

To describe and analyze indicators of feeding practices related to breastfeeding and factors associated with exclusive breastfeeding (EBF) in a subnormal urban cluster (slums) in Pernambuco, Brazil.
MethodsFour breastfeeding indicators were used to interview mothers of children under 3 years of age. An inventory of the families’ socioeconomic and environmental factors, maternal obstetric history, and basic health care access was undertaken. The sample consisted of all 310 children under the age of 3 years from Coelhos, PE, Brazil. Spearman's correlation was carried out, as well as crude and adjusted prevalence ratios for a final statistical model that showed associated factors with the main outcome at a level of 0.05.
ResultsThe prevalence of breastfeeding in the first hour of life, exclusive breastfeeding up to 6 months, continued breastfeeding at 1 year, and continued breastfeeding at 2 years were 60.2%, 32.9%, 45.9, and 35.9%, respectively. A correlation was observed between start of pacifier use and duration of either exclusive (rs=0.358 [p<0.001]) or non-exclusive breastfeeding (rs=0.248 [p=0.006]). Maternal age over 35 years (p<0.001), home visit in the first week after birth (p=0.003), having had a male baby (p=0.029), and not using a pacifier (p<0.001) remained protective factors in the final model.
ConclusionThe prevalence rates of exclusive breastfeeding at 6 months were well above the results obtained by other Brazilian authors. Home visit and maternal age prevailed as protective factors, while pacifier use was shown to be a discouraging practice.
Descrever e analisar indicadores das práticas relacionadas ao aleitamento materno e fatores associados ao aleitamento materno exclusivo em um aglomerado urbano subnormal (favela) em Pernambuco.
MétodosForam usados quatro indicadores do aleitamento materno mediante entrevista com as mães de menores de três anos. Fez-se um inventário de fatores socioambientais das famílias, antecedentes obstétricos e acesso às ações básicas de saúde. A amostra inclui todas as 310 crianças da Comunidade de Coelhos, PE, Brasil. Feitas correlação de Spearman e razões de prevalências brutas e ajustadas que compuseram um modelo estatístico final que evidenciou os fatores associados ao principal desfecho ao nível de 0,05.
ResultadosA prevalência do aleitamento materno na primeira hora de vida, aleitamento materno exclusivo aos 6 meses, amamentação continuada até um ano e dois anos foram, respectivamente, 60,2%, 32,9%, 45,9% e 35,9%. Na correlação entre o início do uso de chupeta e a duração do aleitamento, exclusivo ou não, obtiveram-se respectivamente os coeficientes rs=0,358 (p < 0,001) e rs=0,248 (p = 0,006). No modelo final permaneceram como fatores de proteção: a idade materna acima de 35 anos (p < 0,001), a visita domiciliar na primeira semana de vida (p = 0,003), o sexo masculino (p = 0,029) e o não uso da chupeta (p < 0,001).
ConclusãoOs índices de prevalência do aleitamento materno exclusivo aos 6 meses foram bem superiores aos resultados obtidos por outras pesquisas nacionais. A visita domiciliar e a idade materna prevaleceram como fatores de proteção e o uso de chupeta como uma prática desestimulante.
While acknowledging the great advances in technologies for the production, processing, conservation, and preparation of foods for children in the first months and years of life, the consensus is that there is no ideal substitute for maternal breastfeeding (BF).1–6
In this sense, the World Health Organization (WHO)7 proposes standardized concepts and indicators for the study of the feeding practices in children, considering maternal BF in the first hour of life; exclusive breastfeeding (EBF) in children under 6 months; continued BF up to 1 year; and continued BF up to 2 years of age.
Probably in response to the consensuses and actions of international agencies and the adherence of governments and society's own movements in several countries, in 2016 the United Nations Children's Fund (UNICEF) described remarkable advances in BF practices worldwide, as exemplified by the rate of 44% of maternal BF in the first hour of life, 39% of EBF in children under 6 months, and 49% of continued BF up to 2 years of age.8 In Brazil, this scenario is no different, except for continued BF up to 2 years (26%).8 In the Northeast of Brazil, EBF in children under 6 months is 37% and, in the city of Recife, 38.3%.9
These descriptive data are very often discrepant, hindering comparative inferences for the definition of baselines and temporal, geographic, and social trends. Such inconsistencies result from different ways of collecting, analyzing, and presenting results. Thus, the prevalence of EBF, the most important indicator of BF behavior, is sometimes measured in children younger than 6 months8,9 and, in other cases, in children aged 6 months.10
In isolation, this observation is valid as a justification to apply conceptual fundamentals and the construction of standardized, reliable, and comparable indicators in time, space, and in relation to the assessed populations.
