


The potential role of procalcitonin (PCT) in the diagnosis of catheter-related bloodstream infection (CRBSIs) is still unclear and requires further research. The diagnostic value of serum PCT for the diagnosis of CRBSI in children is evaluated here.
MethodThis study was conducted between October 2013 and November 2014, and included patients with suspected CRBSI from 1 month to 18 years of age who were febrile, with no focus of infection, and had a central venous catheter. Levels of PCT and other serum markers were measured, and their utility as CRBSI markers was assessed. Additionally, the clinical performance of a new, automated, rapid, and quantitative assay for the detection of PCT was tested.
ResultsAmong the 49 patients, 24 were diagnosed with CRBSI. The PCT-Kryptor and PCT-RTA values were significantly higher in proven CRBSI compared to those in unproven CRBSI (p=0.03 and p=0.03, respectively). There were no differences in white blood cell count and C-reactive protein (CRP) levels between proven CRBSI and unproven CRBSI. Among the 24 patients with CRBSI, CRP was significantly higher among those with Gram-negative bacterial infection than in those with Gram-positive bacterial infections. PCT-Kryptor was also significantly higher among patients with Gram-negative bacterial infection than in those with Gram-positive bacterial infections (p=0.01 and p=0.02, respectively).
ConclusionsThe authors suggest that PCT could be a helpful rapid diagnostic marker in children with suspected CRBSIs.
O possível papel da procalcitonina (PCT) no diagnóstico de infecções de corrente sanguínea relacionadas a cateter (ICSRCs) ainda não está claro e precisa ser mais pesquisado. O valor diagnóstico da PCT sérica para o diagnóstico de ICSRC em crianças é avaliado neste estudo.
MétodoEste estudo foi feito entre outubro de 2013 e novembro de 2014 e incluiu pacientes com suspeita de ICSRC de um mês a 18 anos de idade que estavam febris, não tinham foco de infecção e tinham cateter venoso central. Foram medidos os níveis de PCT e de outros marcadores séricos, cuja utilidade como marcadores de ICSRC foi avaliada. Adicionalmente, foi testado o desempenho clínico de um novo ensaio quantitativo automatizado e rápido para a detecção de PCT.
ResultadosDentre 49 pacientes, 24 foram diagnosticados com ICSRC. Os valores de PCT-Kryptor e PCT-RTA foram significativamente maiores em ICSRCs comprovadas do que em ICSRCs não comprovadas (p=0,03 e p=0,03, respectivamente). Não houve diferença na contagem de glóbulos brancos e nos níveis de proteína C reativa (PCR) entre ICSRCs comprovadas e ICSRCs não comprovadas. Dentre os 24 pacientes com ICSRC, a PCR era significativamente maior entre aqueles com infecção bacteriana gram-negativa do que naqueles com infecção bacteriana gram-positiva. O PCT-Kryptor também foi significativamente maior entre pacientes com infecção por bactérias gram-negativas do que naqueles com infecção por bactérias gram-positivas (p=0,01 e p=0,02, respectivamente).
ConclusõesSugerimos que a PCT pode ser um marcador de diagnóstico rápido útil em crianças com suspeita de ICSRCs.
Central venous catheters (CVCs) are generally used to administer intravenous fluids, medications, blood products, and parenteral nutrition fluids, to monitor hemodynamic status, and to provide hemodialysis.1 Catheter-related bloodstream infections (CRBSIs) are the leading cause of nosocomially acquired sepsis including neonatal sepsis,2 and are associated with significant morbidity, mortality, and hospital costs.1,3 Early diagnosis of CRBSIs and appropriate treatment may reduce the associated morbidity and mortality.4,5 The laboratory criteria for diagnosing CRBSIs are precise; however, differences in the definitions and methodologies among various studies have made it difficult to compare the results.1,6 Confirmation of CRBSIs requires the identification of microorganisms recovered from blood and catheter tips. Although blood culture is the best method for the diagnosis of bloodstream infections, test results are not rapidly available. Additionally, only 15–25% of the CVC tips that reach the microbiology laboratory turn out to be culture-positive. Furthermore, not all CRBSIs require the catheter to be withdrawn.7,8 Therefore, the diagnosis of CRBSIs by conservative methods (without catheter withdrawal) appears to be more reasonable in clinical settings to avoid unnecessary removal of the vascular catheter and antibiotic overuse.9
Since the removal of such devices is often a challenge, true CRBSI should be confirmed to distinguish it from contaminated blood cultures, catheter colonization without concomitant bloodstream infection, or fever from another source. Various methods have been previously used to diagnose CRBSI without catheter removal.1 Early and established biomarkers may be useful for diagnosis, prognosis, and monitoring of response to therapy.10 Commonly used biomarkers such as white blood cells (WBCs) or C-reactive protein (CRP) lack adequate specificity for the diagnosis of bacterial infections.9 Serum procalcitonin (PCT), a 116-amino acid polypeptide, has recently emerged as a biomarker for the diagnosis of various bacterial infections. It was found to have a higher diagnostic accuracy when compared with other commonly used laboratory parameters, such as WBC and CRP.11–13 PCT levels are found to be lower in the serum of healthy humans, but are significantly elevated in those suffering from severe infections, particularly sepsis.14,15 To the best of the author's knowledge, only a few studies have assessed the rationale behind PCT levels for the accurate diagnosis of CRBSIs,16,17 especially in children.
