

To evaluate factors associated with low consumption of fruits and vegetables among preschoolers from families treated at basic health centers in Porto Alegre, RS, Brazil.
MethodsThis was a cohort study nested in a randomized field trial. Data collection was performed through structured questionnaires to obtain demographic and dietary data, combined with two 24-hour recalls in the age groups 12–16 months and again at 2–3 years of age. Data on the consumption of one daily serving of fruits (80g) and vegetables (60g) were evaluated, as well as consumption of non-recommended foods such as candy, chocolate, and soft drinks. Statistical analyses were performed using Poisson regression with robust estimation.
ResultsA total of 388 children aged 2-3 years were evaluated; of these, 58% and 87.4% did not consume one daily serving of fruits and vegetables, respectively. The following factors were negatively associated with fruit consumption: family income higher than four minimum wages, (p=0.024), lower paternal educational level (p=0.03), and lower fruit consumption at 12–16 months (p=0.002). Factors negatively associated with the consumption of vegetables were low paternal educational level (p=0.033) and consumption of high-sugar content beverages at 12–16 months (p=0.014).
ConclusionThis study demonstrated a high prevalence of children who consumed less than one daily serving of fruit and vegetables; early feeding practices, parental education, and family income were associated with this process.
Avaliar os fatores associados ao baixo consumo de frutas e verduras entre pré-escolares de famílias usuárias da rede básica de saúde de Porto Alegre, RS, Brasil.
MétodosEstudo de coorte aninhado a ensaio de campo randomizado. A coleta de dados foi feita por meio de questionários estruturados para obtenção de dados dietéticos e sociodemográficos, além de dois recordatórios de 24 horas nas faixas etárias de 12–16 meses e novamente aos 2-3 anos de idade. Foram avaliados os dados de consumo de uma porção diária de frutas (80g) e verduras (60g), além de consumo de alimentos não recomendados, como balas, chocolates e refrigerantes. As análises estatísticas foram feitas por regressão de Poisson com estimativa robusta.
ResultadosForam avaliadas 388 crianças de 2-3 anos, destas 58% e 87,4% não consumiram uma porção de frutas e verduras, respectivamente. Os fatores que se mostraram negativamente associados ao consumo de frutas foram: renda familiar superior a 4 salários mínimos, (p=0,024), menor escolaridade paterna (p=0,03) e menor consumo de frutas aos 12–16 meses (p=0,002). Os fatores negativamente associados à ingestão de verduras foram a menor escolaridade paterna (p=0,033) e consumo de refrigerante aos 12–16 meses (p=0.014).
ConclusãoOs resultados deste estudo mostraram alta prevalência de crianças que consumiram menos de uma porção de frutas e verduras ao dia e sugerem que práticas alimentares precoces, escolaridade paterna e renda estão associadas a esse processo.
Feeding habits in the early phase of life plays a fundamental role in children's growth and development;1 an appropriate introduction of solid foods is extremely important, as it can affect the future acceptance of foods.2 Among the policies on food and nutrition, encouraging the consumption of fruits and vegetables stands out among the guidelines to promote healthy eating habits,3,4 since an insufficient consumption of these groups was considered one of the main factors responsible for the global burden of diseases worldwide.5
Preschoolers are characterized by having higher micronutrient requirements when compared to their energy needs.6 This aspect, combined with the evidence that their diets contain high levels of saturated fat and sugar and are low in dietary fiber,6,7 makes this age group vulnerable to the development of obesity and micronutrient deficiency.6 Furthermore, it has been demonstrated that children prefer foods with higher energy density, mainly by the positive physiological consequences that they provide in relation to satiety and energy input,8 which may affect the consumption of vegetables and fruits.
Given the aforementioned evidence that the quality of food consumed by children is essential for health promotion and prevention of chronic diseases, this study aimed to evaluate the consumption of fruits and vegetables among preschoolers of low socioeconomic status and the maternal and family factors involved in this process.
MethodThis was a cohort study nested in a randomized field trial, performed between April of 2008 and May of 2012, with mothers and children followed from the ages of 6 months to 2-3 years. The recruitment phase occurred during the third trimester of pregnancy at health centers in the eight district areas of the city of Porto Alegre, state of Rio Grande do Sul, Brazil. During all study phases, the data collection team consisted of approximately 20 members (nutritionists and nutrition students) who were previously trained. The teams were divided according to the district region, and the collection was always performed by at least two team members.
