


The objective of this study was to evaluate the health-related quality of life in children and adolescents with autoimmune hepatitis.
MethodsA cross-sectional assessment with the Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) was completed for 80 patients with autoimmune hepatitis and 45 healthy controls. Demographic data, prednisone dose, disease remission state, disease severity, and abdominal pain were also evaluated.
ResultsBased on the child self-reports, physical, emotional, school, and total scores were significantly lower in autoimmune hepatitis patients when compared with controls (p<0.05). Based on the parental reports, only the physical and total scores were significantly lower in autoimmune hepatitis patients versus controls (p<0.05). Further analysis in autoimmune hepatitis patients with abdominal pain in the last month revealed significantly lower physical, social, and total median scores (p<0.05). No differences were observed based on disease remission state or disease severity (p>0.05). Autoimmune hepatitis patients who received a prednisone dose below 0.16mg/kg/day at the time of the interview showed significantly higher physical scores than those who received a dose similar to or above 0.16mg/kg/day (87.5 [50–100] vs. 75 [15.63–100], p=0.006).
ConclusionsReduced scores in the physical, emotional, and school domains were observed in pediatric autoimmune hepatitis patients compared to control patients. Abdominal pain and corticosteroid dose negatively influenced the health-related quality of life in children and adolescents with autoimmune hepatitis.
Avaliar a qualidade de vida relacionada à saúde em crianças e adolescentes com hepatite autoimune (HAI).
MétodosFoi concluída uma avaliação transversal com o Inventário Pediátrico de Qualidade de Vida 4.0 (PedsQL 4.0) para 80 pacientes com hepatite autoimune e 45 controles saudáveis. Os dados demográficos, a dose de prednisona, o estado de remissão da doença, a gravidade da doença e dor abdominal também foram avaliados.
ResultadosCom base nos autorrelatos das crianças, os escores físico, emocional, escolar e total foram significativamente menores em pacientes com hepatite autoimune em comparação com os controles (p < 0,05). Com base nos relatos dos pais, apenas os escores físico e total foram significativamente menores em pacientes com hepatite autoimune em comparação com os controles (p < 0,05). Uma análise adicional em pacientes com hepatite autoimune com dor abdominal no mês passado revelou escores médios físico, social e total significativamente menores (p < 0,05). Nenhuma diferença foi observada com base no estado de remissão da doença ou na gravidade da doença (p > 0,05). Os pacientes com hepatite autoimune que receberam uma dose de prednisona abaixo de 0,16mg/kg/dia no momento da entrevista mostraram escores físicos significativamente maiores que os que receberam uma dose semelhante ou acima de 0,16mg/kg/dia [87,5 (50-100) em comparação com 75 (15,63-100), p = 0,006].
ConclusõesEscores reduzidos nos domínios físico, emocional e escolar foram observados em pacientes pediátricos com hepatite autoimune em comparação com pacientes do grupo de controle. Dor abdominal e dose de corticosteroide influenciaram negativamente a qualidade de vida relacionada à saúde em crianças e adolescentes com hepatite autoimune.
Autoimmune hepatitis (AIH) is a chronic and progressive inflammatory disorder of the liver. AIH is immune-mediated, characterized by high serum aminotransferase and immunoglobulin G (IgG) levels, and detectable by autoantibodies and histological evidence of interface hepatitis in the absence of a known etiology. AIH is a rare condition with a reported incidence of 0.4–3 per 100,000 children. AIH may occur jointly with other autoimmune diseases, such as type I diabetes, hypothyroidism, and systemic lupus erythematosus.1,2 The prevalence of AIH/sclerosing cholangitis and overlap syndromes is 48%.3
The clinical presentation of AIH is highly variable in children, ranging from acute hepatitis to an insidious onset with progressive fatigue, intermittent jaundice, anorexia, and weight loss.4 The primary goal of immunosuppressive treatments is to improve clinical manifestations and laboratory findings.1,4 A common treatment is prednisone, which may lead to side effects such as hypertrichosis, weight gain, and linear growth restriction; these effects may affect self-image and negatively influence emotional health, thus jeopardizing the health-related quality of life (HRQOL) in children and adolescents with AIH.4
Chronic liver disease is a leading cause of death worldwide and is the cause of disability in a large segment of the economically active population.5 In this context, the HRQOL of patients with chronic liver disease since childhood or adolescence is an important health determinant.
