
To analyze the association between household smoking and the development of learning in elementary schoolchildren.
MethodsCross-sectional study with 785 students from the 2nd to the 5th year of elementary school. Students were evaluated by the School Literacy Screening Protocol to identify the presence of learning disabilities. Mothers/guardians were interviewed at home through a validated questionnaire. Descriptive and bivariate analysis, as well as multivariate Poisson regression, were performed.
ResultsIn the final model, the variables associated with learning difficulties were current smoking at the household in the presence of the child (PR=6.10, 95% CI: 4.56 to 8.16), maternal passive smoking during pregnancy (PR=1.46, 95% CI: 1.07 to 2.01), students attending the 2nd and 3rd years of Elementary School (PR=1.44, 95% CI: 1.10 to 1.90), and being children of mothers with only elementary level education (PR=1.36, 95% CI: 1.04 to 1.79).
ConclusionThe study demonstrated an association between passive exposure to tobacco smoke and learning difficulties at school.
Analisar a associação entre o tabagismo domiciliar e o desenvolvimento da aprendizagem em escolares do ensino fundamental.
MétodosEstudo transversal, com 785 escolares do 2° ao 5° ano do ensino fundamental. Os alunos foram avaliados por meio do Protocolo de Triagem de Letramento Escolar, visando identificar a presença de dificuldades de aprendizagem. As mães/responsáveis foram entrevistadas no domicílio por meio de questionário validado. Foram realizadas análises descritiva, bivariada e regressão múltipla de Poisson.
ResultadoNo modelo final, as variáveis associadas às dificuldades de aprendizagem foram tabagismo atual domiciliar na presença do filho (RP=6,10; IC 95% 4,56–8,16), tabagismo passivo materno durante a gestação (RP=1,46; IC 95% 1,07–2,01), alunos pertencerem ao 2° e 3° ano do ensino fundamental (RP=1,44; IC 95% 1,10–1,90) e serem filhos de mães com apenas o nível fundamental de escolaridade (RP=1,36; IC 95% 1,04–1,79).
Conclusãoo estudo evidenciou associação entre a exposição passiva ao tabaco e as dificuldades de aprendizagem nos escolares.
The development of reading and writing by the child results from the interaction between biological characteristics and multiple family sociocultural factors.1 One of the main negative influences in this process is the exposure of children to cigarette smoke, due to its interference with several physiological processes and cognitive functions related to learning.2–4 In Brazil and other countries with high prevalence of smoking,5 this exposure is a major public health problem.
Household tobacco smoke is the most common air pollutant inside homes; its concentration may vary depending on the number of smokers in the household and the number of cigarettes smoked by those individuals. Intense exposure to this type of air pollution can lead to intellectual disability and cognitive impairment in children, as well as result in other deleterious effects related to maternal and child health, such as miscarriage, low birth weight, and prematurity.6
Maternal smoking during pregnancy can lead to premature placental maturation and reduce its nutritional capacity, causing changes in fetal growth. Carbon monoxide and nicotine present in cigarette smoke are rapidly absorbed by the placenta, affecting the mental, intellectual, and behavioral development of these children, in addition to other complications described in literature.7–9
The mechanisms through which tobacco acts on cognitive function have yet to be fully understood. Exposure to tobacco smoke can lead to fetal hypoxia due to increased blood carbon monoxide concentrations, resulting in several neurotoxic effects on the child's neuropsychomotor development.10 Therefore, children born to mothers who smoke during pregnancy and who are constantly exposed to environmental tobacco smoke, especially in early childhood, are at increased risk of experiencing alterations in their intellectual capacities, mental disorders, and hearing loss,6 in addition to a greater probability of having learning difficulties.2
There is a growing interest in the search for understanding the multiple factors that affect growth and neuropsychomotor development of children, considering the high prevalence of learning disabilities at school age. It is also important to implement public policies to recognize the deleterious effects of concomitant passive and active smoking of adults and children, both in external environments and in family homes. Thus, the aim of this study was to analyze the association between household smoking and the learning development of schoolchildren attending elementary school.
