
To identify factors associated with total sedentary time and screen time in children aged 9–11 years.
MethodsFor seven consecutive days, 328 children (51.5% boys) used accelerometers to monitor total sedentary time. Screen time was calculated by the self-reporting method. Individual, family, family environment, and school environment questionnaires were filled out. Body composition was measured using a Tanita scale.
ResultsThe mean sedentary time was 500min/day (boys: 489, girls: 511, p=0.005), and mean screen time was 234min/day (boys: 246, girls: 222, p=0.053). In both genders, factors associated with sedentary time were healthy dietary pattern and moderate-to-vigorous physical activity. In boys, only moderate-to-vigorous physical activity was significant; in girls, the healthy dietary pattern, moderate-to-vigorous physical activity, and transportation to school were significant. As for the screen time, the associated factors were body mass index and healthy dietary pattern (both genders). In boys, the associated factors were body mass index, healthy dietary pattern, and television in the bedroom. In girls, the associated factors were healthy dietary pattern, transportation to school, and physical activity policies or practice at school.
ConclusionSeveral associated factors were identified in the association between total sedentary time and screen time in children; however, only the healthy dietary pattern was common between sedentary time and screen time.
Identificar os fatores associados do tempo sedentário total e tempo de tela em crianças entre 9-11 anos.
MétodosDurante sete dias consecutivos, 328 crianças (51,5% meninos) usaram acelerômetros para monitorar o tempo sedentário total. O tempo de tela foi calculado pelo método autorreferido. Questionários com fatores individuais, familiares, ambiente familiar e escolar foram preenchidos. A composição corporal foi medida usando uma balança Tanita.
ResultadosA média do tempo sedentário (min/dia) foi de 500 (meninos: 489; meninas: 511; p=0,005), e do tempo de tela foi 234 (meninos: 246; meninas: 222; p=0,053). Em ambos os sexos, os fatores associados do tempo sedentário foram o padrão de dieta saudável e atividade física de moderada a vigorosa. Nos meninos, apenas a atividade física de moderada a vigorosa foi significativa e nas meninas o padrão de dieta saudável, atividade física de moderada a vigorosa e transporte para a escola foi significativo. Já para o tempo de tela, os fatores associados foram o índice de massa corporal e padrão de dieta saudável (ambos os sexos). Nos meninos, os fatores associados foram o índice de massa corporal, o padrão de dieta saudável e televisão no quarto. Nas meninas, os fatores associados foram o padrão de dieta saudável, transporte para escola e políticas ou práticas de atividade física na escola.
ConclusãoVários fatores associados foram identificados entre tempo sedentário total e tempo de tela em crianças. Entretanto, somente o padrão de dieta saudável foi comum entre tempo sedentário e tempo de tela.
Sedentary time (ST) is characterized by behaviors that require little energy expenditure and that occurs in a sitting or lying position.1 Many daily activities involve ST, which can also be classified by a variety of sedentary behaviors (SBs), such as reading, working, and watching television (TV), for instance.2 ST should be seen as separate and distinct behavior from physical activity and not simply as failure to comply with physical activity guidelines.3 The amount of time spent by children on SBs should be minimized, and screen time (ScT), sedentary transportation (i.e., motorized), and prolonged time spent in the sitting position should be limited.4
ST has been extensively assessed through questionnaires that focus primarily on specific SBs, such as ScT, rather than total ST. Children with lower ScT have better physical activity measures5 and lower risks to obesity6 than those with higher ScT. In turn, accelerometers can evaluate the overall ST, including its effect on health conditions. In adults, higher total ST is associated with an increased risk of cardiovascular disease.7 However, in children, the association between total ST measured by accelerometers and health problems is less evident, and possibly more complex. For instance, a high total ST is not associated with body composition.8 Additionally, Biddle et al.9 showed that ScT represents only a small proportion of total ST. In a systematic review, 64 studies assessing factors associated with SB were retrieved; however, only 11 used accelerometers to objectively measure total ST and self-reported ScT and none of these were carried out with Brazilian children.10 The 11 studies found a significant association with age, gender, ethnicity, socioeconomic level (SEL), and physical activity in children, especially in high-income countries. Studies that use objective measures of ST in children from low- and middle-income countries, such as Brazil, are necessary to investigate the associated factors in several domains of these behaviors. This study aimed to identify the factors associated with total ST and ScT in children aged 9–11 years.
Material and methodsStudy sampleThis was a cross-sectional multicenter study carried out in 12 countries, and is part of the International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE),11 whose details have been previously published.11
The present study focuses on data collected from the ISCOLE Brasil study, which was carried out in the city of São Caetano do Sul, state of São Paulo, Brazil. In 2013, the municipality had 149,263 inhabitants, of whom 1557 were children (812 boys) aged 10 years.12
After the project was approved by the Secretariat of Education, it was presented at each school and to the parents’ council. After the authorizations were obtained, the project was implemented at each school. All fifth-grade children were invited to participate in the study.
Due to the SEL variability between public and private schools, the type of school (public vs. private) was considered as an indicator of SEL. Two complete lists of public and private schools attended by fifth-grade students were generated. Schools were separately selected from each list, considering a ratio of four (public) to one (private). Twenty schools (16 public) were selected to obtain a sample of 25–30 children from each school, with a target recruitment of 500 children aged 9–11 years, according to the sample calculation.11
Data collection was performed between March 2012 and April 2013, and all evaluations were carried out during an entire week per school. All data collection and management activities were performed and monitored according to quality control procedures, implemented by the ISCOLE coordinating center.11
In total, 564 children (277 boys) were assessed and met the inclusion criteria. Considering the exclusion criteria, the final sample included 328 children (169 boys).13 The study was approved by the Research Ethics Committee of Universidade Federal de São Paulo.