Under the analytical aspect, several factors can have different effects on the practice of BF, such as population's culture, social, and political organization, and economic and environmental conditions, among others.4,9,11–17 It has been reported that wealthier countries have a shorter EBF duration.8 A better income level is often associated with a higher maternal level of schooling, a condition that may facilitate access to information on BF practices. In turn, mothers with lower family income and/or informal occupation need to contribute to the family budget, making BF more difficult.4,13
Moreover, in poorer socioeconomic settings, such as in slums, children are more exposed to disease-causing agents.8 In this context, BF, especially EBF, with its protective properties, is crucial for the healthy development of these children.1–5
It is important to consider that, due to the demographic expression of subnormal urban clusters in Brazil (over 11 million people),18 and the scarcity and inconsistency of studies applied to these urban ecosystems, it is important to estimate the prevalence of indicators for feeding practices related to maternal BF and to identify factors associated with EBF at 6 months of age.
Considering the analytical interest, this study aimed to verify the hypothesis that mothers and children who meet the EBF requirement at six months are differentiated by diverse factors, such as the child's gender, maternal age and level of schooling, type of housing, prenatal care, type of delivery, home visit, and the use of pacifiers in the cases that do not reach the goal proposed by the United Nations.
MethodsThis was a cross-sectional, analytical study, based on the research database “Child development in a subnormal urban cluster (favela) of Recife, Pernambuco.”19 This research was carried out as an extension and update of a baseline survey carried out in a slum population, where the proposal of a formal primary health care (PHC) institution was first implemented in the traditional community of Coelhos, in Pernambuco, Brazil.
The study was a census-based research and included the data collection from all children aged 0–36 months enrolled in the two PHC linked to the Family Health Strategy (FHS). The study was carried out through interviews in the households, with the mothers of the children or their legal guardians. Exceptionally, some mothers were interviewed in the PHC, either because of risk situations or due to work.
Although the study was a census-based research, an a posteriori analysis was performed to calculate whether the sample collected had enough power to identify an association between the variables “received home visit in the first week of life” (power of 93.3%); “pacifier use” (power of 99.9%); “maternal age”, comparing the age group of 36 years with 13–19 years (power 74%); and “gender”, with power of 36.7%.
The WHO recommendations were considered for the characterization of the indicators and prevalence calculation.20 Thus, early start of BF corresponds to the proportion of children born in the last 24 months prior to the interview who were breastfed within the first hour of life; EBF in children under 6 months, the proportion of children aged 0–5 months who were receiving EBF at the time of the interview, based on the child's feeding during the 24h prior to the interview; continued BF up to 1 year, the proportion of children aged 12–15 months being breastfed; and continued BF up to 2 years, the proportion of children aged 20–23 months who were being breastfed at the time of the interview.
The study endpoint was EBF at 6 months, while the explanatory variables were grouped in: sociodemographic, obstetrical, and biological data of the children; home visit by the nurse together with a community health agent in the first week of life; and information about the use of pacifiers (non-nutritive sucking habit made available to the child all the time or to soothe the baby). Children who never used pacifiers were compared with those who had used. The socioeconomic status was evaluated according to the model of the Brazilian Association of Survey Companies (Associação Brasileira de Empresas de Pesquisa [ABEP]), 2014.21
The Stata program (Stata Statistical Software: release 12 – College Station, TX, United States) was used for the statistical analysis of data. Absolute and relative values of the assessed population, their characteristics, and the distributions of the variables of interest were calculated through measures of central tendency and dispersion. Spearman's correlation was used to evaluate the association between the start of pacifier use and duration of BF. To identify factors associated with EBF at 6 months, univariate Poisson regression was initially performed, estimating the crude prevalence ratios (PR) and their respective 95% confidence intervals (95% CI). At this stage, the variables that showed a p-value <0.20 were included in the multivariate analysis, estimating the adjusted PR and 95% CI. For the analyses of statistical significance in the final model, a p-value <5% was considered. The study was approved by the Research Ethics Committee, as formalized in the protocol CAEE No. 54705416.0.00005220.