The life expectancy of pediatric chronic liver disease patients has significantly improved over the last decade, with patient-perceived health-related quality of life (HRQOL) assuming a greater role in determining the quality of the enhanced survival of these pediatric patients.6 Therefore, HRQOL measurement instruments for children, adolescents, and their parents have been developed.
General HRQOL instruments are multidimensional, aiming to evaluate the impact of a disease as a function of pain, general health, vitality, social and emotional aspects, and mental health. The instruments are well-designed to evaluate the effectiveness of health policies and programs or to compare two distinct diseases. Specific instruments focus on the symptoms, disabilities, and limitations associated with a particular disease; however, no specific questionnaire for AIH is available in the literature.7
The authors chose the Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) generic version questionnaire for this study due to its ease of use and its global assessments, including physical, emotional, social, and school aspects; it also allows the assessment of parents perception of their child's HRQOL.8
HRQOL has been rarely studied in adult and pediatric AIH populations using generic instruments.9,10 Negative emotional aspects have been observed in adult AIH patients when compared with the general population, regardless of disease remission status.9 In Brazil, no studies that specifically address the HRQOL of children and adolescents with AIH were retrieved.
To the best of the authors’ knowledge, there is only one report that evaluated HRQOL in AIH patients with a sample of 22 AIH children and adolescents, including those who had undergone liver transplantation showing decreased HRQOL in these patients.10 However, an analysis of HRQOL domains in pediatric patients without liver transplantation, including comparisons of the disease remission status, disease severity, and corticosteroid dose, has not been previously completed.
The objectives of this study were to assess the HRQOL in AIH patients and healthy controls using the generic PedsQL 4.0 instrument for children/adolescents and parents/guardians and to evaluate the possible influence of disease remission status, disease severity, and prednisone dose on HRQOL.
Patients and methodsFrom March to December 2016, a cross-sectional study was performed with 80 AIH patients at two pediatric hepatology units of tertiary hospitals (Instituto da Criança da Faculdade de Medicina da Universidade de São Paulo and Hospital Infantil Municipal Menino Jesus) in São Paulo, Brazil. All patients were systematically evaluated, and the diagnosis of AIH was confirmed in accordance with the International Group of Autoimmune Liver Disease criteria.11,12 This study was approved by the Hospitals’ Ethical Committees. Patients, controls, and their parents/guardians signed informed consent forms.
SamplePatients were selected using a convenience sampling method. AIH patients were from different regions of Brazil, and although they were followed-up at two pediatric hepatology units located in São Paulo, they were not exclusively from this city. The inclusion criteria were (i) age between 5 and 18 years; and (ii) confirmed diagnosis of autoimmune hepatitis. The exclusion criteria were (i) patients who underwent liver transplant; (ii) patients who refused to participate in the study; (iii) patients with fulminant hepatitis; and (iv) patients who had not received any prior treatments.
Control groupThe control group consisted of 45 healthy children and adolescents with a similar age profile as the patients [13 (5–18) vs. 14 (3–18); p=0.804] from a local public school in Cuiabá, Brazil.
HRQL assessmentsThe HRQOL was determined using the (PedsQL 4.0), which was validated for the Brazilian Portuguese language and culture. Three versions were used, based on the patient's age: 5–7, 8–12, or 13–18 years.7,8
Two instruments were used in the present study: the PedsQL 4.0 child self-report and the PedsQL 4.0 parental report. The PedsQL 4.0 questionnaire includes questions related to the following four multidimensional domains: physical capacity, emotional aspects, social aspects, and school activities over the previous month. The score consists of 23 items, which are scored using a five-point scale in the 8–12 years group, the 13–18 years group and the parent groups (0 – never=100 points; 1 – almost never=75 points; 2 – sometimes=50 points; 3 – often=25 points; and 4 – almost always=0 points) and a three-point scale for the 5–7-year-old group (0 – never=100 points; 2 – sometimes=50 points; and 4 – often=0 points). The median scores ranged from 0 to 100, and a higher score indicates a better HRQOL.13,14
Demographic, clinical, laboratory, and therapeutic evaluationsPatients’ medical charts were meticulously reviewed according to an extensive standardized protocol to assess demographic data, clinical features, laboratory findings, and therapeutic data.