AccelerometryThe Actigraph GT3X accelerometer (ActiGraph®, USA) was used to objectively monitor total ST and moderate-to-vigorous physical activity (MVPA). The accelerometer was used at the waist, attached to an elastic belt, in the middle axillary line on the right side. Participants were encouraged to use the accelerometer 24-h/day for at least seven days, including the weekend.
The minimum amount of accelerometer data that was considered acceptable for analysis was four days, with at least 10h/day of use, after its removal at sleep time.14,15 Blocks of 20 consecutive minutes of zero count were considered as not using the device, and were discarded from the analyses.
The research team went to schools to retrieve the accelerometers and check whether the data were complete using the Actilife software (ActiGraph's, premier actigraphy data analysis software, version 5.6, USA). Data were collected at a sampling rate of 80Hz, downloaded in periods of 1s, and aggregated for periods of 15s.16 A cut-off point of ≤25counts/15s was used for total ST and ≥574counts/15s for MVPA.16 For the analyses, total ST was considered as a continuous variable.
Self-reported ScTChildren reported ScT through the Diet and Lifestyle Questionnaire.11 They were asked how many hours they spent watching TV and how many hours they spent playing video and/or computer games on weekdays and weekends11 and the answers were: I do not watch TV, <1, 1, 2, 3, 4, and ≥5h. The mean daily ScT score was calculated as follows: ([TV hours on weekdays×5]+[TV hours on weekends×2]+[hours of video and computer games on weekdays×5]+[hours of video and computer games on weekends×2])/7. The self-reported ScT has been previously validated in children.17
Anthropometric factorsThe data were collected by professionals during the school visit according to standardized procedures.11 Height was measured with a 0.1-cm precision using a Seca 213 portable stadiometer (Seca®, Hamburg, Germany). Body weight and body fat percentage (BF%) were measured using a Tanita SC-240 portable body composition analyzer (Tanita®, Arlington Heights, IL, USA) without shoes, socks, or heavy items in their pockets.18 Two measurements were obtained, and the mean value was used in the analysis.
Body mass index (BMI; kg/m2) was calculated based on height and body weight; subsequently, the Z-score was calculated based on the World Health Organization growth reference charts. The children were classified as: underweight: <−2 SD; normal weight: −2 SD to 1 SD; excess weight >+1 SD to 2 SD; and obese: >+2 SD.19 Waist circumference (WC) measurements were made on the exposed skin at the end of a normal expiration using a non-elastic anthropometric tape between the lower rib margin and the iliac crest.11
QuestionnairesThe Diet and Lifestyle Questionnaire, with information related to food consumption, physical activity, SBs, breakfast consumption, transportation to school, and sleep, was filled out by the children. The Demographic and Family Health Questionnaire, with information about parents’ educational level, family income, and number of automobiles, was answered by parents or guardians. It also included questions about the children's age, gender, number of siblings, and ethnicity. The Neighborhood Questionnaire was used to obtain information about the parents’ or caregivers’ perceptions regarding the social environment, dietary habits, and number of TV sets. The School Environment Questionnaire, with information on the school characteristics, policies or practices that may influence healthy eating habits, and physical activity practice, was filled out by a school administrator. Details have been previously published.11
Statistical analysisA descriptive analysis, including means, standard deviation, frequency, and percentage (%), the Kolmogorov–Smirnov test, and Student's t-test for independent samples were calculated.
A multilevel linear regression analysis was used, including school as a random effect, to analyze the associations between associated factors and total ST and ScT. First, all associated factors were used in the univariate models. Type of school (public and private), gender, ethnicity, and school (to allow grouping at the school level) were included as covariates in the univariate models. The variables with p<0.10 were included in specific models in accordance with the ecological model.2 At a second moment, the factors associated with total ST and ScT with p<0.10 in the specific models were included in the final model. In the final model, p<0.05 was used to consider the variables as factors associated with total ST and ScT. School, gender, ethnicity, number of siblings, and total annual family income were used as covariates in the multivariate models.
Multicollinearity was tested through correlation, tolerance and variance inflation factor (VIF). VIF values higher than 5 were considered AS indicators of problems in estimating the coefficient due to multicollinearity between the independent variables.20 To compare the models, the Akaike information criterion (AIC) and the Bayesian information criterion (BIC) were utilized. The analyses were performed using SPSS, version 20.0.
ResultsThe samples of girls (n=159) and boys (n=169) from 20 schools allowed the detection of elevated effects with a statistical power of more than 90% in the models used.21 Details on the questionnaires, associated factors, descriptive analysis, and information on the sample that did not meet the inclusion and exclusion criteria have been previously provided.13 Of the 328 children (mean age: 10.4 years) who participated in the study and had complete data, 51.5% were boys, and 75.9% were classified as white/Caucasian ethnicity.
The mean total ST was 500.06 (69.0)min/day. In boys, the mean was 489.67 (69.2) and in the girls, 511.11 (67.3)min/day (p=0.005). Regarding ScT, the mean was 234 (126)min/day, 246 (132) in boys and 222 (126) in girls (p=0.053), respectively. Only 22.6% of the children met the ScT guidelines (≤2h/day),4 being 18.9% boys and 26.4% girls (p=0.105).
