPD), and harsh physical discipline (HPD) in several countries, including Brazil.15,16 The questionnaire asks how often mothers (respondent) and/or their husband or partner had used specific disciplinary tactics, with responses scored on a three-point scale of not at all, one or two times, and ≥3 times in the previous year (Table 1).
Categories of discipline methods and list of topics.
| Category | Description |
|---|---|
| Nonviolent discipline (NVD) | Explained why; took away privileges; told the CA to start or stop doing something; made the CA stay in one place; gave the CA something to do. |
| Moderate verbal discipline (MVD) | Shouted; screamed or yelled; refused to speak to the CA; withheld food. |
| Harsh verbal discipline (HVD) | Cursed the CA; called the CA names such as “stupid,” “ugly,” or “useless”; threatened to abandon the CA; threatened to invoke ghosts/evil spirits; threatened to lock the CA out of the house; threatened with a knife or gun; locked CA out of the house. |
| Moderate physical discipline (MPD) | Slapped face; spanked with hand on buttocks; hit head with knuckles; pulled hair; pinched; twisted ear; forced to kneel or stand in one position; put hot pepper or spicy food in the CA's mouth; shook CA aged 2–18 years. |
| Harsh physical discipline (HPD) | Hit buttocks with an object such as a stick, broom, or belt; hit elsewhere other than the buttocks with an object; kicked; choked; smothered with hand or pillow; burned/scalded or branded; beat (hit over and over again with object or fist); shook child aged ≤2 years. |
CA, children or adolescent.
All analyses were conducted using SAS/STAT (2011) version 9.3. The following analyses were performed while considering strata and cluster weights:
- 1.
Means and standard deviation (SD) were calculated to provide an overview of the participants’ profile.
- 2.
Prevalence and confidence intervals (CI) of the types of discipline used by both parents and by each parent were calculated.
- 3.
Logistic regression analysis was conducted to identify the factors associated with moderate and harsh discipline and the corresponding odds ratios (OR) and 95% confidence intervals (95% CI). To determine the significance, Wald's chi-squared test was applied.
This project was in line with the Declaration of Helsinki and national regulations (Resolução 466/2012). The study procedures were submitted to and approved by the Research Ethical Committee of the Medical Faculty at University of Brasilia (Case number: 1.521.672/2016), The interviewers were trained to prevent others from overhearing the participants’ responses. Thus, to maintain participants’ privacy and safety, all interviews were conducted individually. All participants signed a written informed consent.
ResultsOf the 401 households visited, four women (1%) refused to participate; therefore, a total of 397 women were included in the study. In 27 (6.8%) households, the biological mother did not live with the CA, and in 24 of these cases, the grandmother was the person responsible for the CA. The households contained the following number of CAs: one (2%), two (57.4%), three (26.9%), four (9.8%), five (2.8%), six (0.8%), and seven (1%). Approximately 10.4% of the families lived with an income higher than 2400.00 BRL (nearly 850 USD) per month, 63.3% lived with less than 2400.00 BRL and more than 1446.00 BRL (nearly 515 USD) per month, and 26% lived with less than 1446.24 BRL per month; this last group included most families with limited access to basic services and living assets. The mean age of CAs was 9 years (SD: 4.5), and a slightly larger percentage of girls (51%) was observed. Most CAs attended school (73.6%). However, approximately 4.1% (95% CI: 2.4–5.9%) of school-age CAs were not attending school, and 28.5% (23.6–33.4%) had failed in school in the previous year. It was observed that 13.5% had a chronic health problem (such as asthma); 6.1% had an auditory, speech, or vision disorder; 0.5% had a physical impairment or disability; 6.4% had emotional or behavioral problems; 4.2% had a developmental delay; 0.9% had mental retardation; and 6.2% had learning disorders.
