


To investigate the association between smoking and asthma, and possible associated factors in Brazilian adolescents.
MethodsA cross-sectional, national, school-based study with adolescents aged 12–17 years, participants in the Study of Cardiovascular Risks in Adolescents (Estudo de Riscos Cardiovasculares em Adolescentes – ERICA). A total of 66,394 participants answered a self-administered questionnaire with questions about asthma, smoking, lifestyle and sociodemographic variables. Bivariate analysis between Current Asthma (CA) and Severe Asthma (SA) and the other study variables were performed using Chi-squared. Then, the crude and adjusted Prevalence Ratios (PR), and respective 95% Confidence Intervals (95% CI) of current asthma/severe asthma and smoking variables, corrected for sociodemographic and lifestyle variables, were estimated using generalized linear models with Poisson regression, logit link, and robust variance.
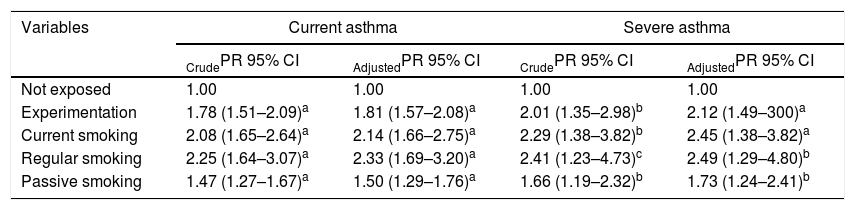
ResultsThe prevalence of current asthma and severe asthma were significantly higher in adolescents who were exposed to: experimentation (current asthma: PR=1.78, 95% CI: 1.51–2.09; severe asthma: PR=2.01; 95% CI: 1.35–2.98); current smoking (current asthma: PR=2.08, 95% CI: 1.65–2.64; severe asthma: PR=2.29; 95% CI: 1.38–3.82); regular smoking (current asthma: PR=2.25, 95% CI: 1.64–3.07; severe asthma: PR: 2.41; 95% CI: 1.23–4.73); and passive smoking (current asthma: PR=1.47, 95% CI: 1.27–1.67; severe asthma: PR=1.66; 95% CI: 1.19–2.32); these associations remained significant after adjustment.
ConclusionsAsthma and smoking were significantly associated in Brazilian adolescents, regardless of the sociodemographic and lifestyle factors, notably in those with more severe disease.
Investigar a associação entre asma, tabagismo e possíveis fatores associados em adolescentes brasileiros.
MétodosEstudo transversal, nacional, de base escolar, envolveu adolescentes com 12 a 17 anos, participantes do Estudo de Riscos Cardiovasculares em Adolescentes (ERICA). Os 66.394 participantes responderam questionários autopreenchíveis com questões sobre asma, tabagismo, estilo de vida e dados sociodemográficos. Foram realizadas análises bivariadas entre asma ativa e asma grave e demais variáveis do estudo, com o uso de χ2. Em seguida, foram estimadas as razões de prevalência (RP) brutas e ajustadas e seus respectivos intervalos de confiança de 95% (IC 95%), entre asma ativa/asma grave e variáveis de tabagismo, corrigidas pelas variáveis sociodemográficas e de estilo de vida, através de modelos lineares generalizados com regressão de Poisson, função de ligação logarítmica e variância robusta.
ResultadosA prevalência de asma ativa e asma grave foi significativamente mais elevada naqueles expostos a experimentação (asma ativa: RP=1,78; IC 95%: 1,51–2,09; asma grave: RP=2,01; IC 95%: 1,35–2,98); tabagismo atual (asma ativa: RP=2,08; IC 95%: 1,65–2,64; asma grave: RP=2,29; IC 95%: 1,38–3,82); tabagismo frequente (asma ativa: RP=2,25; IC 95%: 1,64–3,07; AG=2,41; IC 95%: 1,23–4,73) e tabagismo passivo (asma ativa: RP=1,47; IC 95%: 1,27–1,67; asma grave: RP=1,66; IC 95%: 1,19–2,32). As associações permaneceram significativas após ajuste.
ConclusãoA asma e o tabagismo se associaram de modo significativo em adolescentes brasileiros independente de fatores sociodemográficos e estilo de vida, especialmente naqueles com doença mais grave.