ResultsA total of 310 children were studied in two primary care units linked to FHS: Coelhos I, with 111 children (35.8%) and Coelhos II, with 199 children (64.2%); the median total duration of BF in the two units was 182 days, with an interquartile range of 89–464 days, while the median EBF duration was 91 days, limited by the first and third quartiles, P25 and P75 (45–182 days). The use of pacifiers was reported for 147 children (47.4%).
Regarding the prevalence of BF indicators, the rate of BF in the first hour of life was 60.2% and the rate of EBF in children under 6 months was 46.3%; continued BF up to 1 year of life was 45.9% and up to 2 years, 35.9%.
Fig. 1 presents the association between the start of pacifier use and BF duration. A significant and increasing monotonic association between start of pacifier use and duration of EBF is observed in Fig. 1A (Spearman's correlation coefficient: r=0.51, p<0.001). Fig. 1B also shows a significant monotonic association between the start of pacifier use and duration of BF, regardless of the BF type (r=0.35, p<0.001).
 and the total breastfeeding duration (B) in children under 3 years of age living in the slum areas of the Brazilian Northeast assisted by the Health Family Strategy (HFS), 2015.")
Of the 310 children in the study, 236 (76.1%) were older than or 6 months of age and of those, excluding those who were never breastfed (12) and those for whom there was no information on EBF (five), 219 completed the survey, with a prevalence of EBF at six months of age of 32.9% (72/219 children). The possible association of factors with EBF was studied in this sample.
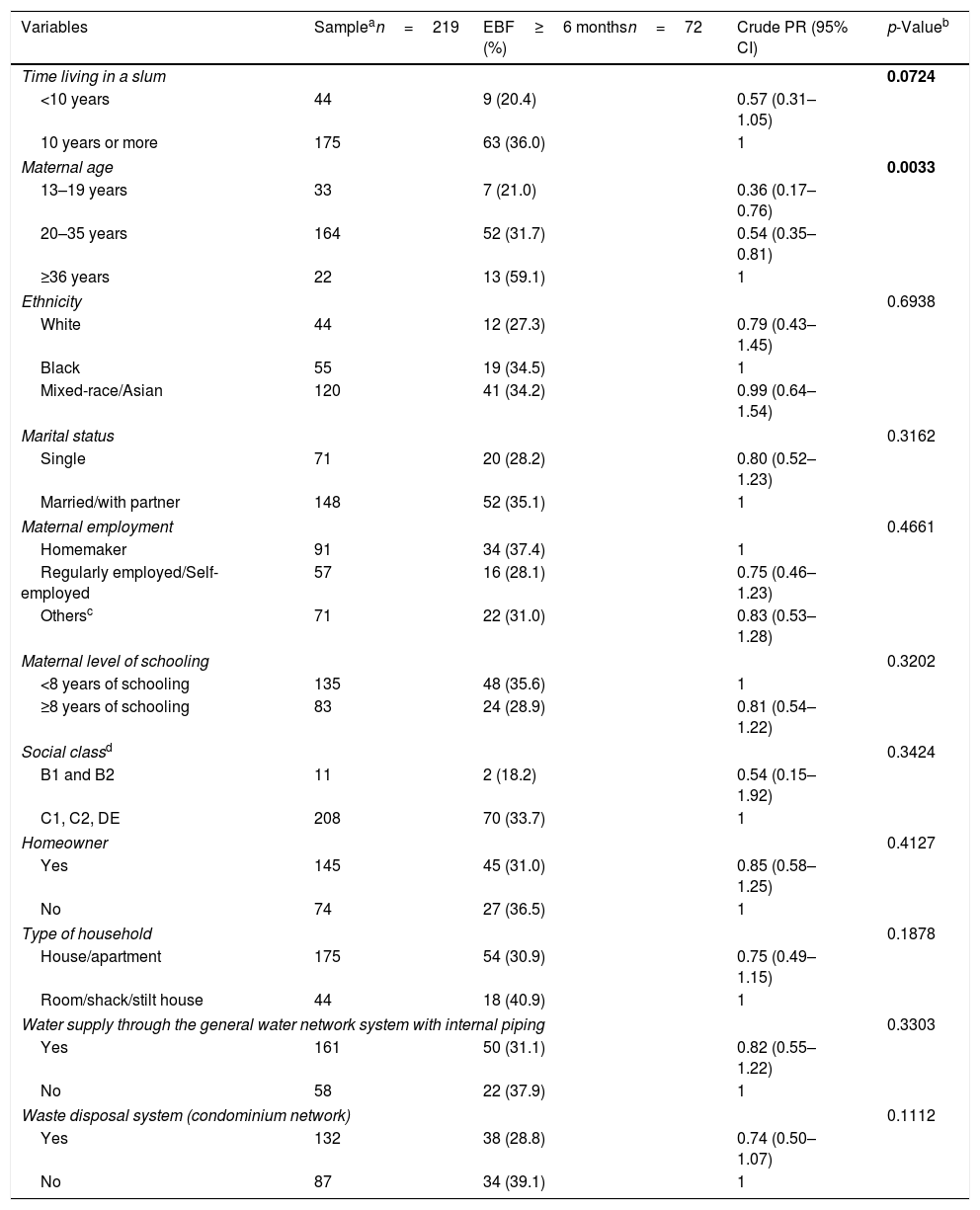
Table 1 shows the univariate analyses for the EBF condition at six months, according to maternal sociodemographic variables and housing conditions of families and children aged 6 months or older, totaling 11 variables (time living in the community, maternal age, ethnicity, marital status, maternal employment, maternal education, social status, homeowner, type of housing, water supply through the general water network system with internal piping, and waste disposal). It was observed that only maternal age (36 years and older) was statistically associated (p<0.0033) with EBF.