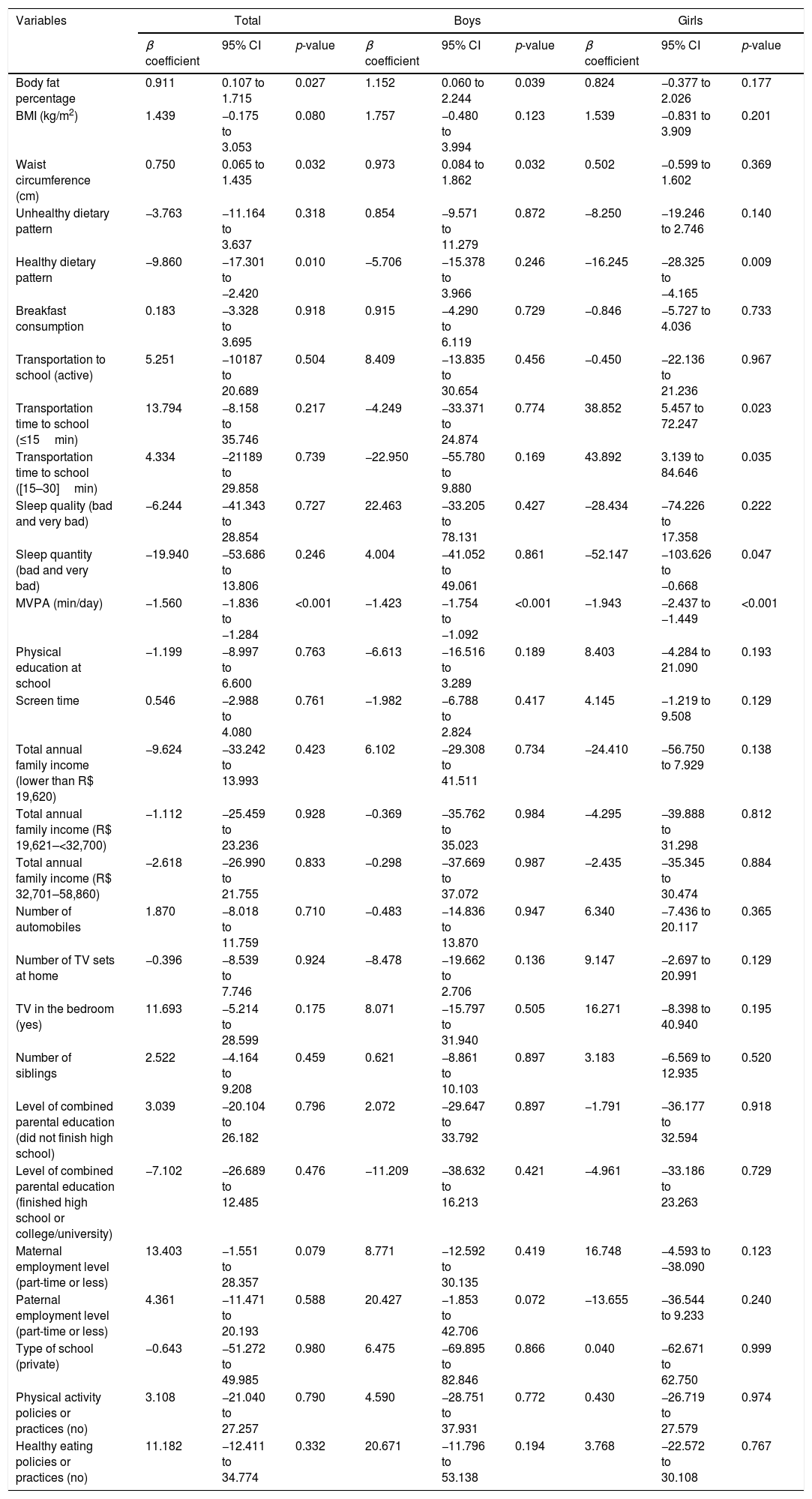
When considering both genders, a positive association was observed between total ST with BF%, BMI, and WC. The association was negative with healthy dietary pattern and MVPA. There was also a significant association with the level of maternal employment.
In boys, total ST was positively associated with BF% and WC, and negatively associated with MVPA and the level of paternal employment. Regarding the girls, a significant and negative association was observed with a healthy dietary pattern, amount of sleep, and with MVPA. A positive association was found between transportation time to school with total ST in girls (Table 1).
Univariate models of the associated factors of total sedentary time in children from São Caetano do Sul, Brazil.a
| Variables | Total | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | |
| Body fat percentage | 0.911 | 0.107 to 1.715 | 0.027 | 1.152 | 0.060 to 2.244 | 0.039 | 0.824 | −0.377 to 2.026 | 0.177 |
| BMI (kg/m2) | 1.439 | −0.175 to 3.053 | 0.080 | 1.757 | −0.480 to 3.994 | 0.123 | 1.539 | −0.831 to 3.909 | 0.201 |
| Waist circumference (cm) | 0.750 | 0.065 to 1.435 | 0.032 | 0.973 | 0.084 to 1.862 | 0.032 | 0.502 | −0.599 to 1.602 | 0.369 |
| Unhealthy dietary pattern | −3.763 | −11.164 to 3.637 | 0.318 | 0.854 | −9.571 to 11.279 | 0.872 | −8.250 | −19.246 to 2.746 | 0.140 |
| Healthy dietary pattern | −9.860 | −17.301 to −2.420 | 0.010 | −5.706 | −15.378 to 3.966 | 0.246 | −16.245 | −28.325 to −4.165 | 0.009 |
| Breakfast consumption | 0.183 | −3.328 to 3.695 | 0.918 | 0.915 | −4.290 to 6.119 | 0.729 | −0.846 | −5.727 to 4.036 | 0.733 |
| Transportation to school (active) | 5.251 | −10187 to 20.689 | 0.504 | 8.409 | −13.835 to 30.654 | 0.456 | −0.450 | −22.136 to 21.236 | 0.967 |
| Transportation time to school (≤15min) | 13.794 | −8.158 to 35.746 | 0.217 | −4.249 | −33.371 to 24.874 | 0.774 | 38.852 | 5.457 to 72.247 | 0.023 |
| Transportation time to school ([15–30]min) | 4.334 | −21189 to 29.858 | 0.739 | −22.950 | −55.780 to 9.880 | 0.169 | 43.892 | 3.139 to 84.646 | 0.035 |
| Sleep quality (bad and very bad) | −6.244 | −41.343 to 28.854 | 0.727 | 22.463 | −33.205 to 78.131 | 0.427 | −28.434 | −74.226 to 17.358 | 0.222 |
| Sleep quantity (bad and very bad) | −19.940 | −53.686 to 13.806 | 0.246 | 4.004 | −41.052 to 49.061 | 0.861 | −52.147 | −103.626 to −0.668 | 0.047 |
| MVPA (min/day) | −1.560 | −1.836 to −1.284 | <0.001 | −1.423 | −1.754 to −1.092 | <0.001 | −1.943 | −2.437 to −1.449 | <0.001 |
| Physical education at school | −1.199 | −8.997 to 6.600 | 0.763 | −6.613 | −16.516 to 3.289 | 0.189 | 8.403 | −4.284 to 21.090 | 0.193 |
| Screen time | 0.546 | −2.988 to 4.080 | 0.761 | −1.982 | −6.788 to 2.824 | 0.417 | 4.145 | −1.219 to 9.508 | 0.129 |