The sample size considered the objective of the randomized field trial, in which an intervention performed with primary health care professionals would increase breastfeeding rates. The intervention consisted in an update of the “Ten steps to healthy eating for children younger than two years”3 guide for all professionals working in the selected health centers, in addition to providing educational materials based on the food guide, to be delivered to all mothers undergoing prenatal and child care. A power of 90%, confidence level of 95%, and a cluster correlation coefficient of 1.5 were considered for sample size calculation, which determined the inclusion of 300 mother-infant pairs in each group. Considering a prediction of loss of 20%, the recruitment of 720 individuals was estimated in order to reach the desired sample size.
Pregnant women were identified, invited to participate in the study, and informed about the procedures. After signing the informed consent, they answered the questionnaire, reporting data on age, educational level (years of schooling), employment (paid or unpaid), parity, marital status, family income (in Brazilian minimum wages, equivalent to R$ 477.40 in 2008), estimated date of birth, address, and telephone contact. Pregnant women with human immunodeficiency virus (HIV) infection were excluded from the study, since breastfeeding is contraindicated in this situation.
Subsequent phases of data collection were performed through home visits to the children when aged between 6 and 9 months, 12 and 16 months, and 2 to 3 years. Structured questionnaires and two 24-hour recalls were applied at each stage with the mothers or primary caregiver. The standardized 24-hour recalls were conducted for any weekday or weekend, and were not performed on consecutive days for the same child. Nutrient calculations were performed using the Dietwin Professional® software (Porto Alegre, Brazil), which is mainly based on the Brazilian Food Composition Table9 and used the average of two days.
The socio-demographic data were obtained at recruitment and were not repeated at the other phases.
Data collection: 6–9 monthsData related to exclusive breastfeeding were obtained.
Data collection: 12–16 monthsThe consumption of fruits and vegetables in the age group of 12 to 16 months was assessed through a specific questionnaire, which contained questions regarding the consumption of fruits and vegetables in the previous week.
The frequency of fruits and vegetables consumption at this age group was calculated based on the answers of the mothers or primary caregivers to the questions: “How often in the last week did your child consumed fruit?” and “How often in the last week did your child consume vegetables?”.
The energy percentage from non-recommended foods was calculated from the 24-hour recall. According to the Brazilian Ministry of Health,3 the following foods are not recommended for consumption by children under 2 years of age: candies, lollipops, chocolates, cookies, jello, petit suisse cheese, chocolate milk, sausages, snacks, soft drinks, artificial juices, and foods with added sugar.
While they answered the questionnaire, mothers also reported whether their children had consumed the abovementioned foods in the previous month. This information was used to classify the children according to the consumption of non-recommend foods into two groups: those who had consumed fewer than four and those who had consumed four types or more. The consumption of soft drinks and artificial juices was not considered in this group, as this information led to the creation of an additional group related to the consumption of sugary drinks.
Data collection: 2–3 yearsAn anthropometric assessment of the mother, including weight and height measurements to calculate body mass index (BMI), was performed. Maternal nutritional status was considered adequate when BMI < 25kg/m2, and overweight when ≥ 25kg/m2, according to the classification of the World Health Organization.5
Dietary variables related to consumption of fruits and vegetables at this age group were calculated using data from 24-hour recalls. The amount (in grams) of fruits and vegetables consumed was verified, and it was then investigated whether at least a portion of each food category had been consumed. A portion was defined as 80g for fruits and 60g for vegetables.3 The recommendations for the consumption of fruits and vegetables consist in three daily servings of each food group.3 To calculate the fruit intake, the consumption of natural fruit juices was not considered; the consumption of vegetables considered the intake of legumes, green-leaf vegetables, and solid soup contents. Potatoes were not considered in the group of vegetables, as they are traditionally allocated in the group of carbohydrate-rich foods, in accordance with Brazilian food guides.3,4
Statistical analysisThe data were double entered in SPSS, version 16.0 (Chicago, United States) and validated using Epi-Info®, version 6.4 (Atlanta, United States). Statistical analyses were performed in SPSS 16.0 software. Frequency analyses were performed to describe categorical variables with means and standard deviation for continuous variables. Continuous variables were tested for normality of distribution using the Kolmogorov-Smirnov test; when the distribution was not normal, they were presented as median and interquartile range.