MethodsA cross-sectional study was carried out with 785 students from seven municipal and state urban public schools in the municipality of Campo Verde. Campo Verde is located in the Southeast region of the state of Mato Grosso, and has an area of 4795km2, an altitude of 736m above sea level, and a population of 31,000 inhabitants; it has the highest agricultural GDP of Brazil due to the large production of soybeans, cotton, corn, sorghum, sunflower, and poultry.11
Sample selection was carried out by simple random sampling of students based on the data provided by the Municipal Education Secretariat of Campo Verde, which, in the year 2012, had 1732 students attending the first years of elementary school (2nd to 5th grades), distributed in seven schools. To calculate the sample size, the number of schools and the proportion of students enrolled at the different grades of elementary school were considered. A prevalence of 15% of smoking adults was estimated,12 95% confidence interval, statistical power of 80%, expected outcome frequency in the unexposed individuals of 9.0%, with a ratio of four unexposed to one exposed individual and a detectable prevalence ratio of 2.0. The final sample comprised 718 schoolchildren, plus 10% for expected losses (72), totaling 790 participants. As inclusion criteria, children who were regular students of these schools were selected. Students with mental, hearing, visual disabilities, and psychiatric disorders pre-identified by specialized health services of the municipal Brazilian Unified Health System (Sistema Único de Saúde [SUS]) and reported to the special education team of the Municipal Education Secretariat, were excluded from the study. There was a loss of five participants due to the refusal of the students’ parents/guardians to participate.
Data collection occurred in two stages: in the first, the students participated of the School Literacy Screening Protocol13 for the assessment of learning difficulties, applied by the main researcher in their own school. This protocol consists of ten questions about performing tasks such as pairing letters, words and numbers, serial letter identification, words and numbers, naming of letters and words, writing name and surname, writing letters and words, word dictation, reading words, reading sentences, and phrasal cloze test (five sentences were shown with a blank in each and a support chart, to be used to complete these sentences; the student completed them so that they made sense). The maximum score that a student could achieve was 30 points and the minimum, zero points. Subsequently, the students who had a performance above the score median were considered as having “normal learning status” and, up to the median (20.5), as “altered status” for learning development.
At the second stage, information was collected on the schoolchildren's households from every child's mother or guardian. These data were used to characterize the status of exposure to maternal smoking and the child's through the Fagerström14 questionnaire, adapted15 and validated16 for the Portuguese language. At this stage eight undergraduate students assisted, from the School of Education of Faculdade Cândido Rondon in Campo Verde, previously trained for this activity.
The information on the children's passive smoking and associated factors were obtained by applying a questionnaire divided into seven parts: the first and the second parts contained questions related to identification data of the child and mother. The third part contained questions related to gestational data of the student, such as: prenatal care, type of delivery, gestational age and weight at birth, and maternal consumption habits such as alcohol, tobacco, drugs, and medication. The fourth part was related to sociodemographic information, including ownership of assets, paternal education, family income, number of household members, and economic class according to the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisas [ABEP]).17 The fifth and the sixth part contained questions related to smoking: past or current smoking history of the mother, father, or other members of the household and tobacco use inside the household. The seventh and last part was related to factors associated with learning difficulties.
Data were double entered using the Epi-Info 7.0 software (Epi Info™, GA, USA) and by using the Data Compare application, which belongs to the same program; the typing errors were detected and corrected.
The bivariate analysis identified the gross associations through the chi-squared test for a prevalence ratio with 95% confidence interval using the Mantel–Haenszel method or Fisher's exact test, when indicated. Possible interactions and confounding factors were examined through stratified analysis, using as stratification variables those that the literature reports as important.
Poisson multiple regression analysis was performed in blocks (block 1 – sociodemographic variables of the students; block 2 – maternal sociodemographic variables; block 3 – gestational variables; block 4 – type of maternal smoking), including in each block all variables with a p-value <0.20 in the bivariate analysis through the step-by-step forward method, retaining in the final model the variables with significance level <0.05. The data were analyzed using the statistical software Epi-Info 7.0 (Epi Info™, GA, USA) and Stata version 13.0 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX, USA).