| Total annual family income (lower than R$ 19,620) | −9.624 | −33.242 to 13.993 | 0.423 | 6.102 | −29.308 to 41.511 | 0.734 | −24.410 | −56.750 to 7.929 | 0.138 |
| Total annual family income (R$ 19,621–<32,700) | −1.112 | −25.459 to 23.236 | 0.928 | −0.369 | −35.762 to 35.023 | 0.984 | −4.295 | −39.888 to 31.298 | 0.812 |
| Total annual family income (R$ 32,701–58,860) | −2.618 | −26.990 to 21.755 | 0.833 | −0.298 | −37.669 to 37.072 | 0.987 | −2.435 | −35.345 to 30.474 | 0.884 |
| Number of automobiles | 1.870 | −8.018 to 11.759 | 0.710 | −0.483 | −14.836 to 13.870 | 0.947 | 6.340 | −7.436 to 20.117 | 0.365 |
| Number of TV sets at home | −0.396 | −8.539 to 7.746 | 0.924 | −8.478 | −19.662 to 2.706 | 0.136 | 9.147 | −2.697 to 20.991 | 0.129 |
| TV in the bedroom (yes) | 11.693 | −5.214 to 28.599 | 0.175 | 8.071 | −15.797 to 31.940 | 0.505 | 16.271 | −8.398 to 40.940 | 0.195 |
| Number of siblings | 2.522 | −4.164 to 9.208 | 0.459 | 0.621 | −8.861 to 10.103 | 0.897 | 3.183 | −6.569 to 12.935 | 0.520 |
| Level of combined parental education (did not finish high school) | 3.039 | −20.104 to 26.182 | 0.796 | 2.072 | −29.647 to 33.792 | 0.897 | −1.791 | −36.177 to 32.594 | 0.918 |
| Level of combined parental education (finished high school or college/university) | −7.102 | −26.689 to 12.485 | 0.476 | −11.209 | −38.632 to 16.213 | 0.421 | −4.961 | −33.186 to 23.263 | 0.729 |
| Maternal employment level (part-time or less) | 13.403 | −1.551 to 28.357 | 0.079 | 8.771 | −12.592 to 30.135 | 0.419 | 16.748 | −4.593 to −38.090 | 0.123 |
| Paternal employment level (part-time or less) | 4.361 | −11.471 to 20.193 | 0.588 | 20.427 | −1.853 to 42.706 | 0.072 | −13.655 | −36.544 to 9.233 | 0.240 |
| Type of school (private) | −0.643 | −51.272 to 49.985 | 0.980 | 6.475 | −69.895 to 82.846 | 0.866 | 0.040 | −62.671 to 62.750 | 0.999 |
| Physical activity policies or practices (no) | 3.108 | −21.040 to 27.257 | 0.790 | 4.590 | −28.751 to 37.931 | 0.772 | 0.430 | −26.719 to 27.579 | 0.974 |
| Healthy eating policies or practices (no) | 11.182 | −12.411 to 34.774 | 0.332 | 20.671 | −11.796 to 53.138 | 0.194 | 3.768 | −22.572 to 30.108 | 0.767 |
95% CI, 95% confidence interval; BMI, body mass index; MVPA, moderate-to-vigorous physical activity; TV, television.
Reference categories of categorical variables: transportation to school: inactive; transportation time to school: >30min; quality and quantity of sleep: good and very good; total annual family income: R$ 58,861 and above; TV in the room: no; level of combined parental education: specialization; maternal and paternal employment level: full time; type of school: public; physical activity or healthy eating policies or practices: yes.