The effect of the association between variables and outcome (consumption or non-consumption of at least a daily portion of each food category) was assessed by bivariate analysis using Poisson regression with robust estimation for variance adjustment. Variables that showed an association with lower level of statistical significance or equal to 20% (p ≤ 0.20) were included in the multivariate analyses. The magnitude of association between the investigated factors and feeding practices was estimated using prevalence ratios and confidence intervals (95% CI) in robust Poisson regression bivariate and multivariate analyses.
The study was approved by the Ethics Committee in Research of the Universidade Federal de Ciências da Saúde de Porto Alegre, and approved by the Porto Alegre City Hall Ethics Committee. Children with unfavorable clinical situations were referred to health services.
ResultsFig. 1 presents the flowchart of data collection, detailing the losses, refusals, and exclusions that occurred in each phase. It is noteworthy that 149 families (20.8%) were not located for follow-up, considering all phases of data collection. In addition, 87 children (12%) needed to be excluded from analysis because they did not have 24-hour recalls at 12-16 months and/or 2-3 years.

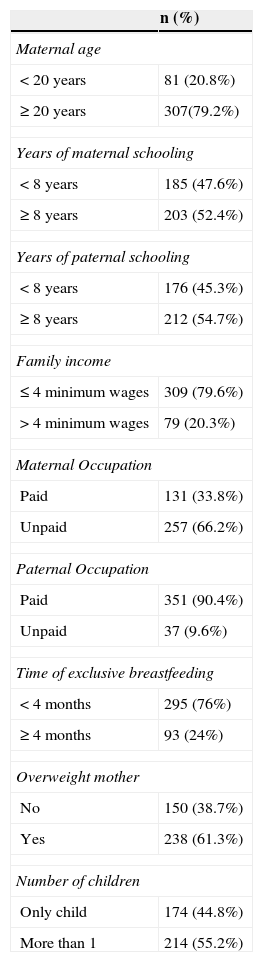
Among the children studied, the distribution between genders occurred homogeneously: 51.8% (n=201) were male. The characterization of the sample regarding the maternal and family data is described in Table 1.
Sample description.
| n (%) | |
|---|---|
| Maternal age | |
| < 20 years | 81 (20.8%) |
| ≥ 20 years | 307(79.2%) |
| Years of maternal schooling | |
| < 8 years | 185 (47.6%) |
| ≥ 8 years | 203 (52.4%) |
| Years of paternal schooling | |
| < 8 years | 176 (45.3%) |
| ≥ 8 years | 212 (54.7%) |
| Family income | |
| ≤ 4 minimum wages | 309 (79.6%) |
| > 4 minimum wages | 79 (20.3%) |
| Maternal Occupation | |
| Paid | 131 (33.8%) |
| Unpaid | 257 (66.2%) |
| Paternal Occupation | |
| Paid | 351 (90.4%) |
| Unpaid | 37 (9.6%) |
| Time of exclusive breastfeeding | |
| < 4 months | 295 (76%) |
| ≥ 4 months | 93 (24%) |
| Overweight mother | |
| No | 150 (38.7%) |
| Yes | 238 (61.3%) |
| Number of children | |
| Only child | 174 (44.8%) |
| More than 1 | 214 (55.2%) |
The prevalence of children aged 2-3 years who did not consume one serving of fruit or one serving of vegetables, considering the mean consumption obtained by two 24-hour recalls, was 58.0% (n=225) and 87.4% (n=340), respectively. The median intake of fruits and vegetables a day among children was 55g (0-130g) and 5g (0-30g), respectively. When assessing how many children consumed the recommended three servings of fruits and vegetables in at least one of the dietary surveys, it was observed that only 35 children (9%) achieved this recommendation for fruit and only one (0.2%) for vegetables.
Mothers who reported offering fruits and vegetables daily to their children when responding the 12-16 month questionnaire accounted for 50.4% and 42.4% of the sample, respectively.