Univariate analyses for the exclusive breastfeeding condition at 6 months of age, according to the sociodemographic and maternal variables of the children living in the slum areas in the Brazilian Northeast and assisted by the Family Health Strategy (FHS). Recife – PE, 2015.
| Variables | Samplean=219 | EBF≥6 monthsn=72 (%) | Crude PR (95% CI) | p-Valueb |
|---|---|---|---|---|
| Time living in a slum | 0.0724 | |||
| <10 years | 44 | 9 (20.4) | 0.57 (0.31–1.05) | |
| 10 years or more | 175 | 63 (36.0) | 1 | |
| Maternal age | 0.0033 | |||
| 13–19 years | 33 | 7 (21.0) | 0.36 (0.17–0.76) | |
| 20–35 years | 164 | 52 (31.7) | 0.54 (0.35–0.81) | |
| ≥36 years | 22 | 13 (59.1) | 1 | |
| Ethnicity | 0.6938 | |||
| White | 44 | 12 (27.3) | 0.79 (0.43–1.45) | |
| Black | 55 | 19 (34.5) | 1 | |
| Mixed-race/Asian | 120 | 41 (34.2) | 0.99 (0.64–1.54) | |
| Marital status | 0.3162 | |||
| Single | 71 | 20 (28.2) | 0.80 (0.52–1.23) | |
| Married/with partner | 148 | 52 (35.1) | 1 | |
| Maternal employment | 0.4661 | |||
| Homemaker | 91 | 34 (37.4) | 1 | |
| Regularly employed/Self-employed | 57 | 16 (28.1) | 0.75 (0.46–1.23) | |
| Othersc | 71 | 22 (31.0) | 0.83 (0.53–1.28) | |
| Maternal level of schooling | 0.3202 | |||
| <8 years of schooling | 135 | 48 (35.6) | 1 | |
| ≥8 years of schooling | 83 | 24 (28.9) | 0.81 (0.54–1.22) | |
| Social classd | 0.3424 | |||
| B1 and B2 | 11 | 2 (18.2) | 0.54 (0.15–1.92) | |
| C1, C2, DE | 208 | 70 (33.7) | 1 | |
| Homeowner | 0.4127 | |||
| Yes | 145 | 45 (31.0) | 0.85 (0.58–1.25) | |
| No | 74 | 27 (36.5) | 1 | |
| Type of household | 0.1878 | |||
| House/apartment | 175 | 54 (30.9) | 0.75 (0.49–1.15) | |
| Room/shack/stilt house | 44 | 18 (40.9) | 1 | |
| Water supply through the general water network system with internal piping | 0.3303 | |||
| Yes | 161 | 50 (31.1) | 0.82 (0.55–1.22) | |
| No | 58 | 22 (37.9) | 1 | |
| Waste disposal system (condominium network) | 0.1112 | |||
| Yes | 132 | 38 (28.8) | 0.74 (0.50–1.07) | |
| No | 87 | 34 (39.1) | 1 | |
EBF, exclusive breastfeeding; PR, prevalence ratio.