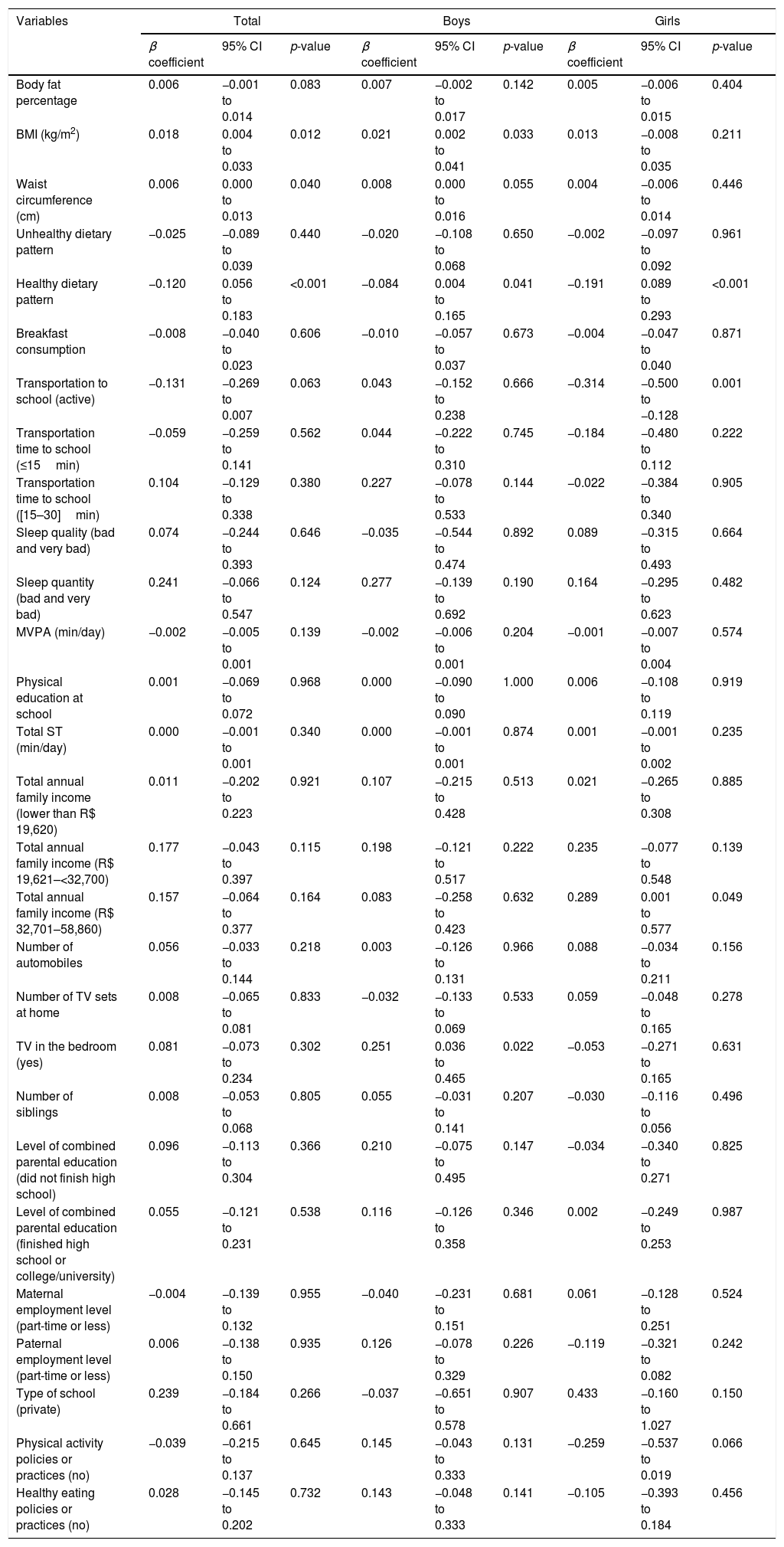
Considering both genders, ScT was positively associated with BMI and WC. A negative association was observed with healthy dietary pattern and transportation to school. In boys, the variables significantly associated with ScT were BMI, WC, healthy dietary pattern, and TV in the bedroom. All associations were positive, except for the healthy dietary pattern. As for the girls, the variables with a significant and negative association with ScT were healthy dietary pattern, transportation to school, and existence of physical activity policies or practices. A positive and significant association was also observed with total annual income (Table 2).
Univariate models of screen time associated factors in children from São Caetano do Sul, Brazil.a
| Variables | Total | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | |
| Body fat percentage | 0.006 | −0.001 to 0.014 | 0.083 | 0.007 | −0.002 to 0.017 | 0.142 | 0.005 | −0.006 to 0.015 | 0.404 |
| BMI (kg/m2) | 0.018 | 0.004 to 0.033 | 0.012 | 0.021 | 0.002 to 0.041 | 0.033 | 0.013 | −0.008 to 0.035 | 0.211 |
| Waist circumference (cm) | 0.006 | 0.000 to 0.013 | 0.040 | 0.008 | 0.000 to 0.016 | 0.055 | 0.004 | −0.006 to 0.014 | 0.446 |
| Unhealthy dietary pattern | −0.025 | −0.089 to 0.039 | 0.440 | −0.020 | −0.108 to 0.068 | 0.650 | −0.002 | −0.097 to 0.092 | 0.961 |
| Healthy dietary pattern | −0.120 | 0.056 to 0.183 | <0.001 | −0.084 | 0.004 to 0.165 | 0.041 | −0.191 | 0.089 to 0.293 | <0.001 |
| Breakfast consumption | −0.008 | −0.040 to 0.023 | 0.606 | −0.010 | −0.057 to 0.037 | 0.673 | −0.004 | −0.047 to 0.040 | 0.871 |
| Transportation to school (active) | −0.131 | −0.269 to 0.007 | 0.063 | 0.043 | −0.152 to 0.238 | 0.666 | −0.314 | −0.500 to −0.128 | 0.001 |
| Transportation time to school (≤15min) | −0.059 | −0.259 to 0.141 | 0.562 | 0.044 | −0.222 to 0.310 | 0.745 | −0.184 | −0.480 to 0.112 | 0.222 |
| Transportation time to school ([15–30]min) | 0.104 | −0.129 to 0.338 | 0.380 | 0.227 | −0.078 to 0.533 | 0.144 | −0.022 | −0.384 to 0.340 | 0.905 |
| Sleep quality (bad and very bad) | 0.074 | −0.244 to 0.393 | 0.646 | −0.035 | −0.544 to 0.474 | 0.892 | 0.089 | −0.315 to 0.493 | 0.664 |
| Sleep quantity (bad and very bad) | 0.241 | −0.066 to 0.547 | 0.124 | 0.277 | −0.139 to 0.692 | 0.190 | 0.164 | −0.295 to 0.623 | 0.482 |
| MVPA (min/day) | −0.002 | −0.005 to 0.001 | 0.139 | −0.002 | −0.006 to 0.001 | 0.204 | −0.001 | −0.007 to 0.004 | 0.574 |
| Physical education at school | 0.001 | −0.069 to 0.072 | 0.968 | 0.000 | −0.090 to 0.090 | 1.000 | 0.006 | −0.108 to 0.119 | 0.919 |
| Total ST (min/day) | 0.000 | −0.001 to 0.001 | 0.340 | 0.000 | −0.001 to 0.001 | 0.874 | 0.001 | −0.001 to 0.002 | 0.235 |