The energy consumption of non-recommended foods at 12-16 months was on average 13.61% of total energy intake; for 9.2% of the children, these foods accounted for over 30% of energy consumption. Mothers who reported having offered soft drinks or artificial juices and at least three different types of non-recommended foods during the month before the 12-16 month data collection accounted for 83.3% and 68.3% of the sample, respectively.
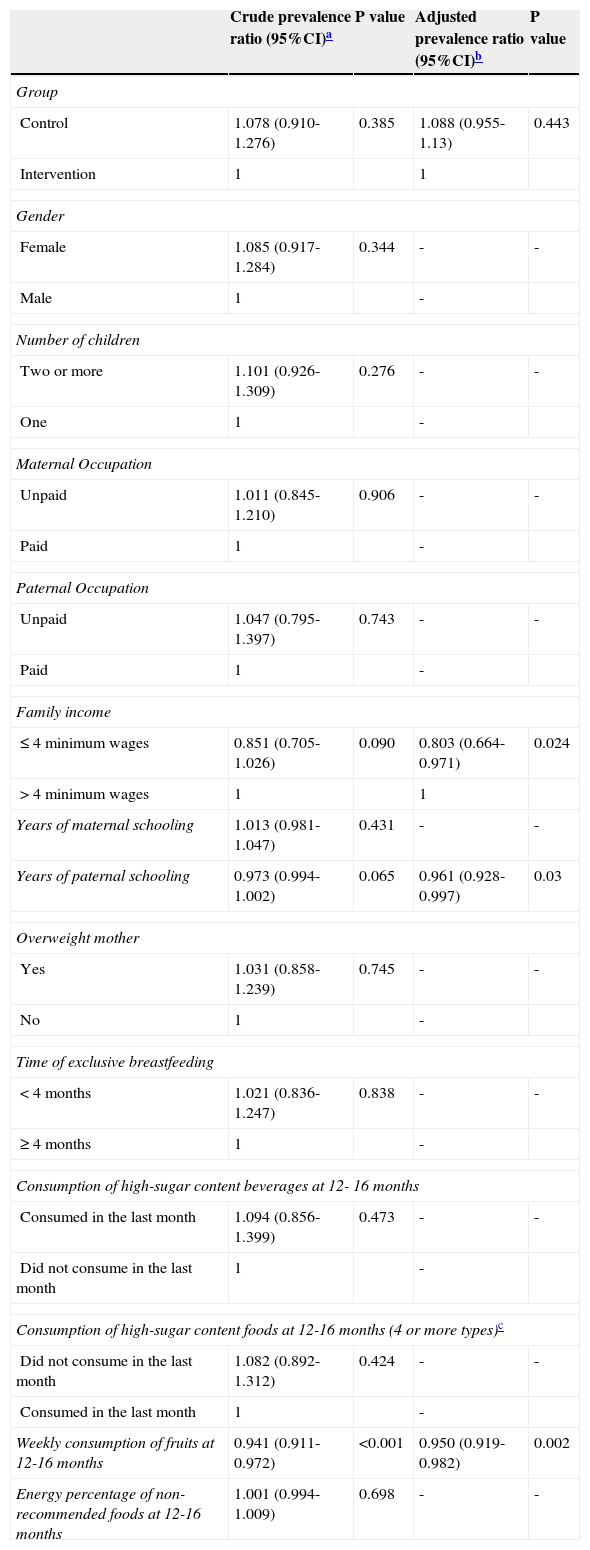
Table 2 shows the variables associated with the consumption of fruit at 2-3 years. There was no significant association with gender, number of children, maternal and paternal occupation, duration of exclusive breastfeeding, nutritional status, and maternal education. Among the dietary variables, the early consumption of sugary foods and drinks, as well as the percentage of energy coming from non-recommended foods consumed at 12-16 months was not associated with outcome.