Asthma is a disease with high prevalence worldwide in all age groups, from childhood to adulthood.1 The prevalence of asthma in adolescents aged 13–14 years in Brazil was estimated at 19%, according to data from the International Study of Asthma and Allergies in Childhood (ISAAC),2 therefore representing a serious public health problem in the country.
As a complex and multifactorial condition, asthma can be influenced by both genetics and environmental factors, such as family history of atopy, gender, type and number of childhood infections, socioeconomic status, lifestyle, obesity, exposure to inhalant allergens, and environmental pollution.3,4 In relation to this last factor, smoking is emphasized.
Overall, factors associated with experimentation and persistence of smoking are the same for asthmatic and non-asthmatic individuals,5 of which the most important are having parents or friends who smoke, not living with both parents, and low socioeconomic level.6
According to the National Adolescent School-based Health Survey (Pesquisa Nacional de Saúde do Escolar – PeNSE 2012), 22.6% (95% CI: 21.7–23.5%) of Brazilian adolescents have experimented with smoking and 6.1% (95% CI: 5.6–6.6%) are regular smokers.7 Therefore, smoking constitutes a public health problem in this age group.
Smoking is associated with poorer asthma control in adults.8 Similarly, children and adolescents exposed to maternal smoking, both in the pre- and postnatal periods, are more likely to develop wheezing episodes and be diagnosed with asthma than the non-exposed.9,10 Regular smoking in adolescence is associated with greater prevalence, severity, and frequency of asthma symptoms.10,11
Therefore, the aim of the present study was to investigate the association between asthma, smoking, and associated risk factors in Brazilian adolescents.
MethodsStudy design and populationThis study is part of the Study of Cardiovascular Risks in Adolescents (Estudo de Riscos Cardiovasculares em Adolescentes – ERICA) and, as such, followed its methodological precepts. This is a multicenter, national, school-based study carried out in a randomized sample of adolescents aged 12–17 years, representative of the group of adolescents enrolled in schools in municipalities with more than 100,000 inhabitants at national and regional level, and of each capital and the Federal District. A more detailed description of the sample design has been published elsewhere by Vasconcellos et al.12
Data collectionThe selected students answered self-administered questionnaires that included questions about physical activity, eating behavior, smoking, alcohol consumption, oral health, common mental disorders, reproductive health, medical history of chronic diseases, among them asthma, and sleep. Data collection was carried out using microcomputers (Personal Digital Assistant – PDA) and was supervised by field staff previously trained to apply the standardized study techniques.13
The presence of asthma was defined by the question: “In the last 12 months (one year), how many wheezing crises attacks of wheezing did you have?” This question was extracted from the ISAAC asthma module for the age of 13–14 years, translated and validated for Brazilian culture.14 A positive response shows high sensitivity and specificity compared to objective measurements of pulmonary function in asthmatic adolescents.14,15 The ISAAC questionnaire shows a good correlation between the responses of adolescents and their parents.16,17
The prevalence of Current Asthma (CA) was defined by the presence of at least one wheezing crisis attack in the last 12 months,18 and Severe Asthma (SA) by four or more crises attacks in the same period, according to previously defined criteria.9,19
The variables associated with smoking were defined as follows: “experimentation”, adolescents who have smoked cigarettes at some point at least once in their lives; “current smoking”, those who have smoked cigarettes on at least one day in the past 30 days; “regular smoking”, those who smoked cigarettes for at least seven consecutive days in the past 30 days, and “passive smoking”, those who had at least one smoker in the household.6 Different studies have shown that these questions have a good correlation with levels of salivary cotinine, a nicotine metabolite used as a marker of both active and passive exposure to tobacco.20
Additionally, the following sociodemographic variables were analyzed: gender, age group (12–14 years or 15–17 years), ethnicity (black or white/other), and type of school (public or private). Physical activity was assessed using an adapted version of the Self-Administered Physical Activity Checklist, previously validated for Brazilian adolescents.21 Participants with less than 300minutes of weekly physical activity were classified as sedentary and those with 300min or more, as active.21
Statistical analysisDescriptive statistics were reported as frequencies and means. Bivariate analyses were performed between CA and SA with the other study variables, using the Chi-squared test. Then, the crude and adjusted Prevalence Ratios (PRs) and their respective 95% Confidence Intervals (95% CI) between CA/SA and the smoking variables, corrected for sociodemographic and lifestyle variables, were estimated using Generalized Linear Models (GLM) with Poisson regression, logit link, and robust variance. For the purpose of the analysis, the smoking variables were considered as mutually exclusive. The linear Chi-squared test was used to evaluate the association between CA and number of smokers in the household. The data were analyzed using commands for the analysis of complex samples (survey) of Stata software, version 14.0 (StataCorp – College Station, TX, USA).
