
To analyze the sociodemographic, school, and family factors associated with the patterns of binge drinking and frequent or heavy drinking among adolescents.
MethodsThis was a cross-sectional study, nested in a randomized controlled trial, of 6285 seventh and eighth grade adolescent students from Brazilian public schools. The associations between binge drinking (consumption of five or more doses of alcohol on a single occasion) in the last 12 months and frequent or heavy drinking (alcohol consumption on six or more days) in the last month and the several factors were analyzed through weighted logistic regression.
Results16.5% of the students reported binge drinking in the year before the interview and 2.2% reported frequent/heavy drinking in the previous month. The factors associated with binge drinking were cigarette smoking (OR=6.7, 95% CI=3.96; 11.23), use of marijuana (OR=2.2, 95% CI=1.17; 4.31), use of inhalant drugs (OR=3.0, 95% CI=1.98; 4.43), exposure to a drunk relative (OR=2.1, 95% C=1.67; 2.53), practice of bullying (OR=1.8, 95% CI=1.47; 2.17), verbal aggression (OR=1.7, 95%CI=1.40; 2.14), and intermediate/low school grades (OR=1.7, 95% CI=1.35; 2.20). The factors associated with frequent/heavy drinking were cigarette smoking (OR=2.5, 95% CI=1.16; 5.22), use of marijuana (OR=3.2, 95% CI=1.32; 7.72), and physical aggression (OR=2.2, 95% CI=1.36; 3.50).
ConclusionsThe analyzed outcomes showed an association between the risk consumption of alcohol in early adolescence and low academic performance, involvement with other drugs, aggressiveness, and witnessing episodes of a family member's drunkenness. Considering the impact on public health of the damages caused by alcohol consumption during adolescence, these factors that showed such association should be considered in the development of preventive interventions.
Analisar os fatores sociodemográficos, escolares e familiares associados aos padrões binge drinking, beber frequente ou beber pesado em adolescentes.
MétodosEstudo transversal aninhado em ensaio controlado randomizado entre 6.387 estudantes do 7° e 8° anos de escolas públicas brasileiras. Associações entre o binge drinking (consumo de cinco ou mais doses de álcool em uma única ocasião) nos últimos 12 meses e o beber frequente/beber pesado (consumo de álcool em seis ou mais dias) no último mês e os diversos fatores foram analisados por meio de regressão logística ponderada.
ResultadosDos estudantes, 16,5% reportaram ter praticado binge drinking no ano anterior à entrevista e 2,2% praticaram beber frequente/beber pesado no último mês. Os fatores associados ao binge drinking foram consumo de cigarro (OR=6,7, IC95%=3,96; 11,23), maconha (OR=2,2, IC95%=1,17; 4,31), uso de inalantes (OR=3,0, IC95%=1,98; 4,43), exposição a algum familiar embriagado (OR=2,1, IC95%=1,67; 2,53), prática de bullying (OR=1,8, IC95%=1,47; 2,17), agressão verbal (OR=1,7, IC95%=1,40; 2,14), notas médias e baixas (OR=1,7, IC95%=1,35; 2,20). Os fatores associados ao beber frequente/beber pesado foram o consumo de cigarro (OR=2,5, IC95%=1,16; 5,22), maconha (OR=3,2, IC95%=1,32; 7,72), agressão física (OR=2,2, IC95%=1,36; 3,50).
ConclusõesOs desfechos analisados evidenciaram associação do consumo de risco de álcool no início da adolescência com o baixo desempenho escolar, envolvimento com outras drogas, agressividade e vivência de episódios de embriaguez dos familiares. Considerando o impacto na saúde pública dos prejuízos decorrentes do consumo de risco de álcool na adolescência, estes fatores que evidenciaram associação devem ser considerados na construção de intervenções preventivas.