Factors associated to low consumption of fruits among children aged 2–3 years.
| Crude prevalence ratio (95%CI)a | P value | Adjusted prevalence ratio (95%CI)b | P value | |
|---|---|---|---|---|
| Group | ||||
| Control | 1.078 (0.910-1.276) | 0.385 | 1.088 (0.955-1.13) | 0.443 |
| Intervention | 1 | 1 | ||
| Gender | ||||
| Female | 1.085 (0.917-1.284) | 0.344 | - | - |
| Male | 1 | - | ||
| Number of children | ||||
| Two or more | 1.101 (0.926-1.309) | 0.276 | - | - |
| One | 1 | - | ||
| Maternal Occupation | ||||
| Unpaid | 1.011 (0.845-1.210) | 0.906 | - | - |
| Paid | 1 | - | ||
| Paternal Occupation | ||||
| Unpaid | 1.047 (0.795-1.397) | 0.743 | - | - |
| Paid | 1 | - | ||
| Family income | ||||
| ≤4 minimum wages | 0.851 (0.705-1.026) | 0.090 | 0.803 (0.664-0.971) | 0.024 |
| >4 minimum wages | 1 | 1 | ||
| Years of maternal schooling | 1.013 (0.981-1.047) | 0.431 | - | - |
| Years of paternal schooling | 0.973 (0.994-1.002) | 0.065 | 0.961 (0.928-0.997) | 0.03 |
| Overweight mother | ||||
| Yes | 1.031 (0.858-1.239) | 0.745 | - | - |
| No | 1 | - | ||
| Time of exclusive breastfeeding | ||||
| <4 months | 1.021 (0.836-1.247) | 0.838 | - | - |
| ≥4 months | 1 | - | ||
| Consumption of high-sugar content beverages at 12- 16 months | ||||
| Consumed in the last month | 1.094 (0.856-1.399) | 0.473 | - | - |
| Did not consume in the last month | 1 | - | ||
| Consumption of high-sugar content foods at 12-16 months (4 or more types)c | ||||
| Did not consume in the last month | 1.082 (0.892-1.312) | 0.424 | - | - |
| Consumed in the last month | 1 | - | ||
| Weekly consumption of fruits at 12-16 months | 0.941 (0.911-0.972) | <0.001 | 0.950 (0.919-0.982) | 0.002 |
| Energy percentage of non-recommended foods at 12-16 months | 1.001 (0.994-1.009) | 0.698 | - | - |
CI, confidence interval.
Regarding income, children whose families had incomes higher than four minimum wages showed a 19% higher probability of not consuming one serving of fruit a day. A higher level of paternal education was associated with the consumption of fruits, and each additional year of study influenced by approximately 4% the probability of the child to consume one portion of fruit. Moreover, the weekly frequency of consumption of fruits at 12 months showed a positive association with their consumption at 2-3 years, with each day that the mother offered fruits to her child leading to a 5% increase in the probability of the child consuming them at the preschool years.