| Total annual family income (lower than R$ 19,620) | 0.011 | −0.202 to 0.223 | 0.921 | 0.107 | −0.215 to 0.428 | 0.513 | 0.021 | −0.265 to 0.308 | 0.885 |
| Total annual family income (R$ 19,621–<32,700) | 0.177 | −0.043 to 0.397 | 0.115 | 0.198 | −0.121 to 0.517 | 0.222 | 0.235 | −0.077 to 0.548 | 0.139 |
| Total annual family income (R$ 32,701–58,860) | 0.157 | −0.064 to 0.377 | 0.164 | 0.083 | −0.258 to 0.423 | 0.632 | 0.289 | 0.001 to 0.577 | 0.049 |
| Number of automobiles | 0.056 | −0.033 to 0.144 | 0.218 | 0.003 | −0.126 to 0.131 | 0.966 | 0.088 | −0.034 to 0.211 | 0.156 |
| Number of TV sets at home | 0.008 | −0.065 to 0.081 | 0.833 | −0.032 | −0.133 to 0.069 | 0.533 | 0.059 | −0.048 to 0.165 | 0.278 |
| TV in the bedroom (yes) | 0.081 | −0.073 to 0.234 | 0.302 | 0.251 | 0.036 to 0.465 | 0.022 | −0.053 | −0.271 to 0.165 | 0.631 |
| Number of siblings | 0.008 | −0.053 to 0.068 | 0.805 | 0.055 | −0.031 to 0.141 | 0.207 | −0.030 | −0.116 to 0.056 | 0.496 |
| Level of combined parental education (did not finish high school) | 0.096 | −0.113 to 0.304 | 0.366 | 0.210 | −0.075 to 0.495 | 0.147 | −0.034 | −0.340 to 0.271 | 0.825 |
| Level of combined parental education (finished high school or college/university) | 0.055 | −0.121 to 0.231 | 0.538 | 0.116 | −0.126 to 0.358 | 0.346 | 0.002 | −0.249 to 0.253 | 0.987 |
| Maternal employment level (part-time or less) | −0.004 | −0.139 to 0.132 | 0.955 | −0.040 | −0.231 to 0.151 | 0.681 | 0.061 | −0.128 to 0.251 | 0.524 |
| Paternal employment level (part-time or less) | 0.006 | −0.138 to 0.150 | 0.935 | 0.126 | −0.078 to 0.329 | 0.226 | −0.119 | −0.321 to 0.082 | 0.242 |
| Type of school (private) | 0.239 | −0.184 to 0.661 | 0.266 | −0.037 | −0.651 to 0.578 | 0.907 | 0.433 | −0.160 to 1.027 | 0.150 |
| Physical activity policies or practices (no) | −0.039 | −0.215 to 0.137 | 0.645 | 0.145 | −0.043 to 0.333 | 0.131 | −0.259 | −0.537 to 0.019 | 0.066 |
| Healthy eating policies or practices (no) | 0.028 | −0.145 to 0.202 | 0.732 | 0.143 | −0.048 to 0.333 | 0.141 | −0.105 | −0.393 to 0.184 | 0.456 |
95% CI, 95% confidence interval; BMI, body mass index; MVPA, moderate-to-vigorous physical activity; ST, sedentary time; TV, television.
Reference categories of categorical variables: transportation to school: inactive; transportation time to school: >30min; quality and quantity of sleep: good and very good; total annual family income: R$ 58,861 and above; TV in the bedroom: no; level of combined parental education: specialization; maternal and paternal employment level: full time; type of school: public; physical activity or healthy eating policies or practices: yes.