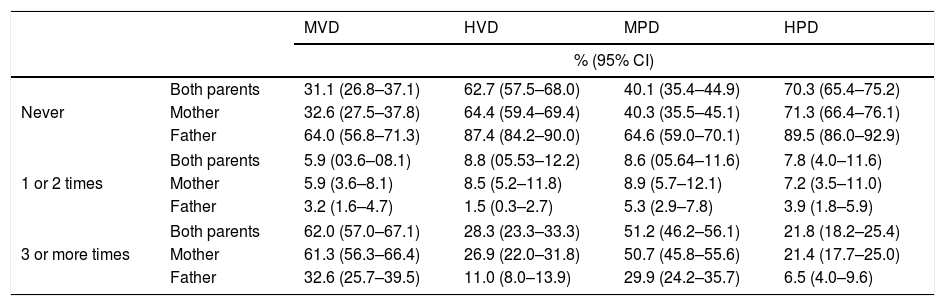
Most CA had been exposed to MVD and MPD more than three times in the past year, namely, 62.0% (95% CI: 57.0–67.1%) and 51.2% (46.2–56.1%), respectively. It was also observed that a large number of CAs had been exposed to HVD (28.3% [23.3–33.3%]) and HPD (21.8% [18.2–25.4%]). Mothers used moderate and harsh forms of physical and verbal discipline more frequently than fathers (Table 2).
Estimated prevalence of different forms of discipline (%; 95% CI).
| MVD | HVD | MPD | HPD | ||
|---|---|---|---|---|---|
| % (95% CI) | |||||
| Never | Both parents | 31.1 (26.8–37.1) | 62.7 (57.5–68.0) | 40.1 (35.4–44.9) | 70.3 (65.4–75.2) |
| Mother | 32.6 (27.5–37.8) | 64.4 (59.4–69.4) | 40.3 (35.5–45.1) | 71.3 (66.4–76.1) | |
| Father | 64.0 (56.8–71.3) | 87.4 (84.2–90.0) | 64.6 (59.0–70.1) | 89.5 (86.0–92.9) | |
| 1 or 2 times | Both parents | 5.9 (03.6–08.1) | 8.8 (05.53–12.2) | 8.6 (05.64–11.6) | 7.8 (4.0–11.6) |
| Mother | 5.9 (3.6–8.1) | 8.5 (5.2–11.8) | 8.9 (5.7–12.1) | 7.2 (3.5–11.0) | |
| Father | 3.2 (1.6–4.7) | 1.5 (0.3–2.7) | 5.3 (2.9–7.8) | 3.9 (1.8–5.9) | |
| 3 or more times | Both parents | 62.0 (57.0–67.1) | 28.3 (23.3–33.3) | 51.2 (46.2–56.1) | 21.8 (18.2–25.4) |
| Mother | 61.3 (56.3–66.4) | 26.9 (22.0–31.8) | 50.7 (45.8–55.6) | 21.4 (17.7–25.0) | |
| Father | 32.6 (25.7–39.5) | 11.0 (8.0–13.9) | 29.9 (24.2–35.7) | 6.5 (4.0–9.6) | |
MVD, such as screaming or yelling, and MPD, such as spanking on the buttocks, were the most frequently used forms of discipline by parents in this sample (Fig. 1).

Parents’ use of moderate discipline significantly increased the odds of harsh discipline. Compared to parents who did not use MPD, those who used MPD had higher odds of HVD (OR: 10.0; p<0.01). Similarly, parents who used MVD had higher odds of HPD (OR: 3.7; p<0.01) and those who used HVD presented higher odds of HPD (OR: 6.8; p<0.01).
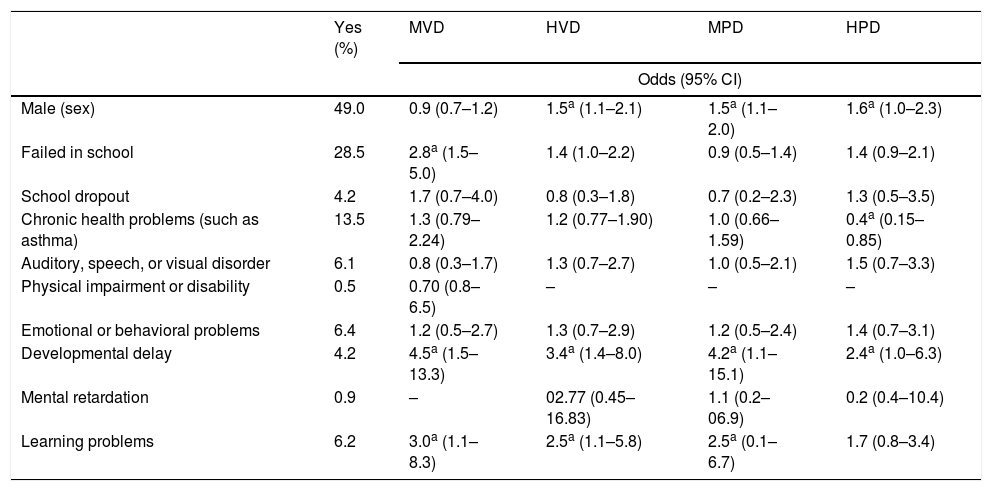
Boys were more often the subject of abuse. In these two communities, being male presented higher odds of being exposed to HVD, MVD, or HVD. Mothers’ perceptions or knowledge of CAs’ auditory, speech, or vision disorder, physical impairments, mental retardation, or emotional or behavioral problem was not significantly associated with moderate or harsh discipline, neither reducing nor increasing the odds. However, parents of CAs with learning disorders had higher odds of using MVD, HVD, and MPD. Developmental delay was associated with higher odds of HVD, MPD, and HPD. Mothers’ perception or knowledge of a chronic health problem reduced the odds of HPD by 60% (85–15%; Table 3).