The project was approved by the Ethics Committee for Research in human subjects of Hospital Julio Müller, under No. 45671. All those involved in the research signed the informed consent, according to Resolution 196/96 of the National Ethics Committee on Research (Comissão Nacional de Ética em Pesquisa [CONEP]).
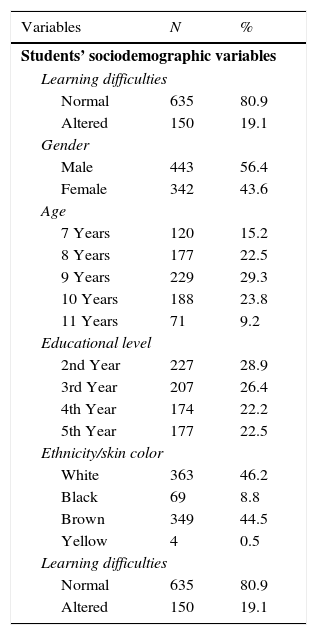
ResultsOf the 790 eligible students for the study, five participants were excluded due to the mother's refusal to participate or change of address during the data collection period, totaling 785 students, aged between 7 and 11 years (Table 1). The prevalence of learning difficulties detected by the literacy test was 19.1%. As for the sociodemographic characteristics of the students, 56.4% were males, 67.0% were younger than 9 years old, 55.3% attended the 3rd grade of elementary school, and white ethnicity was the most frequent (46.2%).
Distribution of schoolchildren according to sociodemographic characteristics, municipality of Campo Verde, MT, Brazil, 2012 (n=785).
| Variables | N | % |
|---|---|---|
| Students’ sociodemographic variables | ||
| Learning difficulties | ||
| Normal | 635 | 80.9 |
| Altered | 150 | 19.1 |
| Gender | ||
| Male | 443 | 56.4 |
| Female | 342 | 43.6 |
| Age | ||
| 7 Years | 120 | 15.2 |
| 8 Years | 177 | 22.5 |
| 9 Years | 229 | 29.3 |
| 10 Years | 188 | 23.8 |
| 11 Years | 71 | 9.2 |
| Educational level | ||
| 2nd Year | 227 | 28.9 |
| 3rd Year | 207 | 26.4 |
| 4th Year | 174 | 22.2 |
| 5th Year | 177 | 22.5 |
| Ethnicity/skin color | ||
| White | 363 | 46.2 |
| Black | 69 | 8.8 |
| Brown | 349 | 44.5 |
| Yellow | 4 | 0.5 |
| Learning difficulties | ||
| Normal | 635 | 80.9 |
| Altered | 150 | 19.1 |
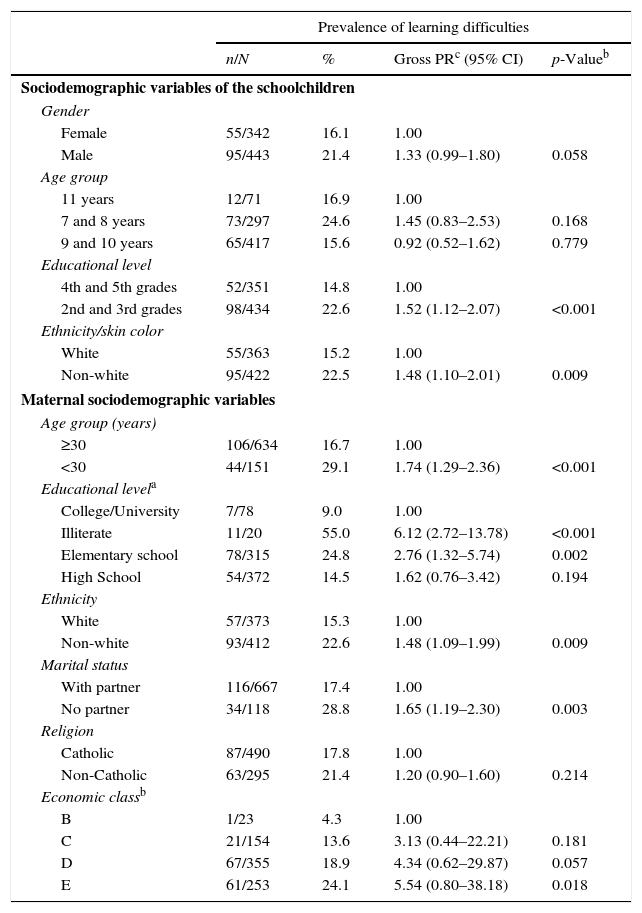
At the bivariate analysis, male students (PR=1.33, 95% CI: 0.99 to 1.80), attending the 2nd and 3rd grades of Elementary School (PR=1.52, 95% CI: 1.12 to 2.07) and non-whites (PR=1.48, 95% CI: 1.10 to 2.01) were statistically associated with learning difficulties. Regarding the maternal variables, children of mothers younger than 30 years of age (PR=1.74, 95% CI: 1.29 to 2.36), who were