In Brazil, the mean age for the first episode of alcohol consumption is 12.5 years,1 and half of the adolescents aged 13–15 years have drunk at least once during their lifetime.2 Some evidence suggests that the earlier the onset of alcohol consumption, the higher the chance of developing harmful patterns of alcohol use in the future.3 To prevent these problems, it is essential to recognize the patterns of alcohol consumption that have been of greatest concern in the public health area: (1) binge drinking (BD) or episodic heavy drinking, defined by alcohol consumption of five or more doses on the same occasion4; (2) frequent drinking (FD), defined as the consumption of one dose of alcohol on six to 19 days during a one-month period; and (3) heavy drinking (HD), defined as the consumption of alcohol on 20 days or more during the month.5
In Brazil, 32% of students between the ages of 14 and 18 reported BD in the last year6 and 8.9% of students aged 10–18 years reported heavy drinking in the previous month.7 In the United States, BD has been indicated as accountable for approximately 90% of alcohol consumption among underage adolescents.8 Considering that adolescents are still living during a stage of brain maturation,9 alcohol consumption in this age group can have severe consequences: increase in hospital and emergency admission rates,10 greater risk of suicide, involvement in accidents, and episodes of domestic violence.11
Studies have shown that alcohol consumption in adolescence may be associated with a number of individual and environmental factors.1 Among the environmental factors, the family has shown to play a key role regarding the protection and the risk of alcohol consumption among adolescents.12,13 In the school context, studies show that alcohol abuse in adolescence is associated with an increase in violence,8 especially the practice of bullying,14 and worsened academic performance.11 It is noteworthy that alcohol abuse in adolescence is also associated with early use of tobacco and illicit drugs,15 potentializing its harmful effects.
Although the damages caused by alcohol consumption in adolescence are quite evident in the scientific literature, there are still few Brazilian studies that have attempted to understand the impact of different patterns of alcohol consumption on the development of adolescents (FD and HD). Considering that Brazil has a very particular culture related to alcohol consumption, with a high rate of permissiveness regarding consumption and weak regulatory control of the promotion and sale of alcoholic beverages,16 it is necessary to invest in Brazilian studies that can understand this reality. Thereby, it would be possible to provide subsidies for the development of preventive measures that are based on Brazilian evidence, considering the cultural influence on alcohol consumption by adolescents. Thus, the aim of this study was to identify the main sociodemographic, school, and family factors associated with BD/FD/HD among Brazilian students who recently entered adolescence.
Materials and methodsThis is a cross-sectional study, nested in a randomized controlled trial, using data initially collected for the evaluation of a school-based drug prevention program entitled #Tamojunto (the Portuguese of “#Wearetogether”). It was a probabilistic sample of 7th and 8th grade students from 72 public schools in six Brazilian municipalities (São Paulo, Federal District, São Bernardo do Campo, Florianópolis, Fortaleza, and Tubarão). #Tamojunto is an adaptation, carried out by the Ministry of Health in partnership with UNODC do Brasil (United Nations Office on Drugs and Crime), and the European program Unplugged, developed and tested by the EU-Dap (European Drug Addiction Prevention Trial).17
The municipalities were selected by the Ministry of Health and the schools were selected by drawing lots from the total number of schools with these grades, in each city, through the Instituto de Estudos e Pesquisas Educacionais Anísio Teixeira (INEP) list using a quantity that was proportional to the total number of students enrolled in each municipality. Among the schools selected to participate in the study, a second simple random draw established whether each school would be allocated to the control or intervention group, maintaining an allocation ratio of 1:1 per municipality. The intervention group received 12 classes from the #Tamojunto program and the control group received no intervention. The randomization was performed at the school level using an Excel macro [RAND command] (Microsoft Office Excel, WA, USA). At each school, all eighth grade classes were included. In the municipalities of Florianópolis, Tubarão, and Fortaleza, at the request of the Municipal Education Secretariats, 7th Grade students were also included, due to the transition to the new school regimen established in Brazil. Initial data were collected in both groups two weeks before the program was implemented.
This study was registered at the Brazilian Registry of Clinical Trials (REBEC – Registro Brasileiro de Ensaios Clínicos) of the Brazilian Ministry of Health under number RBR-4mnv5g, and its protocol was approved by the Research Ethics Committee of Universidade Federal de São Paulo (protocol No. 473,498).
SamplingThe sample consisted of 6387 students attending the 7th and 8th grades of Elementary School from 261 classes of 72 public schools in the six municipalities.
The sample size was calculated for longitudinal studies,18 with a power of 80%, significance level of 5%, and a predicted mean reduction of 1.5% in the prevalence of BD, which was estimated at 5%. Considering 2835 for each group (intervention and control), the total number of students required for the study was established at 5670 students. After defining the required sample size, a mean of four classes per school was calculated and a total of 40 schools were randomly selected in each arm. The flowchart with data from the first two data collections was published in a previous study.17
Of the schools that accepted to participate, considering the enrollment registers, the presence of 8547 students in the participating classes was expected. However, a total of 6771 students were present, of whom 59 refused to participate, generating a refusal rate of 0.8%, although the number of absent students on the day of collection represented 20% of the students enrolled in these classes.