Thus, the present study aimed to evaluate the accuracy of PCT for the diagnosis of CRBSIs in children. Furthermore, the clinical performance of a new, automated, and rapid quantitative assay was also examined.
Materials and methodsThis study was conducted between October 2013 and November 2014 on patients with clinical suspicion of CRBSI and eligible for inclusion. Patients who were aged between 1 month and 18 years, febrile, with no focus of infection, and had a central venous catheter were enrolled in the study. The investigation was reviewed and approved by the ethical committee of the Zekai Tahir Burak Maternity Teaching Hospital, Ministry of Health, Ankara, Turkey.
Clinical suspicion of CRBSI was based on the onset of the following features suggestive of infection: (a) clinical manifestations of infection (fever, chills, and/or hypotension); (b) use of central venous catheter for over 48h; and (c) no other apparent source of infection.1 In cased of suspected CRBSI, paired blood samples from the catheter and a peripheral vein were obtained and submitted for culture test.1
According to previously published guidelines, a definitive diagnosis of CRBSI requires either the isolation of the same organism from the peripheral blood culture and the culture of the catheter tip or positive culture from both the catheter hub and blood from peripheral vein, meeting the CRBSI criteria.1,16
Patients with any active infection other than CRBSI or those who showed culture negativity despite the suspicion of CRBSI were excluded from the study (13 patients). If a patient had more than one episode of suspected CRBSI during the study period, only the first episode was included.
For monitoring purposes, patients with proven CRBSI were categorized into two subgroups depending on the infection control: (a) controlled, patients with controlled infection (n=20), defined as clinical and microbiological improvement, and (b) not controlled, patients with uncontrolled infection (n=4), defined as persistent bacteremia (the same pathogen responsible for the first episode was cultured 72h after catheter removal or 72h after initiation of the appropriate treatment), superinfection (CRBSI due to another pathogen during the therapy period), or death related to CRBSI.16 Mortality was defined as related to CRBSI if death occurred within the first 28 days of CRBSI suspicion.
Blood samples were assessed for routine hematology and biochemistry panels, as well as for PCT and CRP levels. PCT levels were determined using Brahms Kryptor® compact immunoassay analyzer (Thermofisher, Hennigsdorf, Germany) and RTA® Procalcitonin device (RTA, Kocaeli, Turkey) simultaneously. Both assays required a minimum of 80μL serum, and tested positive if PCT levels were greater than 0.5ng/mL, according to the manufacturer's instructions. Preferably, fresh serum samples were used for measurements. However, if samples were not used on the same day, they were frozen at −20°C.
Statistical analysisData were analyzed using the SPSS version 19.0 (SPSS, Inc. – Chicago, USA). Descriptive statistics were used to summarize the participants’ baseline characteristics, including means, standard deviations (SDs), medians, and interquartile ranges for continuous variables and frequency distributions for categorical variables. To compare the baseline characteristics according to the occurrence of CRBSI, the χ2 test was used for categorical variables. The normality of quantitative variables was tested by Kolmogorov–Smirnov test. For continuous variables, the independent-groups t test was used for normally distributed variables or the nonparametric Mann–Whitney U test, if the normality assumption was violated. The area under the receiver operating characteristic (ROC) curve was calculated to evaluate the diagnostic and prognostic significance of the tested parameters. Data were expressed as area under ROC curves with 95% confidence intervals (CIs). The Youden index (maximum level of sensitivity+maximum level of specificity) was used to find the optimal cut-off points. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were also calculated. The agreements of the PCT values between the two PCT devices were determined by Cohen's κ coefficient. In all analyses, two-tailed p-values <0.05 were regarded as statistically significant.