illiterate (PR=6.12, 95% CI: 2.72 to 13.78), or who had only elementary education (PR=2.76, 95% CI: 1.32 to 5.74) when compared to children of mothers that had a higher level of schooling, and who were non-white (PR=1.48, 95% CI: 1.09 to 1.99) were associated with learning difficulties. The children of mothers who lived without a partner and belonged to economic classes D (PR=4.34; 95%: CI 0.62 to 29.87) and E (PR=5.54, 95% CI: 0.80 to 38.18) were also associated with learning difficulties (PR=1.65, 95% CI: 1.19 to 2.30), when compared with children of mothers from Class B (Table 2).
Learning difficulties among elementary school students: prevalence ratio (PR) and confidence interval (95% CI) in relation to sociodemographic and gestational variables. Campo Verde, MT, Brazil, 2012 (n=785).
| Prevalence of learning difficulties | ||||
|---|---|---|---|---|
| n/N | % | Gross PRc (95% CI) | p-Valueb | |
| Sociodemographic variables of the schoolchildren | ||||
| Gender | ||||
| Female | 55/342 | 16.1 | 1.00 | |
| Male | 95/443 | 21.4 | 1.33 (0.99–1.80) | 0.058 |
| Age group | ||||
| 11 years | 12/71 | 16.9 | 1.00 | |
| 7 and 8 years | 73/297 | 24.6 | 1.45 (0.83–2.53) | 0.168 |
| 9 and 10 years | 65/417 | 15.6 | 0.92 (0.52–1.62) | 0.779 |
| Educational level | ||||
| 4th and 5th grades | 52/351 | 14.8 | 1.00 | |
| 2nd and 3rd grades | 98/434 | 22.6 | 1.52 (1.12–2.07) | <0.001 |
| Ethnicity/skin color | ||||
| White | 55/363 | 15.2 | 1.00 | |
| Non-white | 95/422 | 22.5 | 1.48 (1.10–2.01) | 0.009 |
| Maternal sociodemographic variables | ||||
| Age group (years) | ||||
| ≥30 | 106/634 | 16.7 | 1.00 | |
| <30 | 44/151 | 29.1 | 1.74 (1.29–2.36) | <0.001 |
| Educational levela | ||||
| College/University | 7/78 | 9.0 | 1.00 | |
| Illiterate | 11/20 | 55.0 | 6.12 (2.72–13.78) | <0.001 |
| Elementary school | 78/315 | 24.8 | 2.76 (1.32–5.74) | 0.002 |
| High School | 54/372 | 14.5 | 1.62 (0.76–3.42) | 0.194 |
| Ethnicity | ||||
| White | 57/373 | 15.3 | 1.00 | |
| Non-white | 93/412 | 22.6 | 1.48 (1.09–1.99) | 0.009 |
| Marital status | ||||
| With partner | 116/667 | 17.4 | 1.00 | |