Ethical aspectsThe study followed the principles of the Declaration of Helsinki and was approved by the Research Ethical Committees of the Institute of Collective Health Studies of Universidade Federal do Rio de Janeiro – Process n° 45/2008 of 11/2/2009. Student privacy and data confidentiality were guaranteed throughout the study.
ResultsBetween years 2013 and 2014, the questionnaires answered by 74,589 adolescents were collected.22 Those who answered “I do not know/I do not remember” to the question about asthma were excluded from the analysis. The distribution of the variables of interest in this group did not vary significantly from the rest of the sample; therefore, 66,394 adolescents were included in the final analysis (Fig. 1).

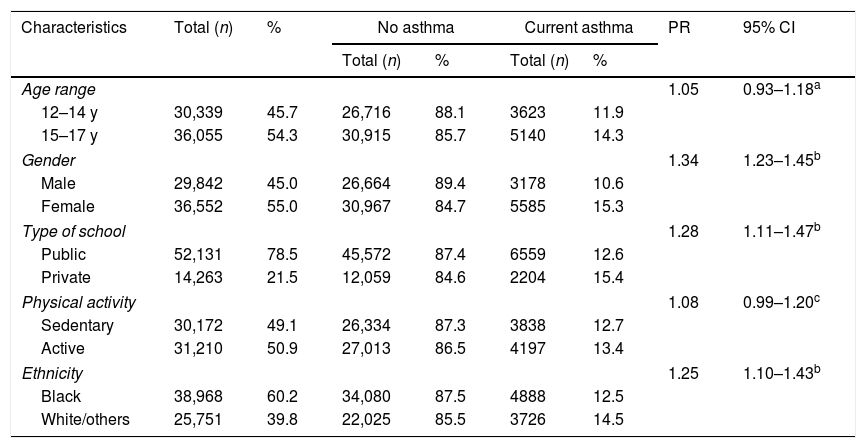
The prevalence of CA and SA was 13.2% (95% CI: 12.9–13.5) and 2.4% (95% CI: 2.3–2.5), respectively. Approximately half of the assessed adolescents were between 15 and 17 years old and 55% were females (Table 1). The prevalence of current asthma was significantly higher among female students, those of white/other ethnicity, and those enrolled in private schools. However, there was no association between CA and physical activity or age group (Table 1).
Overall characteristics of the participants according to the diagnosis of current asthma. ERICA, Brazil, 2012–2014.
| Characteristics | Total (n) | % | No asthma | Current asthma | PR | 95% CI | ||
|---|---|---|---|---|---|---|---|---|
| Total (n) | % | Total (n) | % | |||||
| Age range | 1.05 | 0.93–1.18a | ||||||
| 12–14 y | 30,339 | 45.7 | 26,716 | 88.1 | 3623 | 11.9 | ||
| 15–17 y | 36,055 | 54.3 | 30,915 | 85.7 | 5140 | 14.3 | ||
| Gender | 1.34 | 1.23–1.45b | ||||||
| Male | 29,842 | 45.0 | 26,664 | 89.4 | 3178 | 10.6 | ||
| Female | 36,552 | 55.0 | 30,967 | 84.7 | 5585 | 15.3 | ||
| Type of school | 1.28 | 1.11–1.47b | ||||||
| Public | 52,131 | 78.5 | 45,572 | 87.4 | 6559 | 12.6 | ||
| Private | 14,263 | 21.5 | 12,059 | 84.6 | 2204 | 15.4 | ||
| Physical activity | 1.08 | 0.99–1.20c | ||||||
| Sedentary | 30,172 | 49.1 | 26,334 | 87.3 | 3838 | 12.7 | ||
| Active | 31,210 | 50.9 | 27,013 | 86.5 | 4197 | 13.4 | ||
| Ethnicity | 1.25 | 1.10–1.43b | ||||||
| Black | 38,968 | 60.2 | 34,080 | 87.5 | 4888 | 12.5 | ||
| White/others | 25,751 | 39.8 | 22,025 | 85.5 | 3726 | 14.5 | ||
PR, prevalence ratio; 95% CI, 95% confidence interval.