ResultsCharacteristics of the study populationClinical suspicion of CRBSI was noted in 62 children. These subjects did not show an obvious alternative source for infection. Microbiological culture of urine and chest X-ray were negative. Thirteen children with infection other than CRBSI during hospitalization were excluded from the study. Of the remaining 49 patients, 25 (51%) were proven as not suffering from CRBSI (unproven CRBSI) and 24 (49%) were positive for CRBSI (proven CRBSI).
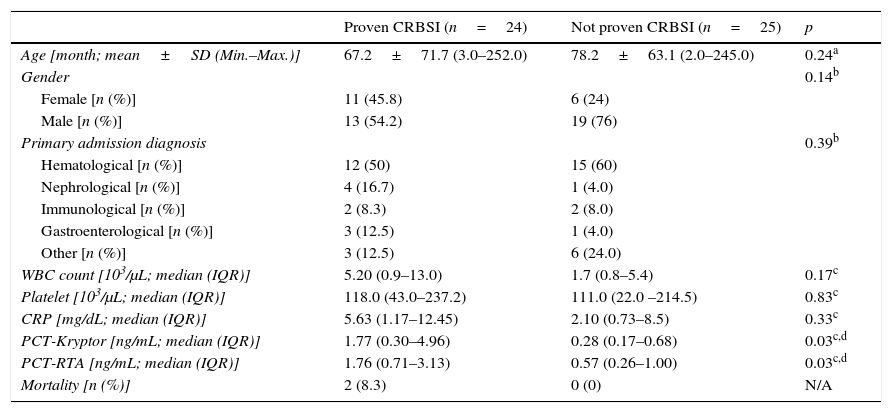
The demographic and clinical characteristics of the patients are summarized in Table 1. During the study period, 49 patients (34.7% female, n=17; 65.3% male, n=32) from the 240 beds at the Pediatric Unit of University Hospital, Ankara, Turkey, were enrolled, with a mean age of 72.8±66.9 months (range: 2–252 months). No statistically significant differences were found regarding patients’ age (p=0.24) and gender (p=0.14; Table 1). The accompanying co-morbidities were as follows: 25 (52%) patients had non-oncologic diagnosis, including chronic diarrhea, cholestasis, renal failure, neurologic diseases requiring continuous total parenteral nutrition, while the remaining 24 (48%) patients had hematologic or oncologic malignancies/diseases, including acute lymphoblastic leukemia, acute myelogenous leukemia, or central nervous system tumors (e.g., ependymoma, primitive neuroectodermal tumor; Table 1).
Patients’ demographics and clinical characteristics.
| Proven CRBSI (n=24) | Not proven CRBSI (n=25) | p | |
|---|---|---|---|
| Age [month; mean±SD (Min.–Max.)] | 67.2±71.7 (3.0–252.0) | 78.2±63.1 (2.0–245.0) | 0.24a |
| Gender | 0.14b | ||
| Female [n (%)] | 11 (45.8) | 6 (24) | |
| Male [n (%)] | 13 (54.2) | 19 (76) | |
| Primary admission diagnosis | 0.39b | ||
| Hematological [n (%)] | 12 (50) | 15 (60) | |
| Nephrological [n (%)] | 4 (16.7) | 1 (4.0) | |
| Immunological [n (%)] | 2 (8.3) | 2 (8.0) | |
| Gastroenterological [n (%)] | 3 (12.5) | 1 (4.0) | |
| Other [n (%)] | 3 (12.5) | 6 (24.0) | |
| WBC count [103/μL; median (IQR)] | 5.20 (0.9–13.0) | 1.7 (0.8–5.4) | 0.17c |
| Platelet [103/μL; median (IQR)] | 118.0 (43.0–237.2) | 111.0 (22.0 –214.5) | 0.83c |
| CRP [mg/dL; median (IQR)] | 5.63 (1.17–12.45) | 2.10 (0.73–8.5) | 0.33c |
| PCT-Kryptor [ng/mL; median (IQR)] | 1.77 (0.30–4.96) | 0.28 (0.17–0.68) | 0.03c,d |
| PCT-RTA [ng/mL; median (IQR)] | 1.76 (0.71–3.13) | 0.57 (0.26–1.00) | 0.03c,d |
| Mortality [n (%)] | 2 (8.3) | 0 (0) | N/A |
WBC, white blood cell; CRP, C-reactive protein; PCT, procalcitonin; IQR, interquartile range; CRBSI, catheter-related blood stream infection; N/A, not applicable; SD, standard deviation.