Demographic data included current age, gender, and disease duration (time between diagnosis and interview). AIH was classified as AIH type 1 (presence of antinuclear antibodies [ANA] and/or anti-smooth muscle antibody [SMA]) or AIH type 2 (presence of anti-type I liver-kidney microsomal antibody [anti-LKM-1] and/or anti-liver cytosol antibody [anti-LC1]).15,16 Overlap syndrome was defined as AIH associated with autoimmune sclerosing cholangitis based on clinical/biochemical features of cholestasis and histological or cholangiographic findings.17 Other autoimmune diseases were also assessed, including type 1 diabetes mellitus (T1DM; assessed based on polyuria, polydipsia, unexplained weight loss, and increased plasma glucose ≥200mg/dL at any time of the day or fasting glucose ≥126mg/dL)18 and childhood-onset systemic lupus erythematosus (cSLE), in accordance with the American College of Rheumatology classification criteria.19 Data concerning prednisone, azathioprine, and other immunosuppressive drugs were also collected, as well as laboratory findings at study entry.
Incomplete remission or non-remission was defined as aminotransferase levels two times greater than the normal upper limit, as well as a high concentration of IgG or serum gamma globulin.20
Remission was characterized as levels of aminotransferases (AST/ALT) and IgG below the normal upper limit.20
Disease severity was defined as a previous history of complications, such as portal hypertension, upper gastrointestinal bleed, ascites, and/or spontaneous bacterial peritonitis.21 No patients presented with these complications at the time of the interview.
Prednisone dosePatients were arbitrarily divided into two groups according to the median prednisone dose at the time of the interview: group A (<0.16mg/kg/day) and group B (≥0.16mg/kg/day).
Statistical analysesStatistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, version 22.0, NY, USA). Mann–Whitney tests or t-tests were used to compare continuous variables, which were presented as median (range) or mean±standard deviation (SD), respectively. Differences in frequencies for categorical variables were assessed by Fisher's exact test. p-Values were set at 5% (p<0.05) for all statistical tests.
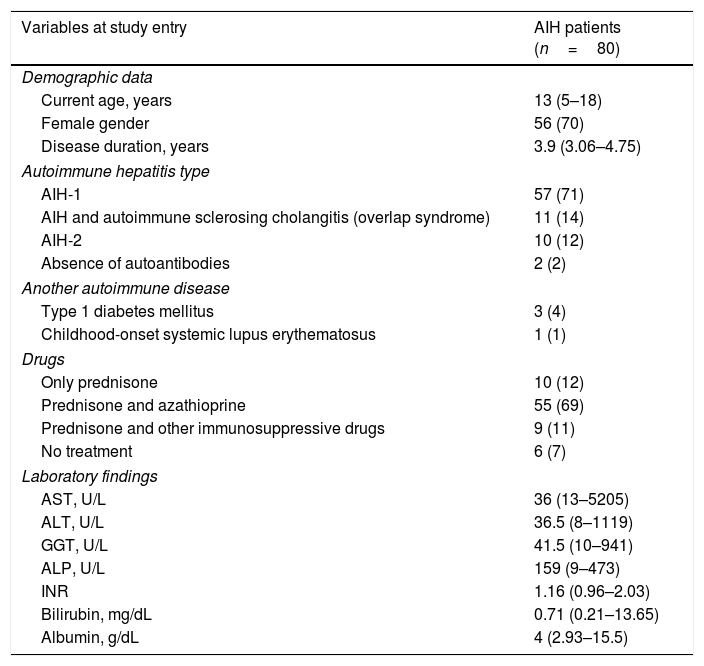
ResultsTable 1 includes demographic data, AIH types, other autoimmune diseases, medications and laboratory findings in AIH patients. The median current age was similar for AIH patients and healthy controls [13 years (5–18) vs. 14 years, (3–18) p=0.804]. Type 1 AIH was observed in 57 patients (71%), autoimmune sclerosing cholangitis was observed in 11 patients (14%), Type 2 AIH was observed in ten patients (12%), and an absence of autoantibodies was seen in two patients (2%). T1DM comorbidity was observed in three patients (4%) and cSLE comorbidity was observed in one patient (1%).