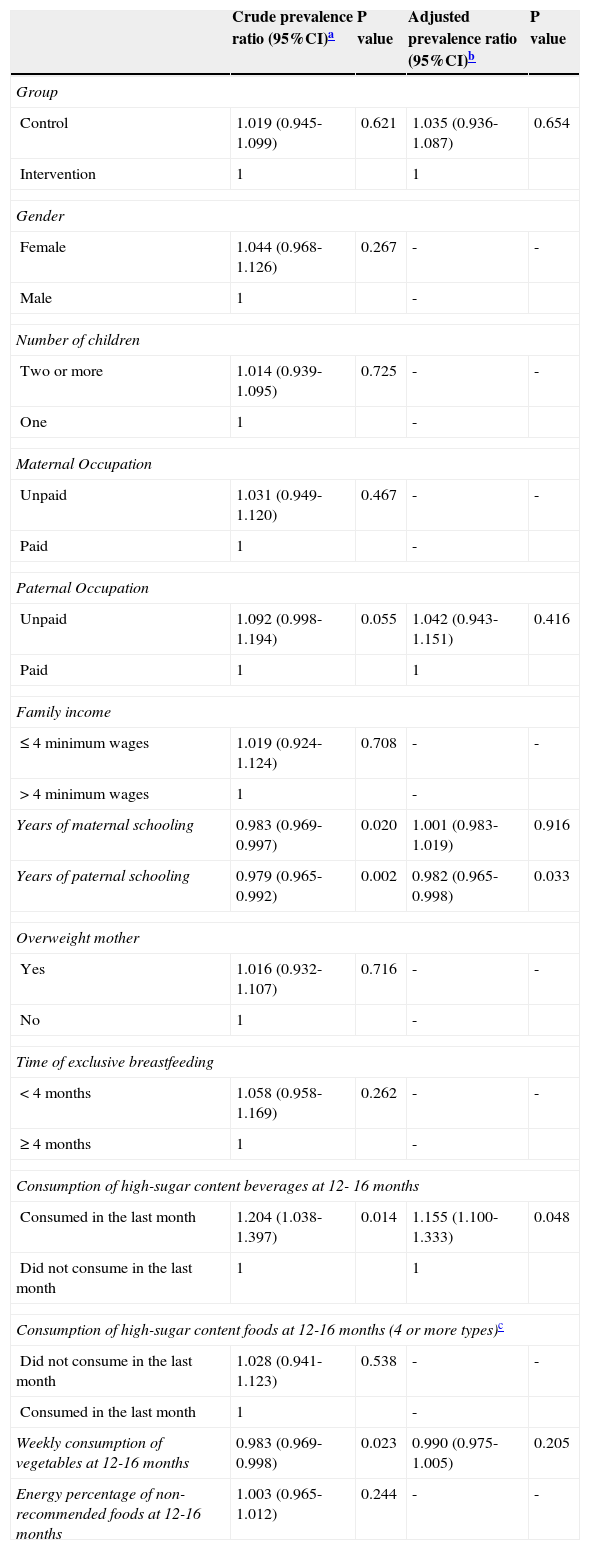
Table 3 describes the variables associated with the consumption of vegetables at 2-3 years. Each year of paternal education resulted in an increase of almost 2% in the probability of consuming at least one daily serving of vegetables; consumption of sugary drinks at 12-16 months increased the probability of the child not consuming one portion of vegetables by more than 15%.
Factors associated with low consumption of vegetables among children aged 2-3 years.
| Crude prevalence ratio (95%CI)a | P value | Adjusted prevalence ratio (95%CI)b | P value | |
|---|---|---|---|---|
| Group | ||||
| Control | 1.019 (0.945-1.099) | 0.621 | 1.035 (0.936-1.087) | 0.654 |
| Intervention | 1 | 1 | ||
| Gender | ||||
| Female | 1.044 (0.968-1.126) | 0.267 | - | - |
| Male | 1 | - | ||
| Number of children | ||||
| Two or more | 1.014 (0.939-1.095) | 0.725 | - | - |
| One | 1 | - | ||
| Maternal Occupation | ||||
| Unpaid | 1.031 (0.949-1.120) | 0.467 | - | - |
| Paid | 1 | - | ||
| Paternal Occupation | ||||
| Unpaid | 1.092 (0.998-1.194) | 0.055 | 1.042 (0.943-1.151) | 0.416 |
| Paid | 1 | 1 | ||
| Family income | ||||
| ≤4 minimum wages | 1.019 (0.924-1.124) | 0.708 | - | - |
| >4 minimum wages | 1 | - | ||
| Years of maternal schooling | 0.983 (0.969-0.997) | 0.020 | 1.001 (0.983-1.019) | 0.916 |
| Years of paternal schooling | 0.979 (0.965-0.992) | 0.002 | 0.982 (0.965-0.998) | 0.033 |
| Overweight mother | ||||
| Yes | 1.016 (0.932-1.107) | 0.716 | - | - |
| No | 1 | - | ||
| Time of exclusive breastfeeding | ||||
| <4 months | 1.058 (0.958-1.169) | 0.262 | - | - |
| ≥4 months | 1 | - | ||
| Consumption of high-sugar content beverages at 12- 16 months | ||||
| Consumed in the last month | 1.204 (1.038-1.397) | 0.014 | 1.155 (1.100-1.333) | 0.048 |
| Did not consume in the last month | 1 | 1 | ||
| Consumption of high-sugar content foods at 12-16 months (4 or more types)c | ||||
| Did not consume in the last month | 1.028 (0.941-1.123) | 0.538 | - | - |
| Consumed in the last month | 1 | - | ||
| Weekly consumption of vegetables at 12-16 months | 0.983 (0.969-0.998) | 0.023 | 0.990 (0.975-1.005) | 0.205 |
| Energy percentage of non-recommended foods at 12-16 months | 1.003 (0.965-1.012) | 0.244 | - | - |
CI, confidence interval.