Among the 24 patients with proven CRBSI, 12 (50%) had Gram-positive bacteriemia, ten (41.7%) had Gram-negative bacteriemia, and two (8.3%) presented candidemia. The microorganisms considered responsible for CRBSI were Staphylococcus epidermidis (n=7), Klebsiella pneumoniae (n=4), Escherichia coli (n=3), Staphylococcus aureus (n=2), Staphylococcus haemolyticus (n=2), Pseudomonas aeruginosa (n=1), Klebsiella oxytoca (n=1), Acinetobacter baumannii (n=1), Enterococcus faecalis (n=1), Candida parapsilosis (n=1), and Candida lusiteniae (n=1). The group of patients with uncontrolled infection included one patient with persistent bacteremia, one patient with superinfection, and two patients who died due to CRBSI. The isolated pathogens from patients with uncontrolled infection were Gram-negative organisms, including E. coli (n=1) and K. oxytoca (n=1; responsible for death), and Gram-positive organisms, which included S. epidermidis (n=1) and S. aureus (n=1).
PCT-Kryptor and PCT-RTA values were significantly higher in patients with proven CRBSI when compared with those in patients with unproven CRBSI (p=0.03 and p=0.03, respectively). CRBSI patients did not show a significant increase in CRP values, as compared to non-CRBSI patients (p=0.33; Table 1). The distribution of PCT and CRP values according to the patient group is shown in Fig. 1. Among the 24 patients with CRBSI, CRP was significantly higher among patients with Gram-negative bacterial infection (12.30 [5.65–32.57]) than in those with Gram-positive bacterial infection (2.33 [0.40–9.15], p=0.01). PCT-Kryptor was also significantly higher among patients with Gram-negative bacterial infection (4.40 [1.69–19.22]) than in those with Gram-positive bacterial infections (0.32 [0.08–2.10], p=0.02). Among the 24 patients with CRBSI, those with uncontrolled infection did not show significant increases in PCT-Kryptor, PCT-RTA, and CRP values, when compared with patients with controlled infection (p=0.91, 0.48, and 0.14, respectively). The agreement of the PCT values between PCT-Kryptor and PCT-RTA devices was considered as intermediate (κ: 0.548).
 and C-reactive protein (CRP) according to the study groups. CRBSI, catheter-related bloodstream infection.")
The areas under the ROC curves for the diagnosis of CRBSI were 0.684 (95% CI, 0.526–0.843; p=0.03) for PCT-RTA (best cutoff, 1.18ng/mL) and 0.683 (95% CI, 0.525–0.842; p=0.03) for PCT-Kryptor (best cutoff, 0.86ng/mL; Fig. 2). The area under the ROC curves for the diagnosis of CRBSI was 0.581 (95% CI, 0.417–0.745; p=0.33) for CRP. The sensitivity, specificity, PPV, NPV, and accuracy of PCT-RTA were 0.71, 0.80, 0.77, 0.74, and 0.75, respectively. The sensitivity, specificity, PPV, NPV, and accuracy of PCT-Kryptor were 0.66, 0.84, 0.80, 0.72, and 0.75, respectively.
Discussion and C-reactive protein (CRP) for the detection of central venous catheter-related bloodstream infection (CRBSI).")
Current methods for the diagnosis of CRBSIs are time-consuming and rely on culture techniques that require 24–48h to confirm the diagnosis. Therefore, parameters that accurately distinguish CRBSI from non-CRBSI at an early stage are important.17 In the present study, PCT was considered a good diagnostic marker when compared with WBC and CRP. PCT can distinguish patients with CRBSI from patients with BSI from other sources. Additionally, on the day of clinical suspicion of the infection, a cutoff point of 0.86ng/mL of PCT was shown to distinguish patients with and without CRBSI. The specificity of the test was 0.84 and a positive result in any patient may be used as a parameter to remove central lines immediately. The RTA-PCT assay showed moderate concordance with the established Kryptor method, with an optimal cutoff of 1.18ng/mL. Therefore, this technique can be considered as a useful tool in various medical settings, although it requires further evaluation in larger studies.
The present findings are in agreement with some of the recent reports that assessed the diagnostic value of PCT for early detection of different infections in the intensive care unit (ICU).16,18,19 The diagnostic value of PCT in CRBSIs was also evaluated in a different cohort, and the present findings are consistent with those reports.16,17 However, the authors in those reports did not specifically evaluate CRBSI in children, and a proportion of their patients had suffered septic episodes.