Factors associated with the use of moderate and harsh forms of discipline by both parents.
| Yes (%) | MVD | HVD | MPD | HPD | |
|---|---|---|---|---|---|
| Odds (95% CI) | |||||
| Male (sex) | 49.0 | 0.9 (0.7–1.2) | 1.5a (1.1–2.1) | 1.5a (1.1–2.0) | 1.6a (1.0–2.3) |
| Failed in school | 28.5 | 2.8a (1.5–5.0) | 1.4 (1.0–2.2) | 0.9 (0.5–1.4) | 1.4 (0.9–2.1) |
| School dropout | 4.2 | 1.7 (0.7–4.0) | 0.8 (0.3–1.8) | 0.7 (0.2–2.3) | 1.3 (0.5–3.5) |
| Chronic health problems (such as asthma) | 13.5 | 1.3 (0.79–2.24) | 1.2 (0.77–1.90) | 1.0 (0.66–1.59) | 0.4a (0.15–0.85) |
| Auditory, speech, or visual disorder | 6.1 | 0.8 (0.3–1.7) | 1.3 (0.7–2.7) | 1.0 (0.5–2.1) | 1.5 (0.7–3.3) |
| Physical impairment or disability | 0.5 | 0.70 (0.8–6.5) | – | – | – |
| Emotional or behavioral problems | 6.4 | 1.2 (0.5–2.7) | 1.3 (0.7–2.9) | 1.2 (0.5–2.4) | 1.4 (0.7–3.1) |
| Developmental delay | 4.2 | 4.5a (1.5–13.3) | 3.4a (1.4–8.0) | 4.2a (1.1–15.1) | 2.4a (1.0–6.3) |
| Mental retardation | 0.9 | – | 02.77 (0.45–16.83) | 1.1 (0.2–06.9) | 0.2 (0.4–10.4) |
| Learning problems | 6.2 | 3.0a (1.1–8.3) | 2.5a (1.1–5.8) | 2.5a (0.1–6.7) | 1.7 (0.8–3.4) |
–, The number of observations was not sufficient for the analysis.
Most mothers reported that their CA was easier to look after than other CAs (69.2%), 17.8% perceived that caring for their CA was the same level of difficulty as caring for other CAs, and 12.8% found that it was more difficult to take care of their CA than other CAs. CAs who were considered more difficult to raise had higher odds of MPD (OR: 5.3, p<0.0001) and HPD (OR: 3.1, p<0.0001) than those who were considered easier to raise or the same level of difficulty.
DiscussionIn this article, the authors estimated the proportions of parental use of discipline in two underprivileged neighborhoods in the Federal District, Brazil, using an urban informant sample. A very high one-year prevalence of parental abuse was observed. Screaming/yelling and spanking were the most common and frequent forms of verbal and physical discipline, respectively. MVD and MPD were shown to significantly increase the odds of HPD.