This study demonstrated that 87% of the children consumed less than one serving of vegetables, and that 58% did not consume one serving of fruit a day. Similar data were observed in a Brazilian study of children between 6 and 59 months of age, in which the low prevalence of consumption of fruits and vegetables was observed. The authors observed that less than 50% of the children consumed fruit daily and only 12% consumed leafy vegetables.10 There is evidence that dietary patterns established in the early years will remain throughout life,11,12 because early exposure to certain foods or flavors has a heavy influence on their acceptance in the short and long-term.13
The findings of this study corroborate this evidence, with the observation that fruit consumption at 12 months of age was associated to its consumption at 2-3 years. It is emphasized that the recommendations for fruits and vegetables are three daily servings, that is, 240g and 180g, respectively. The percentage of children who reached these recommendations was not sufficient to analyze this proposal in the present study.
Another finding was the association between consumption of soft drinks and other sugary drinks in the first year of life and lower consumption of vegetables at 2-3 years. The consumption of these beverages, especially soft drinks, has increased significantly among children,14 and some studies have associated the consumption of sugar-sweetened beverages with weight gain and adiposity15 and other comorbidities, such as increased blood glucose levels in children and adults.15,16
Beauchamp and Moran17 demonstrated that children have the innate sweet taste preference, and that early intake of sugary liquids can further encourage this preference. Additionally, Skinner11 observed that while sweet foods are among the favorites of children, the least-appreciated foods are vegetables. Thus, stimulation of the innate preference for sweets, offering soft drinks and artificial juices, added to the low consumption of vegetables early in life, which may negatively affect the development of eating habits.18
Socioeconomic and family factors are directly associated with the development of preescholers’ eating habits.19 Although maternal education is the most studied variable and a strong influence on the outcomes of health and nutrition,20 in the present study it was low paternal education that was associated with lower consumption of fruits and vegetables. There is evidence that low parental education is related to less understanding of health needs and a lower degree of child care,21 also interfering with the knowledge and understanding of nutritional recommendations and requirements.19,22 Thus, as observed in this study, other researchers found that parents with low educational level offer fewer fruits and vegetables to their children.23,24
The results of this study demonstrated that children from higher-income families were less likely to consume fruits. However, it is important to emphasize that, in the present study, the sample consisted only of families of low socioeconomic status, and that the comparison between the different levels of income was performed only in this group. Thus, a hypothesis for this finding is that, in this population, among families with higher income, fruits are being replaced by processed foods with higher energy density, due to higher purchasing power25 and greater capacity for the acquisition of these foods.14
A study performed in Brazil observed that increased consumption of foods with high energy density may be associated with reduced consumption of traditional foods in the diet of Brazilians.14 It was also observed that dietary patterns characterized by high intake of sweets, soft drinks, and snacks are more frequent in populations with higher purchasing power.14,26 Studies in other developing countries observed similar results, associating highly energetic dietary patterns with higher-income families.27,28
This study has limitations that need to be acknowledged. The low socioeconomic status of the study population does not allow for the extrapolation of the present results to other populations. However, this population that uses the Brazilian Public Health System centers has greater biological and social vulnerability when compared with the population with higher socioeconomic status, which require care and effective health promotion strategies. Another limitation to be considered is that the assessed children participated in a randomized field trial, and the performed intervention may have influenced the results.
However, minimizing the effects of the intervention, the group variable was included in the regression, with the purpose of serving as a control for its effect and was shown not to be associated with outcomes. Moreover, it was not possible to assess the factors associated with insufficient consumption of fruits and vegetables, as over 90% of the children did not consume the recommended three daily servings.
The results of this study demonstrate that high prevalence of children aged 2–3 years, treated at Brazilian basic health care centers, eat less than one serving of fruits and vegetables per day and suggest that low paternal education and feeding practices during the first year of life are involved in this process. Thus, the implementation of healthy eating practices in childcare by health professionals is of utmost importance, since it was demonstrated by the randomized field trial29,30 that mothers with low purchasing power improve the quality of the food given to their children after receiving dietary counseling.
FundingFundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Valmórbida JL, Vitolo MR. Factors associated with low consumption of fruits and vegetables by preschoolers of low socio-economic level. J Pediatr (Rio J). 2014;90:464–71.
Study conducted at the Núcleo de Pesquisa em Nutrição (NUPEN) of the Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA).