Biomarkers of inflammation, such as the WBC count and CRP levels, can also be evaluated to diagnose CRBSIs, although their specificity is lower.20 Several studies have reported the clinical value of CRP in the diagnosis of bacterial infections, especially sepsis.14,21–23 Additionally, Theodorou et al.16 have reported that the diagnostic accuracy of PCT in patients with CRBSIs is significantly higher when compared with WBC and CRP. Consistent with this report, we have not observed significant differences in the CRP levels between patients with and without CRBSI.
In order of prevalence, the four groups of microbes that most commonly cause CRBSI associated with percutaneous insertion are coagulase-negative staphylococci, S. aureus, Candida species, and enteric Gram-negative bacilli.1 Consistent with that report,1 the dominant causative agent of CRBSI in the present study was coagulase-negative staphylococci. However, contrary to the present findings, Theodorou et al.16 have reported that Gram-negative bacteria were predominantly recovered from patients with proven CRBSI, and their patients were critically ill with prolonged intensive care unit stay. Consistent with the findings by Chen et al.,17 the present findings also underlined that the PCT concentrations and CRP levels were higher among patients with Gram-negative bacteremia than among those with Gram-positive bacterial infections. Dandona et al.24 and Linscheid et al.25 have described that serum PCT levels may be markedly increased by endotoxins (lipopolysaccharides), and the present finding may possibly be explained by such stimulations. Additionally, most of the Gram-positive bacterial infections in the present study were caused by coagulase-negative staphylococci, which is a less virulent organism than any of the listed Gram-negatives. Therefore, the determination of the NPV of the test will probably be more significant than the PPV to start on antimicrobial therapy empirically.
Several ICU cases can be empirically managed without immediate catheter withdrawal. On many occasions, watchful waiting is a prudent approach.26 Some CRBSIs in hemodynamically stable patients can be handled in situ by using antibiotics, and frequently, bacteremia is cleared and the catheter is sterilized.8,27 In 20 of the 24 patients with CRBSI in the present study, bacteremia was cleared and the catheter was sterilized with accurate antimicrobials, without removal. This result was especially important for children, considering the underlying reasons, including malignancies, in the present study. However, Gram-negative bacteria were recovered from two of the deceased children. When the patients were considered as controlled and not controlled for infection in the present study, although PCT or WBC and CRP were not the discriminating biomarkers, the PCT results may have provided the earliest opportunity to remove a catheter while awaiting the blood culture results.
Some limitations of the present study should also be noted here. First, the sample population was relatively smaller and heterogeneous regarding the underlying disease conditions. Therefore, the present results need to be confirmed in a larger and more homogeneous pool. A control group was not designed in this study, but rather two groups including proven CRBSI and unproven CRBSI from the population of children with central lines were categorized at the end of the study period to create the desired groups. Conversely, a control population with blood stream infection from children without central lines that are not catheter related may allow for a better understanding of other catheter-related blood stream infections. However, the present results are very important, due to the scarcity of studies on early CRBSI diagnosis in children. In addition, patients who had any other infection were excluded, and the withdrawal of potential confounders may increase the strength of the present findings about biomarkers as diagnostic and monitoring tools. Second, it was not possible to perform the sequential analysis of the infectious biomarkers to understand the longitudinal changes in the PCT concentration and optimal timing of the PCT for prognostic value, due to financial constraints.
In conclusion, PCT may be a useful rapid diagnostic biomarker for suspected CRBSI in children. The new automated rapid quantitative assay, the PCT-RTA (Kocaeli, Turkey), has some benefits such as small size, easy implantability in a laboratory, and ease of interpretation of the results for the measurement of PCT values. This assay, with a sensitivity and specificity of 71% and 80%, respectively, is an immunochromatographic test for the quantitative detection of PCT, and is easy to use under emergency conditions.
FundingThe study was partially supported by The Company of Dialab Tibbi Urunler ve Ozel Saglik.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Sevilay Karahan (Department of Biostatistics, Hacettepe University Faculty of Medicine, Ankara, Turkey) for the statistical analyses.
Please cite this article as: Ozsurekci Y, Oktay Arıkan K, Bayhan C, Karadağ-Öncel E, Emre Aycan A, Gürbüz V, et al. Can procalcitonin be a diagnostic marker for catheter-related blood stream infection in children? J Pediatr (Rio J). 2016;92:414–20.