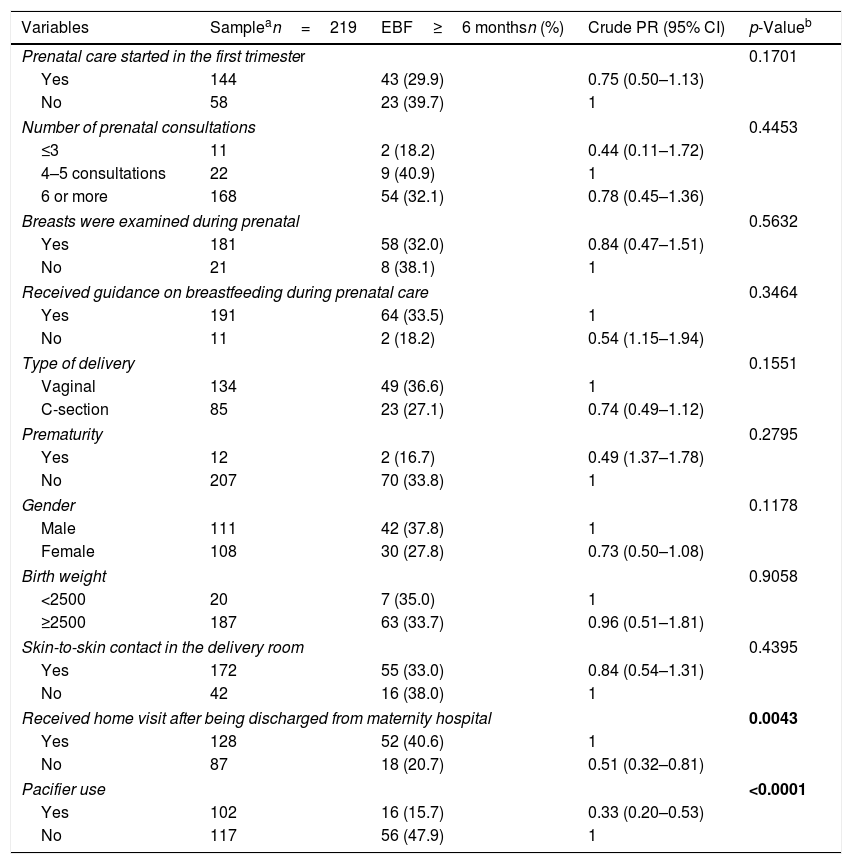
Table 2 shows the univariate analyses for EBF at 6 months, according to obstetric history and other maternal variables, as well as biological variables of the child, home visit in the first week of life, information on BF and use of pacifiers in children aged 6 months or older, totaling 11 adequately specified variables. Only the home visit in the first week of life (p=0.0043) was statistically associated as a protective factor for EBF, while pacifier use was a risk factor for the lower prevalence of EBF.
Univariate analyses for the exclusive breastfeeding condition at 6 months, according to the child's obstetric and biological antecedents and health actions of possible interest for the practice of EBF in children living in the slum areas in Northeast Brazil, Recife – PE, 2015.