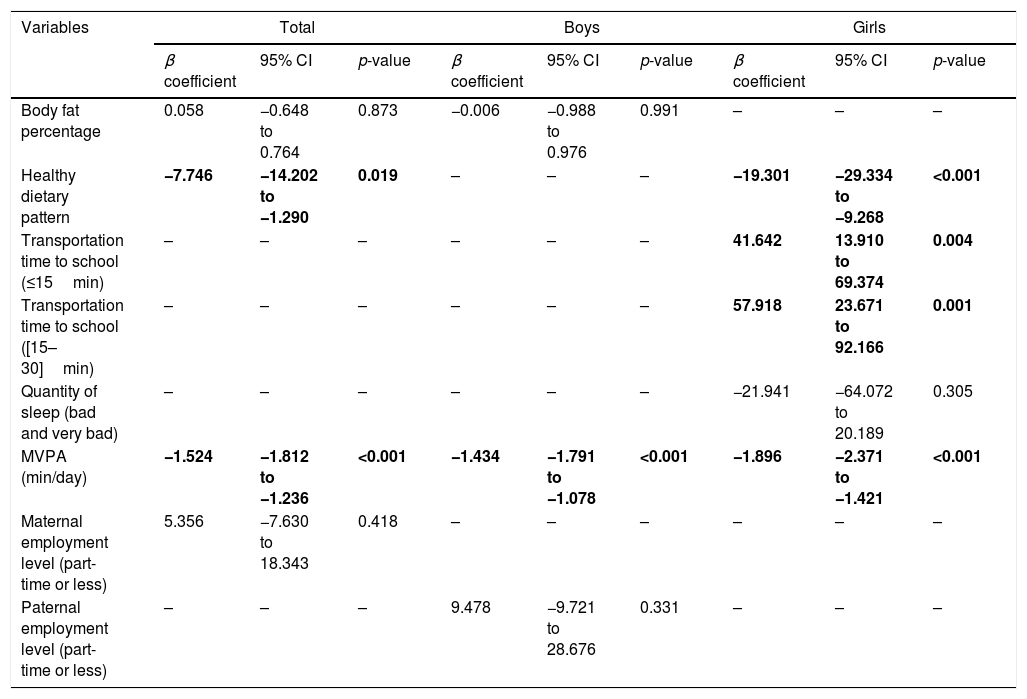
In the multivariate models of total ST, multicollinearity problems between the BF%, BMI, and WC variables were observed. Models were tested with each of the variables, together with the others defined from the univariate models. The WC variable was led to a better-fit model and was therefore included in the multivariate models (Table 3).
Final model (multivariate) of the factors associated with total sedentary time in children from São Caetano do Sul, Brazil.a
| Variables | Total | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | |
| Body fat percentage | 0.058 | −0.648 to 0.764 | 0.873 | −0.006 | −0.988 to 0.976 | 0.991 | – | – | – |
| Healthy dietary pattern | −7.746 | −14.202 to −1.290 | 0.019 | – | – | – | −19.301 | −29.334 to −9.268 | <0.001 |
| Transportation time to school (≤15min) | – | – | – | – | – | – | 41.642 | 13.910 to 69.374 | 0.004 |
| Transportation time to school ([15–30]min) | – | – | – | – | – | – | 57.918 | 23.671 to 92.166 | 0.001 |
| Quantity of sleep (bad and very bad) | – | – | – | – | – | – | −21.941 | −64.072 to 20.189 | 0.305 |
| MVPA (min/day) | −1.524 | −1.812 to −1.236 | <0.001 | −1.434 | −1.791 to −1.078 | <0.001 | −1.896 | −2.371 to −1.421 | <0.001 |
| Maternal employment level (part-time or less) | 5.356 | −7.630 to 18.343 | 0.418 | – | – | – | – | – | – |
| Paternal employment level (part-time or less) | – | – | – | 9.478 | −9.721 to 28.676 | 0.331 | – | – | – |
95% CI, 95% confidence interval; MVPA, moderate-to-vigorous physical activity.
Note: Data in bold indicate significance (p<0.05).
Reference categories of categorical variables: transportation time to school: >30min; quantity of sleep: good and very good; maternal and paternal employment level: full time; type of school: public.
Considering the total sample, the associated significant and negative factors were healthy dietary pattern and MVPA. In boys, only the association with MVPA was significant. In girls, the association was negative with healthy dietary pattern and MVPA and positive with transportation time (Table 3).
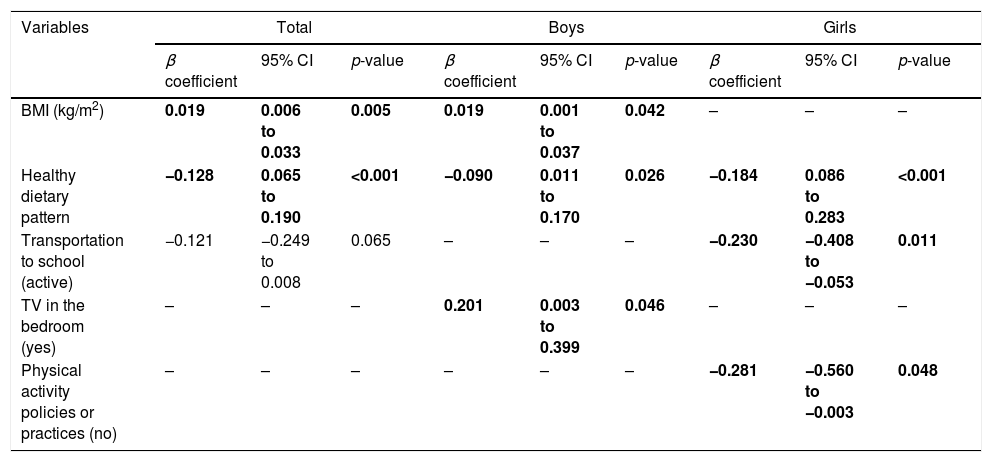
In multivariate ScT models, multicollinearity problems between BMI and WC were also observed. The BMI was the variable that showed a better-fit model, and was therefore included in the multivariate models (Table 4).
Final model (multivariate) of the factors associated with screen time in children from São Caetano do Sul, Brazil.a
| Variables | Total | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | β coefficient | 95% CI | p-value | |
| BMI (kg/m2) | 0.019 | 0.006 to 0.033 | 0.005 | 0.019 | 0.001 to 0.037 | 0.042 | – | – | – |
| Healthy dietary pattern | −0.128 | 0.065 to 0.190 | <0.001 | −0.090 | 0.011 to 0.170 | 0.026 | −0.184 | 0.086 to 0.283 | <0.001 |
| Transportation to school (active) | −0.121 | −0.249 to 0.008 | 0.065 | – | – | – | −0.230 | −0.408 to −0.053 | 0.011 |
| TV in the bedroom (yes) | – | – | – | 0.201 | 0.003 to 0.399 | 0.046 | – | – | – |
| Physical activity policies or practices (no) | – | – | – | – | – | – | −0.281 | −0.560 to −0.003 | 0.048 |
95% CI, 95% confidence interval; BMI, body mass index; TV, television.