| No partner | 34/118 | 28.8 | 1.65 (1.19–2.30) | 0.003 |
| Religion | ||||
| Catholic | 87/490 | 17.8 | 1.00 | |
| Non-Catholic | 63/295 | 21.4 | 1.20 (0.90–1.60) | 0.214 |
| Economic classb | ||||
| B | 1/23 | 4.3 | 1.00 | |
| C | 21/154 | 13.6 | 3.13 (0.44–22.21) | 0.181 |
| D | 67/355 | 18.9 | 4.34 (0.62–29.87) | 0.057 |
| E | 61/253 | 24.1 | 5.54 (0.80–38.18) | 0.018 |
| Variables | Prevalence of learning difficulties | |||
|---|---|---|---|---|
| n/N | % | Gross PR (95%CI) | p-Value | |
| Prenatal care | ||||
| Yes | 148/779 | 19.0 | 1.00 | |
| No | 2/6 | 33.3 | 1.75 (0.56–5.49) | 0.322 |
| Number of consultations | ||||
| ≥6 | 133/748 | 17.8 | 1.00 | |
| <6 | 17/37 | 45.9 | 2.58 (1.76–3.78) | <0.001 |
| Type of delivery | ||||
| Vaginal | 91/475 | 19.2 | 1.00 | |
| Cesarean section | 59/309 | 19.1 | 0.99 (0.74–1.34) | 0.982 |
| Low birth weight | ||||
| No | 144/769 | 18.7 | 1.00 | |
| Yes | 6/16 | 37.5 | 2.00 (1.04–3.83) | 0.059 |
| Preterm birth | ||||
| No | 138/716 | 19.3 | 1.00 | |
| Yes | 12/69 | 17.4 | 0.90 (0.52–1.54) | 0.704 |
| Alcohol consumption | ||||
| No | 129/735 | 17.6 | 1.00 | |
| Yes | 21/50 | 42.0 | 2.39 (1.67–3.43) | <0.001 |
| Drug use | ||||
| No | 148/779 | 19.0 | 1.00 | |
| Yes | 2/5 | 40.0 | 2.10 (0.71–6.22) | 0.234 |
| Medication use | ||||
| No | 140/749 | 18.7 | 1.00 | |
| Yes | 10/36 | 27.8 | 1.48 (0.85–2.57) | 0.176 |
| Gestational diseases | ||||
| No | 138/754 | 18.3 | 1.00 | |
| Yes | 12/31 | 38.7 | 2.11 (1.32–3.38) | 0.004 |
Regarding the gestational variables (Table 3), the learning difficulties showed to be statistically associated with children of pregnancies with fewer than six prenatal consultations (PR=2.58, 95% CI: 1.76 to 3.78), those born with low birth weight (PR=2.00, 95% CI: 1.04 to 3.83), those born to mothers who consumed alcohol during the pregnancy (PR=2.39, 95% CI: 1.67 to 3.43), and those who had some gestational disease (PR=2.11, 95% CI: 1.32 to 3.38).
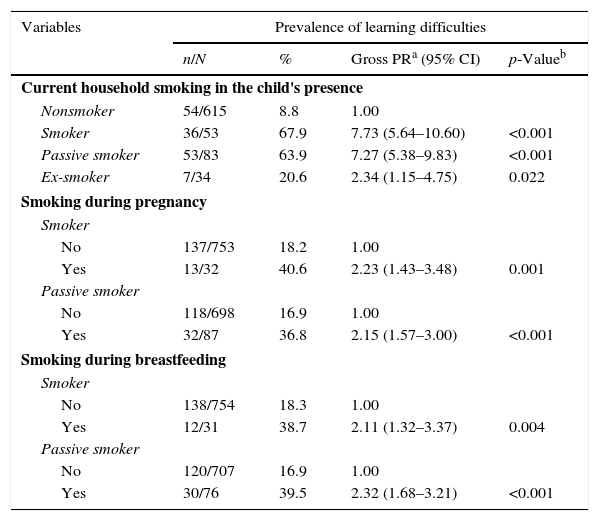
Learning difficulties among elementary school students: prevalence ratio (PR) and confidence interval (95%) in relation to maternal smoking. Campo Verde, MT, Brazil, 2012 (n=785).