Other studies have found that moderate discipline is a risk factor for parental abuse.17 This association presents a challenge regarding how parental use of different forms of discipline become a professional matter or remain a private issue, as disciplinary behaviors can be considered normative, adequate forms of parenting despite being harsh or abusive.4 Previous studies have claimed that pediatricians and healthcare professionals should be trained not only in identifying cases of maltreatment but also in preventing them. An effective way of preventing this type of behavior is by strengthening families and promoting safe, stable, and nurturing relationships during consultations and home visits.18,19
The global prevalence of parental physical and emotional abuse based on informant samples has been estimated to be 0.3% (85% CI: 0.1–1.2%) and 0.3% (85% CI: 0.2–0.6%), respectively.4 The combined prevalence of physical abuse from eight informant studies in South America indicated a similar prevalence of 0.4% (85% CI: 0.1–1.4%), which is strikingly lower than the prevalence of 22.6% (85% CI: 20.3–25.1%) identified in studies using self-reported data from this region.4 A much higher one-year prevalence of physical abuse was observed in this informant sample than in other informant studies. The prevalence of physical abuse (i.e., HPD) based on an informant sample of mothers was approximately 30%, which is comparable to and even higher than the prevalence rates found in previous self-report studies.4,7
This higher figure might be related to the social context; underprivileged neighborhoods can lack resources, and severe stress can lead to high-risk parenting. Other researchers in Brazil have found lower prevalence rates of HPD in underprivileged neighborhoods using informant samples (e.g., 10.1%, k=89, informant sample, urban, underprivileged neighborhood15; 20%, k=813 informant sample, urban, underprivileged neighborhood).20 Thus, the higher one-year prevalence in the present study appears to corroborate the notion that economic limitations have negative associations with parental abuse, as suggested elsewhere.21
As in other studies, mothers used moderate and harsh forms of discipline more frequently than fathers.22,23 However, instead of being blamed, women should receive appropriate health support. Parents’ motivations for using moderate and harsh forms of discipline tend to be similar to the reasons for using NVD (i.e., parents want to teach their children right from wrong). Research indicates that poor mental health and overburden among mothers within a household can lead to the use of harsh discipline.24 Thus, pediatricians and allied health professionals should promote mental health among women.25
In this sample, most of the disabilities and health conditions did not significantly increase or decrease the odds of a specific discipline. In contrast to previous findings, a lower prevalence of harsh punishment was observed in CAs with disabilities.26 In this sample, CAs with a chronic health problem had lower odds of being the subject of abuse.
However, CAs with developmental delays and learning problems presented higher odds of receiving moderate and harsh punishment. Thus, CAs with developmental delays should receive systematic monitoring and assessment of risk factors, specifically through primary care services.27 The trend identified in the present study is worrisome, as CAs tend to experience reduced academic development when exposed to abuse, which can lead to a cycle of school failure and domestic abuse.28 In fact, there is a strong relationship between harsh discipline and internalizing problems, which have been related to lower working memory capacity and school performance.29 In this research, it was observed that a large number of CAs were exposed to parental abuse and underachieved in school; however, these factors were not significantly associated. This lack of significance indicates that CA underachievement might be related to other variables (e.g., lack of schools in the neighborhood). Indeed, school mobility has been identified as a risk factor for underachievement.30
To the best of the authors’ knowledge, this is the first study on parental use of different forms of discipline among a representative urban sample in the Midwest region of Brazil, and this study is among the very few conducted on this topic in the country. This study provides data on parental rearing practices and presents a solid methodological approach to estimating the prevalence of parental abuse. However, some limitations should be acknowledged. The information reported by mothers may have been biased by their concerns and fears of sharing domestic information. Additionally, the quality of information on CA health based on mothers’ perceptions is limited, and the results should thus be interpreted with caution; research using standardized instruments should be conducted. Further research focusing on self-reported data is needed, given the substantial gap between the prevalence identified in self-report studies and the prevalence in studies using informants.4,7
In sum, CAs in these two neighborhoods were highly exposed to moderate and harsh forms of discipline. In this sense, parental abuse is embedded within CA rearing practices in these two underprivileged neighborhoods.
FundingFundação de Apoio à Pesquisa do Distrito Federal.
Conflicts of interestThe authors declare no conflicts of interest.
VS would like to acknowledge Prof. Dr. Isabel Altenfelder Santos Bordin for suggesting and sharing key references and materials for this research. The authors are grateful to all of the women who participated in this study.
Please cite this article as: Santos V, Silva PH, Gandolfi L. Parents’ use of physical and verbal punishment: cross-sectional study in underprivileged neighborhoods. J Pediatr (Rio J). 2018;94:511–7.
Study conducted at Universidade de Brasília (UnB), Faculdade de Medicina, Brasília, DF, Brazil.