Regarding smoking, 18.2% (95% CI: 17.3–19.1) of the adolescents experimented with cigarettes, of whom 25.3% were classified as “current smokers” and 11.8% as “regular smokers”. The prevalence of adolescents with at least one smoker in the household was 27.5% (95% CI: 26.6–28.3), while 60.8% (95% CI: 59.8–61.9) were not exposed to smoking.
Asthma was significantly associated with all evaluated smoking variables, and these associations remained for both CA and SA after adjusting for sociodemographic variables (Table 2).
Crude and adjusted analysis between current asthma/severe asthma and smoking variables. ERICA, Brazil, 2013–2014.
| Variables | Current asthma | Severe asthma | ||
|---|---|---|---|---|
| CrudePR 95% CI | AdjustedPR 95% CI | CrudePR 95% CI | AdjustedPR 95% CI | |
| Not exposed | 1.00 | 1.00 | 1.00 | 1.00 |
| Experimentation | 1.78 (1.51–2.09)a | 1.81 (1.57–2.08)a | 2.01 (1.35–2.98)b | 2.12 (1.49–300)a |
| Current smoking | 2.08 (1.65–2.64)a | 2.14 (1.66–2.75)a | 2.29 (1.38–3.82)b | 2.45 (1.38–3.82)a |
| Regular smoking | 2.25 (1.64–3.07)a | 2.33 (1.69–3.20)a | 2.41 (1.23–4.73)c | 2.49 (1.29–4.80)b |
| Passive smoking | 1.47 (1.27–1.67)a | 1.50 (1.29–1.76)a | 1.66 (1.19–2.32)b | 1.73 (1.24–2.41)b |
Notes: CrudePR, crude prevalence ratio; AdjustedPR, prevalence ratio adjusted by gender, age, ethnicity and school type; 95% CI, 95% confidence interval.
Fig. 2 shows a progressive and statistically significant increase in asthma prevalence according to the number of smokers in the household. This tendency is observed up to the presence of three smokers, but from this point on, the increase in the prevalence of asthma is independent from the exposure load.
.")
It was also observed that the distribution of the association between CA and regular smoking in all Brazilian macro-regions was statistically significant: North (PR=1.81; 95% CI: 1.39–2.36); Northeast (PR=1.93; 95% CI: 1.46–2.54); Midwest (PR=1.93; 95% CI: 1.72–2.69); Southeast (PR=1.88; 95% CI: 1.53–2.31); and South (PR=1.67; 95% CI: 1.34–2.08).
DiscussionThe prevalence of CA was significantly higher in adolescents exposed to different levels of smoking. These associations were independent from age, gender, ethnicity, and lifestyle. These findings are compatible with those of similar international studies carried out in this age group. In 2004, a cross-sectional study carried out in North Carolina, United States, evaluated 128,568 students attending seventh and eighth grades, and found a significant association between asthma and current smoking (OR=1.47, 95% CI: 1.41–1.54), and passive smoking (OR=1.12; 95% CI: 1.08–1.17).10 Similarly, a cross-sectional study carried out in Salta, Argentina, with 3000 adolescents (13–14 years old) participating in the ISAAC study, showed an association between passive smoking and asthma (OR=1.83; 95% CI: 1.42–2.35).23
In the present study, SA showed an association with smoking that was even more significant than CA. Recent studies have shown that asthmatic smokers, when compared to nonsmokers, have a predominant pattern of non-eosinophilic inflammation, with a higher proportion of neutrophils in the airways, which may contribute to a worse response of smokers to the maintenance therapy with inhaled corticosteroids.24 Although spirometry data and asthma therapy have not been evaluated in the present sample, it is speculated that the higher number of exacerbations in adolescents with more severe disease could be a result of poorer lung function and/or a poorer response to the conventional anti-inflammatory treatment.
Moreover, a longitudinal study carried out in 2007 observed that the association between asthma and smoking in adolescents seemed to have a bidirectional association, in which those with more severe symptoms tended to be at increased risk of becoming smokers, whereas the habit of smoking was a predictive factor for a higher incidence of asthma.11
Most studies show an equal or increased prevalence of smoking in asthmatics when compared to non-asthmatics,5,11,25 indicating that these individuals assume a risk behavior when they start smoking, although the majority are aware of the fact that smoking can exacerbate their asthma. It was observed in a study with 3234 adolescents aged 15–18 years in Memphis, United States, that individuals with current asthma more often reported the intention to start smoking in the following year than those without the disease.25 Corroborating this finding, a study carried out in Rio de Janeiro, Brazil, observed that adolescents with chronic diseases do not seem to perceive their condition as a disease, but only as a “problem”, considering the risk as something distant and impersonal, rather than as a potential factor for disease worsening.26 In this context, adolescents with asthma may be more predisposed to smoking, aggravating symptoms and disease control.