| Variables | Prevalence of learning difficulties | |||
|---|---|---|---|---|
| n/N | % | Gross PRa (95% CI) | p-Valueb | |
| Current household smoking in the child's presence | ||||
| Nonsmoker | 54/615 | 8.8 | 1.00 | |
| Smoker | 36/53 | 67.9 | 7.73 (5.64–10.60) | <0.001 |
| Passive smoker | 53/83 | 63.9 | 7.27 (5.38–9.83) | <0.001 |
| Ex-smoker | 7/34 | 20.6 | 2.34 (1.15–4.75) | 0.022 |
| Smoking during pregnancy | ||||
| Smoker | ||||
| No | 137/753 | 18.2 | 1.00 | |
| Yes | 13/32 | 40.6 | 2.23 (1.43–3.48) | 0.001 |
| Passive smoker | ||||
| No | 118/698 | 16.9 | 1.00 | |
| Yes | 32/87 | 36.8 | 2.15 (1.57–3.00) | <0.001 |
| Smoking during breastfeeding | ||||
| Smoker | ||||
| No | 138/754 | 18.3 | 1.00 | |
| Yes | 12/31 | 38.7 | 2.11 (1.32–3.37) | 0.004 |
| Passive smoker | ||||
| No | 120/707 | 16.9 | 1.00 | |
| Yes | 30/76 | 39.5 | 2.32 (1.68–3.21) | <0.001 |
As for current household smoking in the child's presence, it was observed that children of mothers that were ex-smokers (PR=2.34, 95% CI: 1.15 to 4.75), passive smokers (PR=7.27; 95% CI: 5.38 to 9.83), or current smokers (OR=7.73, 95% CI: 5.64 to 10.60) were associated with learning difficulties. In relation to maternal smoking during pregnancy, children of mothers who were smokers (PR=2.23, 95% CI: 1.43 to 3.48) and passive smokers (PR=2.15, 95% CI: 1.57 to 3.00) had a higher incidence of learning difficulties. Regarding smoking while breastfeeding, children of mothers who were smokers (PR=2.11, 95% CI: 1.32 to 3.37) or passive smokers (PR=2.32, 95% CI: 1.68 to 3.21) also had children associated with learning difficulties (Table 4).
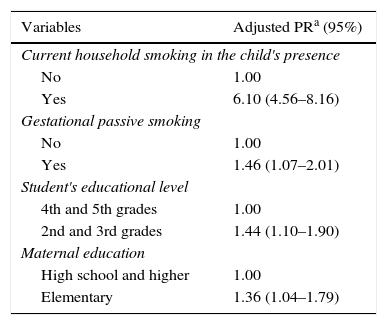
Multiple Poisson regression for maternal smoking and learning difficulties of schoolchildren from elementary schools in Campo Verde, MT, Brazil, 2012 (n=785).
| Variables | Adjusted PRa (95%) |
|---|---|
| Current household smoking in the child's presence | |
| No | 1.00 |
| Yes | 6.10 (4.56–8.16) |
| Gestational passive smoking | |
| No | 1.00 |
| Yes | 1.46 (1.07–2.01) |
| Student's educational level | |
| 4th and 5th grades | 1.00 |
| 2nd and 3rd grades | 1.44 (1.10–1.90) |
| Maternal education | |
| High school and higher | 1.00 |
| Elementary | 1.36 (1.04–1.79) |
Table 4 shows the results of the final Poisson model. Current smoking in the household in the child's presence (PR=6.10, CI: 4.56 to 8.16), maternal passive smoking during pregnancy (PR=1.46, CI: 1.07 to 2.01), students attending the 2nd and 3rd years of Elementary School (PR=1.44, CI: 1.10 to 1.90), and children of mothers with only elementary schooling (PR=1.36; CI: 1.04 to 1.79), remained associated with learning difficulties.
DiscussionThe results of this study confirmed the association between learning difficulties in students exposed to both active and passive maternal smoking. The fact of having parents who smoke leads to more occurrences of learning difficulties, behavioral problems, and language difficulties in children.2–4,16 Kabir et al.,3 in a national child health survey in the United States, confirmed a higher prevalence of learning difficulties from neurobehavioral disorders associated with passive smoking. Linnet et al.,8 in a systematic review article, evaluated 24 studies on tobacco use during pregnancy and its effect on attention deficit disorder and associated diseases. In addition to the association between maternal smoking and attention deficit, those authors found associations with hyperactivity and learning disorders in the assessed children. It is noteworthy that the entire tobacco exposure period, both the mother's prenatal and the newborn's postnatal, may be responsible for the deleterious effects on the child's learning development. Tobacco smoke inhalation causes a decrease in oxygen and nutrient flow to the fetus, especially damaging the normal activities of the central and peripheral nervous system.8
There was a higher prevalence of students with learning difficulties in the early grades of elementary school (2nd and 3rd grades). In this sense, Sousa and Maluf18 stated that the automation of the reading and writing learning process occurs continuously, suggesting that in the early years of study, these difficulties are greater and, with the passing of the remaining school years, a continued improvement in the behavioral and cognitive aspects of learning occurs.