| Variables | Samplean=219 | EBF≥6 monthsn (%) | Crude PR (95% CI) | p-Valueb |
|---|---|---|---|---|
| Prenatal care started in the first trimester | 0.1701 | |||
| Yes | 144 | 43 (29.9) | 0.75 (0.50–1.13) | |
| No | 58 | 23 (39.7) | 1 | |
| Number of prenatal consultations | 0.4453 | |||
| ≤3 | 11 | 2 (18.2) | 0.44 (0.11–1.72) | |
| 4–5 consultations | 22 | 9 (40.9) | 1 | |
| 6 or more | 168 | 54 (32.1) | 0.78 (0.45–1.36) | |
| Breasts were examined during prenatal | 0.5632 | |||
| Yes | 181 | 58 (32.0) | 0.84 (0.47–1.51) | |
| No | 21 | 8 (38.1) | 1 | |
| Received guidance on breastfeeding during prenatal care | 0.3464 | |||
| Yes | 191 | 64 (33.5) | 1 | |
| No | 11 | 2 (18.2) | 0.54 (1.15–1.94) | |
| Type of delivery | 0.1551 | |||
| Vaginal | 134 | 49 (36.6) | 1 | |
| C-section | 85 | 23 (27.1) | 0.74 (0.49–1.12) | |
| Prematurity | 0.2795 | |||
| Yes | 12 | 2 (16.7) | 0.49 (1.37–1.78) | |
| No | 207 | 70 (33.8) | 1 | |
| Gender | 0.1178 | |||
| Male | 111 | 42 (37.8) | 1 | |
| Female | 108 | 30 (27.8) | 0.73 (0.50–1.08) | |
| Birth weight | 0.9058 | |||
| <2500 | 20 | 7 (35.0) | 1 | |
| ≥2500 | 187 | 63 (33.7) | 0.96 (0.51–1.81) | |
| Skin-to-skin contact in the delivery room | 0.4395 | |||
| Yes | 172 | 55 (33.0) | 0.84 (0.54–1.31) | |
| No | 42 | 16 (38.0) | 1 | |
| Received home visit after being discharged from maternity hospital | 0.0043 | |||
| Yes | 128 | 52 (40.6) | 1 | |
| No | 87 | 18 (20.7) | 0.51 (0.32–0.81) | |
| Pacifier use | <0.0001 | |||
| Yes | 102 | 16 (15.7) | 0.33 (0.20–0.53) | |
| No | 117 | 56 (47.9) | 1 | |
EBF, exclusive breastfeeding; PR, prevalence ratio.
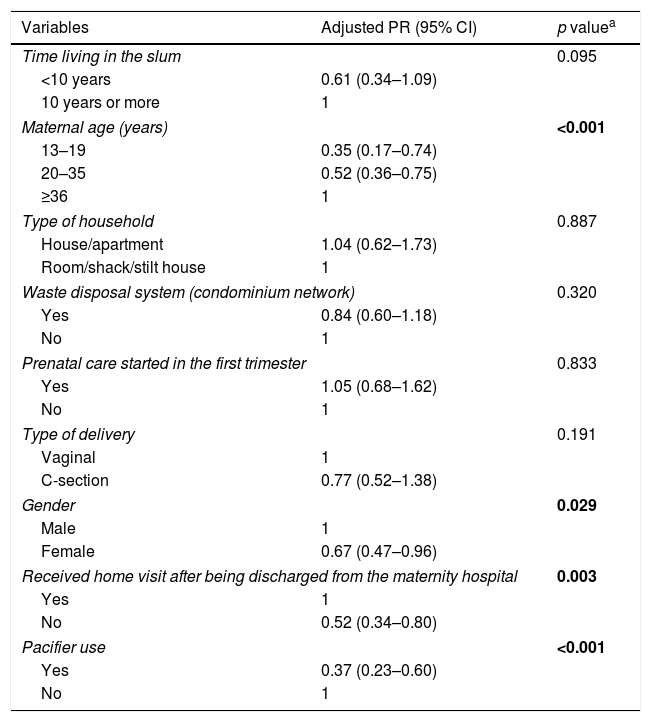
Of the 22 variables, nine showed p-values <20 in the univariate analysis (time living in the community, maternal age, type of housing, waste disposal, prenatal start in the first trimester, type of delivery, gender, home visit in the first week of life, and pacifier use), and were therefore included in the multivariate analysis. At this stage of the analysis, maternal age (p=0.0005), child's gender (p=0.029), home visit during the first week of life (p=0.003), and pacifier use (p<0.0001) were maintained in the model (Table 3).