Note: Data in bold indicate significance (p<0.05).
Reference categories of categorical variables: transportation to school: inactive; TV in the bedroom: no; physical activity policies and practice: yes.
Considering the entire sample, the factors significantly associated with ScT were BMI (positive association) and healthy dietary pattern (negative association). In boys, these factors were also BMI and healthy dietary pattern. In addition to these, TV in the bedroom showed a significant effect on ScT in boys. In girls, the significant associated factors were healthy dietary pattern, type of school transportation, and physical activity policies or practices (Table 4).
DiscussionThe healthy dietary pattern was the only common factor associated with total ST and ScT in both genders. Regarding total ST, the associated factors were healthy dietary pattern and MVPA, in both genders. In boys, only MVPA was significant. In the girls, the association was negative with healthy dietary pattern and MVPA, and positive with transportation time. Regarding ScT, BMI and healthy dietary pattern showed significant results in both genders together and in boys. A positive association was also observed with TV in the bedroom, in boys. In girls, the associated factors were healthy dietary pattern, type of transportation to school, and physical activity policies or practices.
Herman et al.22 concluded that higher levels of total ST measured by accelerometry were associated with higher BF% levels, being determinant for weight gain and disease risk.7 Herman et al.22 reported a positive association between total ST and BMI in Canadian children. However, the authors found that total ST was not associated with BF%.
Results reported by LeBlanc et al.23 showed that healthy dietary pattern is a predictor of ScT. These authors did not find significant results between total ST and the healthy dietary pattern.
The present study showed a significant association between the healthy dietary pattern score and total ST, which may be partly due to the increase in energy intake, mainly through the consumption of energy-dense foods.24 Boys and girls who reported high levels of reading or doing homework consumed significantly less energy than those who reported low levels of reading or doing homework.25 Corroborating a previously published study,25 the present study has shown that lower healthy dietary pattern scores are associated with ScT in both genders together and only in girls. A previous study by Utter et al.25 showed that girls and boys who reported higher ScT consumed 300–400calories/day more than those who reported lower ScT. Although the authors are unable to discuss the amount (i.e., the number of calories) of energy consumption, the association of ScT with consumption of energy-rich foods such as soda, fried foods, and healthy snacks is consistent with the current results, as well as other studies using the ISCOLE dataset.23
The present study found evidence of an association between transportation to school (time and type) with total ST. A study of 9- to 11-year-old children from ISCOLE-participating countries did not identify an association between active transportation to school and total ST.26 In turn, children who engage in active transportation to school and live within a 1–2km radius of school accumulate less time in SBs than those who live closer to school.27
Children with high levels of adiposity28 and low level of physical activity29 have electronic equipment in the bedroom. The present results show a positive association between TV in the bedroom with ScT in boys. The present study showed no association between TV in the bedroom and total ST. Atkin et al.30 verified that the presence of TV in the bedroom was not associated with total ST, but was associated with ScT. Watching TV, for instance, can be an overall indicator of a sedentary lifestyle,9 and may be only an indicator of total SB time.22
This study has some strengths and limitations. Accelerometers are valid tools used to measure different intensities of physical activity and total ST in children.14 However, it is well established that the monitor placed on the hip is less effective in differentiating sedentary positions, such as lying down or sitting. Moreover, they cannot accurately assess activities performed with the trunk. Some factors associated with total ST and ScT were based on reports. It is also possible that these associated factors are exclusive to the children of the municipality, due to the sample's non-representativeness. Caution should be exercised when generalizing the results to other populations. Even though the study involved 20 schools, it does not provide a representative national sample. Causality cannot be determined from cross-sectional data.
This study assessed a broad variety of factors associated with total ST and ScT in children from São Caetano do Sul. The only common factor associated with both ST and ScT was healthy dietary pattern. For the total ST, the associated factors found were healthy dietary pattern and MVPA, in both genders. In boys, only MVPA was associated. In girls, the healthy dietary pattern, MVPA and time of school transportation were considered associated factors.
As for ScT, BMI and healthy dietary pattern were considered associated factors in both genders together and only in boys. Among the boys, TV in the bedroom was also considered an associated factor. In girls, the associated factors were healthy dietary pattern, type of school transportation, and physical activity policies or practices. These results should be used by professionals who aim to implement interventions to reduce SBs in children. The use of longitudinal and experimental data is essential for further advances in this field and should be complemented by the development of ecological models.2
FundingThe ISCOLE Brazil research project was funded by the Coca-Cola Company.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Victor Matsudo, Sandra Matsudo, Timóteo Araújo, Luis Carlos de Oliveira, Leandro Rezende, Luis Fabiano, Diogo Bezerra, and Gerson Ferrari for their contribution to ISCOLE Brazil data collection, and the ISCOLE Coordination Center in Baton Rouge, Louisiana, United States.
The authors would like to thank the participants, the children's parents and/or guardians, teachers, and coordinators of the Municipal Secretariat of Education of São Caetano do Sul and the Municipality of São Caetano do Sul.
Please cite this article as: Ferrari GL, Pires C, Solé D, Matsudo V, Katzmarzyk PT, Fisberg M. Factors associated with objectively measured total sedentary time and screen time in children aged 9–11 years. J Pediatr (Rio J). 2019;95:94–105.