Thus, it is recommended that the attending physician routinely checked exposure to smoking and associated risk factors, aiming to provide and reinforce appropriate preventive measures for this age group.27 In a study carried out in Uruguaiana, in Southern Brazil, which evaluated 798 adolescents, the most important risk factors associated with smoking were: having friends who smoked, being offered cigarettes by peers, and easy access to cigarettes.28
The present data show that the prevalence of CA was directly proportional to the number of smokers in the household, suggesting a dose-effect association between asthma and passive smoking. Similar findings were observed by Mitchell et al. in a global ISAAC – phase III analysis, comprising approximately 350,000 adolescents aged 13–14 years, which showed a significant association between CA and maternal and paternal smoking, especially among those with more severe asthma. Furthermore, a clear dose-response association was observed between asthma symptoms and the number of cigarettes smoked by the parents.9
According to the Brazilian Demographic Census of 2015, four out of ten families are headed and supported by women.29 For this reason, the present data appear to be in agreement with other studies that indicate maternal smoking and the number of smokers in the household as important factors associated with the presence of asthma, as well as the presence of more severe disease. This hypothesis is reinforced by a study carried out with adolescents in Nova Iguaçu, state of Rio de Janeiro, which showed an association between CA and maternal smoking, but not with paternal smoking.3
The socioeconomic level of the sample was not objectively evaluated; however, a significant association between CA and attending private schools was observed. Recent data from national research institutes have shown that, in general, private school students have a higher socioeconomic level and a better quality of education than those in the public system.30 In this context, the present results contradict those of other studies that reported a higher prevalence of asthma in individuals with a lower socioeconomic level.4 However, the association between asthma and smoking persists even after adjusting for the type of school and other sociodemographic variables of the study. Another relevant finding of this study is that frequent smoking is associated with CA in adolescents in all Brazilian geographic macro-regions, despite the country's continental dimensions, as well as its climatic and cultural differences. These data highlight the need to strengthen anti-smoking policies focused on this age group throughout the national territory.
The prevalence of asthma in Brazilian adolescents according to ERICA was lower than that observed in 2003 in ISAAC – phase III. It would be possible to infer from these data that there was a real reduction in the prevalence of asthma during this period; however, the age group evaluated by ERICA should be considered, which was broader, as it included older adolescents and may have affected this finding. Additionally, the original ISAAC question for the evaluation of current asthma (“wheezing episodes in the last 12 months”) has been rewritten in ERICA (“wheezing crises attacks of wheezing in the last 12 months”), which may have reduced its sensitivity, by excluding participants with milder or well-controlled disease.
Among other limitations of the present study are those originated from its cross-sectional design, which does not allow the establishment of a temporal or causal relation in the observed associations. However, the sample size and representativeness, the use of standardized questionnaires and trained field researchers, in addition to the consistency of the results with those of other longitudinal studies, increase the importance of these findings.
Therefore, a significant association was observed between smoking and asthma in Brazilian adolescents, particularly among those with more severe disease, regardless of sociodemographic and lifestyle factors. Considering that both asthma and smoking are challenges in adolescence, the authors emphasize that the consolidation and increase of public health measures to reduce the exposure/prevalence of smoking in this age group in Brazil, especially in asthmatic individuals, should consider the susceptibilities and specific characteristics of this population group.
FundingThe Study of Cardiovascular Risks in Adolescents (ERICA) was funded by the Department of Science and Technology of the Science, Technology and Strategic Inputs Secretariat of the Ministry of Health (Decit/SCTIE/MS), Health Sector Funding of the Ministry of Science, Technology and Innovation (MCTI). FINEP protocols: 01090421 and CNPq: 565037/2010-2 and 405009/2012-7; and Research Incentive Fund of Hospital das Clínicas de Porto Alegre (FIPE-HCPA – Process 405.009/2012-7).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Jordão EA, Kuschnir FC, Figueiredo VC, Félix MM, Silva TL, Kuschnir MC, et al. ERICA: smoking is associated with more severe asthma in Brazilian adolescents. J Pediatr (Rio J). 2019;95:538–44.