Multivariate analyzes for the EBF status at 6 months, according to maternal and family sociodemographic variables, obstetric history, and other factors hypothetically related to the practice of EBF at 6 months of age in a slum area in Northeast Brazil, Recife – PE, 2015.
| Variables | Adjusted PR (95% CI) | p valuea |
|---|---|---|
| Time living in the slum | 0.095 | |
| <10 years | 0.61 (0.34–1.09) | |
| 10 years or more | 1 | |
| Maternal age (years) | <0.001 | |
| 13–19 | 0.35 (0.17–0.74) | |
| 20–35 | 0.52 (0.36–0.75) | |
| ≥36 | 1 | |
| Type of household | 0.887 | |
| House/apartment | 1.04 (0.62–1.73) | |
| Room/shack/stilt house | 1 | |
| Waste disposal system (condominium network) | 0.320 | |
| Yes | 0.84 (0.60–1.18) | |
| No | 1 | |
| Prenatal care started in the first trimester | 0.833 | |
| Yes | 1.05 (0.68–1.62) | |
| No | 1 | |
| Type of delivery | 0.191 | |
| Vaginal | 1 | |
| C-section | 0.77 (0.52–1.38) | |
| Gender | 0.029 | |
| Male | 1 | |
| Female | 0.67 (0.47–0.96) | |
| Received home visit after being discharged from the maternity hospital | 0.003 | |
| Yes | 1 | |
| No | 0.52 (0.34–0.80) | |
| Pacifier use | <0.001 | |
| Yes | 0.37 (0.23–0.60) | |
| No | 1 | |
PR, prevalence ratio.
The study addressed the relevant and universal issue of BF under three mostly innovative aspects: the holistic approach, the use of this approach in a very specific socio-environmental ecosystem and, finally, the systematization of concepts and indicators standardized by the WHO.20
By assessing the universe of children up to 36 months old living in a slum area in the Northeast region of Brazil, for the first time in the country, it was possible to describe and analyze the prevalence and typologies of BF in an ecosystem of marked socio-environmental vulnerability, now formally called subnormal urban cluster.18
Given the scarcity and limitation of other studies, the present study can be considered as baseline for a cohort project in the assessed community and a possible reference for subsequent epidemiological investigations in similar suburban areas, consolidating and improving PHC on new bases, with the comprehensive understanding of the health/disease process as an expression of human development.22
Shifting the comparative perspective to other evaluation instances, it is noteworthy that the prevalence of 60.2% of BF in the first hour of life is already well above the 44% global levels reported by UNICEF (2016),8 being very close to the data observed in Brazil (68%) and in the city of Recife (67%); similar findings were observed regarding EBF in children under 6 months in the Northeast region (37.0%), and Recife (38.3%),8 whereas in the Coelhos Community it was 46.3%. The high prevalence of EBF at 6 months (32%) was a surprising fact, considering that the II BF Prevalence Survey, carried out in Brazilian city capitals, found a prevalence of 9.3% for the country, 8.4% for the Northeast region, and 6.1% for the city of Recife.9
It is very likely that differences in results, as shown by BF median values in the Coelhos community in relation to data from Brazilian capital cities, can be attributed to the assumption that it would be questionable that the results of an urban cluster considered subnormal (or atypical) be comparatively referenced with national, regional and even state data, when they involve distinct populations, distinct times, distinct methods of collecting and analyzing well-differentiated data,10 and, especially, the history of health care, which is very characteristic in relation to BF.23 This is most likely to be the major focus of smaller or larger between studies. In this case, the carefully revalidated 182-day results observed in the present study appear to be robust and acceptable for the assessed population.
It is quite possible that the intensive participation of the FHS, through actions that have been well established in the community, such as the former Community Health Program Agents (PACS), later converted into the Family Health Program (FHP) comprising a 45-year history when the evaluation reported here was carried out, played a significant role in these results.
This is a pioneering experience in Brazil, implemented in the Coelhos Community with the support of UNICEF shortly after the International Conference of Alma Ata (1978) in Russia,23 with the proposal to universalize PHC as a strategy to expand coverage of basic health actions to all countries and territorial areas not assisted by the traditional model of public or private services.
Moreover, the Coelhos community is the beneficiary of the first Child-Friendly Hospital in Brazil, with an on-demand outpatient clinic for BF promotion, protection, and support, as well as care for early and late puerperal breast problems at the Human Milk Bank, which has been used as a model for other services in Brazil and Latin America.
It is clear that there is still a great deal to be achieved in relation to BF indicators in the assessed community, considering 80% of EBF in children under 6 months as a desirable and possible target.7
The analysis of isolated factors, and especially of combined factors in a complex event that can be associated to the main outcome of the study (EBF at 6 months) is obviously a complicated task, especially for quantitative evaluations, when often the causes can only be understood through a qualitative analysis.15,16 This is one clearly depicted limitation.