An association was found between low level of maternal schooling and higher prevalence of children with learning difficulties. Similarly to the present study, Jackson,19 in a longitudinal study that followed black mothers from families at social risk and assessed the characteristics of their children's behavior and cognitive development, found that children of mothers in low employment situation showed a higher incidence of cognitive problem development, always associated to the lower levels of education of these mothers.
An association between mothers of low socioeconomic status and the occurrence of learning difficulties was also identified. Consistent with other studies, schoolchildren of single mothers were more often associated with learning difficulties.19,20 Sganzerla et al.21 emphasized the role of the family and the importance of the mother's partner's presence for emotional and financial stability and, consequently, the children's best intellectual development.
Regarding the variables related to pregnancy, children of mothers who had fewer than six prenatal consultations were associated with higher rates of learning difficulties. The Ministry of Health recommends having at least seven consultations during pregnancy.22 Among the positive effects related to the monitoring of pregnant women are the decrease in child mortality and better prognosis during childbirth and infancy of the newborn, including better psychomotor development of the newborn.23
The occurrence of diseases during pregnancy was also associated with higher prevalence of learning difficulties. Several gestational diseases, such as rubella and toxoplasmosis, among others, are associated with higher incidence of stillbirths, intrauterine growth retardation, and sequelae in the intellectual development of the affected children,24 suggesting that these same situations might have occurred in this study.
Alcohol use during pregnancy was associated with learning difficulties. Alcohol intake is often associated with deleterious effects on the fetus’ neurodevelopment, ranging from cognitive deficit and learning difficulties to severe mental impairment.25 Social drinking is often associated with the habit of smoking26; this interaction has led to the inclusion of maternal alcohol consumption to improve the data analysis regression model adjustment.
It is necessary to be cautious when interpreting the association between non-white ethnicity and learning disability, as observed in this study. Also, the occurrence of a probable confounding factor between social class and ethnicity (skin color) cannot be excluded.27 Data from IBGE11 indicate that the majority of the brown and black-skinned population belong to the lower socioeconomic strata, with greater difficulty in school access, which could result in a spurious association between ethnicity and learning disability. Another likely confounding factor that may have occurred was that between low prenatal care adherence and low birth weight.28
It is important to remember that, in cross-sectional studies, the exposure factors and the outcome are simultaneously determined, and caution is recommended when interpreting the causal associations. A possible recall bias by the mothers when answering the questionnaire with recall data on the pregnancy and previous habits may also have occurred. In these cases, longitudinal studies of exposure monitoring are more appropriate to indicate the associations between the exposure variable (smoking) and the response variable (learning disability).29
Regarding the tool used to measure school literacy, it was carefully assessed by professionals from a reference educational and research institution, suggesting that the results were reproducible and considered consistent for its use as a school performance assessment method. Nevertheless, a limitation of this tool is the fact that has not been not validated and published in an important journal in this field of knowledge, as well as the limitations related to biases that may have occurred with the use of this tool. Finally, the strong association found between current household smoking and school learning difficulties in the final model may have eliminated the statistical significance of the associations with other types of smoking, even though these are important for the occurrence of learning difficulties.
The results of this study indicated that exposure to passive smoking was associated with higher incidence of learning difficulties in the assessed population. It is necessary to prohibit tobacco use in all public spaces and conduct health educational campaigns regarding the harmful effects of passive smoking on the health of sensitive populations, especially schoolchildren.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Jorge JG, Botelho C, Silva AM, Moi GP. Influence of passive smoking on learning in elementary school. J Pediatr (Rio J). 2016;92:260–7.