Demographic data, autoimmune hepatitis (AIH) types, other autoimmune diseases, drugs, and laboratory findings for AIH patients at study entry.
| Variables at study entry | AIH patients (n=80) |
|---|---|
| Demographic data | |
| Current age, years | 13 (5–18) |
| Female gender | 56 (70) |
| Disease duration, years | 3.9 (3.06–4.75) |
| Autoimmune hepatitis type | |
| AIH-1 | 57 (71) |
| AIH and autoimmune sclerosing cholangitis (overlap syndrome) | 11 (14) |
| AIH-2 | 10 (12) |
| Absence of autoantibodies | 2 (2) |
| Another autoimmune disease | |
| Type 1 diabetes mellitus | 3 (4) |
| Childhood-onset systemic lupus erythematosus | 1 (1) |
| Drugs | |
| Only prednisone | 10 (12) |
| Prednisone and azathioprine | 55 (69) |
| Prednisone and other immunosuppressive drugs | 9 (11) |
| No treatment | 6 (7) |
| Laboratory findings | |
| AST, U/L | 36 (13–5205) |
| ALT, U/L | 36.5 (8–1119) |
| GGT, U/L | 41.5 (10–941) |
| ALP, U/L | 159 (9–473) |
| INR | 1.16 (0.96–2.03) |
| Bilirubin, mg/dL | 0.71 (0.21–13.65) |
| Albumin, g/dL | 4 (2.93–15.5) |
Results are shown as median (range) and n (%).
When assessing the clinical characteristics of all interviewed patients, the most common complaint was abdominal pain, which was reported by 20 AIH patients (25%). Only one patient complained of hypertrichosis as a side effect of prednisone use, and there were no complaints of weight gain or stretch marks. A history of portal hypertension was detected in seven patients (58.4%), a history of upper gastrointestinal bleed was present in two patients (16.6%), and a history of ascites was detected in three patients (25%). Remission was observed in 62 (77.5%) AIH-1 and AIH-2 patients, and incomplete or non-remission was observed in 18 AIH-1 patients (22.5%).
Table 2 illustrates the PedsQL 4.0 patient scores compared to healthy controls and parental scores compared to control parents. The physical, emotional, school, and total scores were significantly lower in AIH patients compared to healthy controls. Physical and total scores were significantly lower in AIH parents compared to control parents.
Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) scores according to reports of autoimmune hepatitis (AIH) patients, healthy controls, and parents.
| Variables | AIH patients (n=80) | Controls (n=45) | p |
|---|---|---|---|
| Physical | 81.25 (15.63–100) | 96.88 (50–100) | <0.001 |
| Emotional | 65 (5–100) | 75 (40–100) | 0.020 |
| Social | 100 (20–100) | 90 (45–100) | 0.427 |
| School | 75 (20.8–100) | 90 (40–100) | 0.01 |
| Total score | 78.25 (36.61–97.5) | 85.63 (56.41–100) | <0.001 |
| AIH parents (n=58) | Controls parents (n=47) | p | |
|---|---|---|---|
| Physical | 84.37 (3.13–100) | 96.88 (53.13–100) | <0.001 |
| Emotional | 67.5 (5–100) | 75 (25–100) | 0.071 |
| Social | 100 (10–100) | 90 (45–100) | 0.120 |
| School | 77.50 (20–100) | 85 (35–100) | 0.246 |
| Total score | 79.06 (35.47–100) | 86.25 (57.5–100) | 0.016 |
Results are presented as median (range) by Mann–Whitney test.
Table 3 demonstrates the lower median physical, social, and total scores observed in AIH patients who presented with abdominal pain when compared those who presented without abdominal pain. A significant impairment in HRQOL was observed in the physical, social, school, and total scores in AIH patients with abdominal pain based on the parental report.
Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) scores of autoimmune hepatitis (AIH) children, adolescents, and parents according to the presence of abdominal pain.
| Variables | Without abdominal pain (n=60) | With abdominal pain (n=20) | p |
|---|---|---|---|
| AIH children | |||
| Physical | 84.37 (50–100) | 67.18 (15.63–100) | 0.013 |
| Emotional | 65 (20–100) | 57.50 (5–100) | 0.701 |
| Social | 100 (20–100) | 85 (30–100) | 0.005 |
| School | 75 (20.8–100) | 68.98 (36.61–97.50) | 0.262 |
| Total | 79.13 (37.54–96.25) | 69.98 (36.61–97.50) | 0.017 |
| (n=42) | (n=16) | p | |
|---|---|---|---|
| AIH parents | |||
| Physical | 87.50 (43.75–100) | 75 (3.13–100) | 0.016 |
| Emotional | 65 (25–100) | 70 (5–95) | 0.910 |
| Social | 100 (20–100) | 95 (10–100) | 0.027 |
| School | 85 (55–100) | 67.50 (20–95) | 0.012 |
| Total | 81.79 (57.97–100) | 72.50 (35.47–93.13) | 0.016 |
Results are presented as median (range) by Mann–Whitney test.
The analysis of AIH patients in incomplete or non-remission when compared with those in remission revealed no significant median physical, emotional, social, school, or total scores in the AIH patient self-reports or in the AIH parental reports. An analysis based on disease severity did not show any significant differences in any domain in either patient or parental reports.
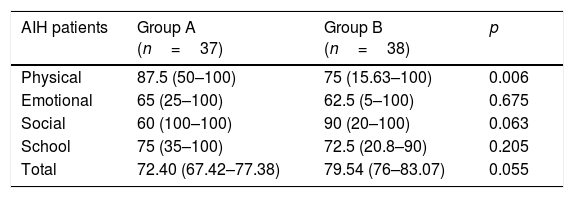
Further analysis of AIH patients based on prednisone dose, where group A received a prednisone dose of <0.16mg/kg/day and group B, ≥0.16mg/kg/day, revealed that the physical score was significantly lower in group B. No differences were observed in the physical, emotional, social, school, or total scores between prednisone dose groups based on parental reports (Table 4).
Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) scores of children and adolescents according to the median prednisone dose at the time of the interview: group A (<0.16mg/kg/day) versus group B (≥0.16mg/kg/day).
| AIH patients | Group A (n=37) | Group B (n=38) | p |
|---|---|---|---|
| Physical | 87.5 (50–100) | 75 (15.63–100) | 0.006 |
| Emotional | 65 (25–100) | 62.5 (5–100) | 0.675 |
| Social | 60 (100–100) | 90 (20–100) | 0.063 |
| School | 75 (35–100) | 72.5 (20.8–90) | 0.205 |
| Total | 72.40 (67.42–77.38) | 79.54 (76–83.07) | 0.055 |
| AIH parents | Group A (n=23) | Group B (n=31) | p |
|---|---|---|---|
| Physical | 86.41 (81.09–91.73) | 74.63 (66.36–82.90) | 0.056 |
| Emotional | 67.60 (58.36–76.84) | 63.22 (54.86–71.58) | 0.434 |
| Social | 91.95 (85.18–98.72) | 89.83 (81.79–97.88) | 0.965 |
| School | 79.13 (71.70–86.55) | 77.31 (72.53–82.08) | 0.578 |
| Total | 81.27 (76.66–85.89) | 76.25 (70.83–81.67) | 0.290 |
Results are presented as median (range) by Mann–Whitney test.
The present study was the first investigation of HRQOL in AIH pediatric patients in South America. The authors found reduced scores in almost all domains (physical, emotional, school, and total) in AIH patients when compared with controls.
Chronic conditions are known to jeopardize HRQOL at all ages, and although toddlers are often unable to express themselves verbally, they are able to communicate their problems. These signals should not be underestimated during the clinical consultation.22 In the case of adolescents, an improvement in HRQOL is crucial in promoting treatment adherence. Despite this importance, it is estimated that fewer than 25% of pediatricians use quality of life measurements in their consultations.23 There is a growing interest in adapting and creating instruments to measure HRQOL in children and adolescents, due to an increased prevalence of chronic diseases in this age group. Most of these instruments are quantitative and many of them are specific to certain diseases. A major challenge is to incorporate HRQOL measurements into clinical practice.7 Quality of life is a concept related to cultural aspects; thus, HRQOL measurement instruments must be adapted to local cultures and languages. There is no specific questionnaire for children and adolescents with autoimmune hepatitis (AIH), and little is known about the HRQOL of these patients.