However, it is important to consider that, of the 22 assessed variables, nine were preliminarily admitted into the statistical screening (p<0.20) to be included in the multivariate analysis adjustment process. At this stage, which defines the construction of the final model, four factors remained in the “explanatory” panel as pros in determining the statistically validated hypotheses: maternal age>36 years, home visit in the first week of life by the health agents together with the nurse, child's male gender, and non-use of pacifiers.
Evidently, there is a basic truism in these analytical observations. It is very likely that older mothers have accumulated a more substantial prior experience, either because of previous pregnancies or because of their receptiveness to the formal contacts with health services where they were assisted during prenatal care, delivery, and puerperium. As for adolescents or young mothers, almost always with low or no parity, they face the demands of pregnancy with greater insecurity, including the willingness to breastfeed. The national24 and international25 literature has recorded this behavior, which is outstanding in the case of Brazil and many countries, due to the observation that the birth rate is concentrated in women under 25 years of age, many of them adolescents.26
The evidence that early weaning may vary according to the child's gender,9,14,15,17,27 considering the fact that the female gender is benefits more from EBF,9,14,15 may arise from the idea that, as boys are biologically “stronger”, they should receive stronger milk, “mistakenly perceived by some mothers as cow's milk”.15 The present study showed a prevalence of EBF for the male gender, which can be explained by the theory of Trivers-Willard27 as natural selection principles, of teleological character, enunciated in 1973.27 Thus, the unequal parental investment regarding daughters and sons would derive from maternal socioeconomic conditions and the reproductive potential of their offspring.
Contrary to Trivers-Willard's hypothesis that mothers with better social conditions invest more in their sons, while those in more adverse conditions would prioritize their daughters, and the evidence shown by Fujita et al. in 201216 in Kenya's agropastoral communities, it is possible that the preference of mothers living in slums for BF their sons is a more appropriate behavior in urban populations, which have very specific characteristics, not being useful for comparisons with other studies. Moreover, due to the homogeneity of the economic poverty situation in the assessed slum, it is not possible to establish very different socioeconomic contrasts, as in the study by Fujita et al.,16 having as reference the Trivers-Willard's hypothesis.27
The use of pacifiers, despite being a documented practice and considered discouraging to BF,17 was widely observed in the present study (47.4%) and consistently associated with weaning. However, a systematic review carried out in 2016 to evaluate the effect of the restricted use of pacifier versus free use on the practice of BF in two studies, with a total of 1302 healthy children born at term, found no significant effect on the rate of EBF at 3 months and 4 months of life.28 It is noteworthy that, unlike that systematic review, in the present study children who had never used pacifiers were compared with those who had.
Another systematic review with meta-analysis carried out in 2014 to investigate the association between pacifier use and interruption of EBF in the first six months of life, totaling 46 studies (two clinical trials, 20 longitudinal studies, and 24 cross-sectional studies), showed that pacifier use may be a significant risk factor for early termination of EBF.29 These results, which are still contradictory, indicate that the question demands further study.
As a limitation of the present study, the possible lack of power for some of the assessed associations is noteworthy. In turn, it is important to emphasize that it was a census survey, not a simple sample covering the age group most suitable for studies that require the retrieval of previous data on BF, due to the recall bias that increases with the increasing age of the children.
In conclusion, it was observed that the different indicators applied to the classification items of BF practices in the studied children may indicate the recent advancement process occurring in the country regarding the area of BF.4,30 Additionally, two analytical observations are considerably important, one of which was positive: the role of the home visit in the first week of life, a care action that constitutes a protection factor for EBF and, therefore, should be considered as systematic guidance.31 Another condition, due to its negative influence (the use of pacifiers) impairing the BF practice, represents a traditional practice that should be discouraged.11
FundingNational Post-Doctorate Program (PNPD) of Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silva VA, Caminha MF, Silva SL, Serva VM, Azevedo PT, Batista Filho M. Maternal breastfeeding: indicators and factors associated with exclusive breastfeeding in a subnormal urban cluster assisted by the Family Health Strategy. J Pediatr (Rio J). 2019;95:298–305.