Tool and measuresThe data were collected through an anonymous, self-completed questionnaire, applied by researchers in the classroom without the presence of a teacher. The tool used for data collection was developed and tested by the EU-DAP and was applied in previous Unplugged studies.19 In Brazil, it was translated and adapted to the Portuguese language,20 resulting in some changes based on questions from two questionnaires widely used in studies with Brazilian students: a World Health Organization questionnaire used by the Brazilian Center for Information on Psychotropic Drugs21 (Centro Brasileiro de Informação sobre Drogas Psicotrópicas) to investigate the use of drugs in schools and a questionnaire used by the Brazilian National School Health Survey2 (Pesquisa Nacional de Saúde do Escolar [PeNSE]).
To identify the questionnaires in the study phases, the students generated a “secret code” with letters and numbers, created based on personal information. These codes allowed the researchers to compare the questionnaires at different times of follow-up, while simultaneously protecting the participants by providing the anonymity and confidentiality that are essential to a study of illicit behavior.22
To ensure a minimum information bias in the questionnaires, a question about the use of fictitious drugs (Holoten and Carpinol) was included. This question led to the exclusion of 49 students at baseline.
Response variable: The response variables (outcomes) considered in this study were: (1) BD during the last year, where BD corresponded to the confirmation to the question “Since last year, that is, during the last 12 months, have you had five or more doses of alcoholic beverages on a single occasion?”; (2) FD/HD of alcohol in the last 30 days. This variable was the result of grouping the answers to the question “During the last month, that is, during the last 30 days, did you drink any alcoholic beverages?”. The answers “No” and “Yes, I drank on one to five days during the month” were considered as No FD/HD behavior; and the answers “Yes, I drank on six to 19 days during the month” and “Yes, I drank on 20 days or more during the month” as FD/HD behavior. FD and HD were grouped due to the low prevalence of HD in this age group.
Investigated covariates: The covariates of interest were the (1) sociodemographic variables (gender, age, socioeconomic class, and family composition); (2) practice of school violence in the last 30 days (bullying, physical, and verbal aggression) measured through three dichotomous questions (yes/not); (3) students’ academic performance in the last year, where the students had to classify their school grades as low, intermediate or high; (4) sporadic alcohol consumption and exposure to a family member's drunkenness episodes (parents/siblings), both variables collected through dichotomous questions (yes/not); (5) use of other drugs (cigarette smoking, use of inhalant drugs, and marijuana) in the last year and in the last month, measured through dichotomous questions (yes/not); (6) BD during the last year and alcohol consumption characterized as FD/HD in the last 30 days (control variables).
The socioeconomic class evaluation was carried out according to the ABEP23 scale, which considers the educational level of the household head, goods present, and services used, with scores varying from 0 to 46; the higher the score, the better the student's social status.
Statistical analysisThe analyses were performed using weighted data to correct unequal probabilities of sample selection. The sample weights considered the school as the primary sampling unit, with stratification by city, the total number of students expected in each class and those present on the day of the survey. An initial multiple logistic regression model, including the explanatory variables with a p-value ≤0.20 was considered. A backward procedure was used to remove the explanatory variables aiming to obtain a final model for each response variable.
The chi-squared test was applied to verify the association between response variables and covariates. To verify the joint association of variables, multiple logistic regression models were estimated for each response variable. The level of significance was set at 5%.
The analyses were performed with the software Stata 14 (SPSS for Windows, version 14.0, Chicago, USA) using a svyset command to ensure the inclusion of sample weights and determine the appropriate variance estimate of this complex sample.