The major advantages of the current study are the systematic assessment of the HRQOL in children and adolescents with autoimmune hepatitis using a relatively large sample, despite minimal previous studies, and the exclusion of patients who had undergone liver transplantation, since this condition may decrease HRQOL.24 Moreover, a healthy control group with a similar age profile was included in the present study. The main limitation of this study was the use of only one generic tool to measure the HRQOL in AIH children and their parents. A possible bias was the exclusive comparison with a healthy control group; however, there is no published data on the HRQOL of children and adolescents with chronic liver disease in Brazil for other comparisons. As the present sample was composed of children from different regions of Brazil, a control group from any region could be used with confidence.
Patient complaints regarding clinical manifestations were very poorly reported, with the exception of abdominal pain, which attracted the authors’ attention. The present data confirm previous reports that abdominal pain is associated with decreased HRQOL.10 This finding may be related to the side effects of immunosuppressive agents, AIH complications, or even psychosomatic manifestations.25
It was observed that corticosteroid dose is associated with decreased physical scores in children and adolescents with AIH.9 Even low doses of corticosteroids should not be underestimated, as these drugs could affect body composition and hypertrichosis, acne, stretch marks, weight gain, and growth disturbances, and thus affect HRQOL scores.26 Although these manifestations were not observed in the present sample, AIH patients’ physical scores were decreased.
Approximately one-fifth of the AIH patients in the present study were in incomplete remission at the time of the interview, although this variable did not influence HRQOL. This finding has also been observed in adult AIH populations. Therefore, HRQOL may be reduced in patients in remission as well as in patients who are starting treatment. These findings support the view that HRQOL is an individual and subjective measure that should be considered in each patient's individualized treatment.9,22
A previous history of complications did not influence the HRQOL of AIH children or adolescents. Parental reports revealed poorer HRQOL scores in only the physical domain, a finding that differs from a previous report that suggests that all domains (except the social domain) were jeopardized.10 Furthermore, the parental evaluation of HRQOL differs from that of the patients, in whom almost all domains are reduced. Perhaps parents confound children's emotional symptoms with physical symptoms, and misinterpret sadness as physical pain. It is possible that the cultural and socioeconomic differences between the present sample of parents and the sample in the previous study led to this discrepancy in findings, although the instrument has been validated for local cultural and socioeconomic status.
Chronic conditions in the pediatric population decrease HRQOL, especially conditions with severe physical pain or those that require more aggressive treatments.27 Although AIH does not exhibit these characteristics and often responds well to treatment, the present results show a significantly reduced HRQOL in all domains except social for AIH patients compared to healthy controls.10,28 For AIH patients, the treatment of any physical symptoms that may occur does not eliminate the chronic condition in childhood and adolescence, and the alleviation of physical symptoms does not necessarily imply a better HRQOL. Although all tested domains are related to each other, i.e., emotional distress should affect the physical domain, the physical and school domains must be further investigated, as AIH does not lead to significant physical symptoms or cognitive decline. It is possible that school absences caused by regular follow-up appointments, which are necessary for medical examinations, may jeopardize school performance.
Notably, previous research indicates that children are able to demonstrate their own feelings and complaints with a reliable evaluation of their own HRQOL.29 Thus, specific instruments to measure HRQOL in several diseases in children and adolescents are being developed, and further studies that evaluate new and specific tools to assess HRQOL in AIH patients will be necessary.
In conclusion, reduced scores in physical, emotional, and school domains were observed in pediatric AIH patients. Abdominal pain and corticosteroid dose negatively influenced the HRQOL in children and adolescents with AIH. Disease severity and disease remission status did not influence the HRQOL in the AIH pediatric population.
Finally, the present results highlight the urgency of providing attention to the physical, school, and emotional symptoms of AIH patients and to the development of a specific HRQOL measurement instrument for AIH children and adolescents.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would thank Drs. James W. Varni, Claudio A. Len, and Denise A. Klatchoian for providing the Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) instrument.
Please cite this article as: Bozzini AB, Neder L, Silva CA, Porta G. Decreased health-related quality of life in children and adolescents with autoimmune hepatitis. J Pediatr (Rio J). 2019;95:87–93.