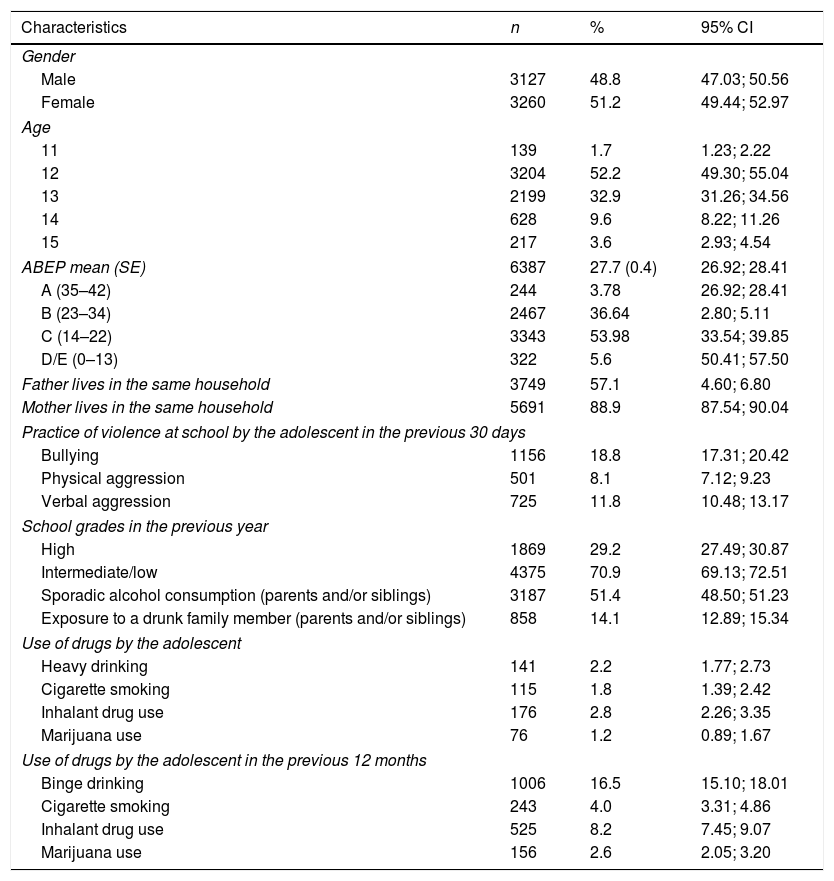
ResultsTable 1 shows the main characteristics of the students. The mean age of the interviewees was 12.6 years (SE=0.3), with girls accounting for half of those interviewed. In the previous month, 2.2% reported FD/HD and in the previous year, 16.5% reported BD. 11% of students reporting BD in the previous year also reported FD/HD in the previous month. However, 80% of the students who reported FD/HD also reported BD behavior.
Sociodemographic, behavioral, and family characteristics, and drug use among the students (n=6387).
| Characteristics | n | % | 95% CI |
|---|---|---|---|
| Gender | |||
| Male | 3127 | 48.8 | 47.03; 50.56 |
| Female | 3260 | 51.2 | 49.44; 52.97 |
| Age | |||
| 11 | 139 | 1.7 | 1.23; 2.22 |
| 12 | 3204 | 52.2 | 49.30; 55.04 |
| 13 | 2199 | 32.9 | 31.26; 34.56 |
| 14 | 628 | 9.6 | 8.22; 11.26 |
| 15 | 217 | 3.6 | 2.93; 4.54 |
| ABEP mean (SE) | 6387 | 27.7 (0.4) | 26.92; 28.41 |
| A (35–42) | 244 | 3.78 | 26.92; 28.41 |
| B (23–34) | 2467 | 36.64 | 2.80; 5.11 |
| C (14–22) | 3343 | 53.98 | 33.54; 39.85 |
| D/E (0–13) | 322 | 5.6 | 50.41; 57.50 |
| Father lives in the same household | 3749 | 57.1 | 4.60; 6.80 |
| Mother lives in the same household | 5691 | 88.9 | 87.54; 90.04 |
| Practice of violence at school by the adolescent in the previous 30 days | |||
| Bullying | 1156 | 18.8 | 17.31; 20.42 |
| Physical aggression | 501 | 8.1 | 7.12; 9.23 |
| Verbal aggression | 725 | 11.8 | 10.48; 13.17 |
| School grades in the previous year | |||
| High | 1869 | 29.2 | 27.49; 30.87 |
| Intermediate/low | 4375 | 70.9 | 69.13; 72.51 |
| Sporadic alcohol consumption (parents and/or siblings) | 3187 | 51.4 | 48.50; 51.23 |
| Exposure to a drunk family member (parents and/or siblings) | 858 | 14.1 | 12.89; 15.34 |
| Use of drugs by the adolescent | |||
| Heavy drinking | 141 | 2.2 | 1.77; 2.73 |
| Cigarette smoking | 115 | 1.8 | 1.39; 2.42 |
| Inhalant drug use | 176 | 2.8 | 2.26; 3.35 |
| Marijuana use | 76 | 1.2 | 0.89; 1.67 |
| Use of drugs by the adolescent in the previous 12 months | |||
| Binge drinking | 1006 | 16.5 | 15.10; 18.01 |
| Cigarette smoking | 243 | 4.0 | 3.31; 4.86 |
| Inhalant drug use | 525 | 8.2 | 7.45; 9.07 |
| Marijuana use | 156 | 2.6 | 2.05; 3.20 |
ABEP, scale used to assess socioeconomic class.
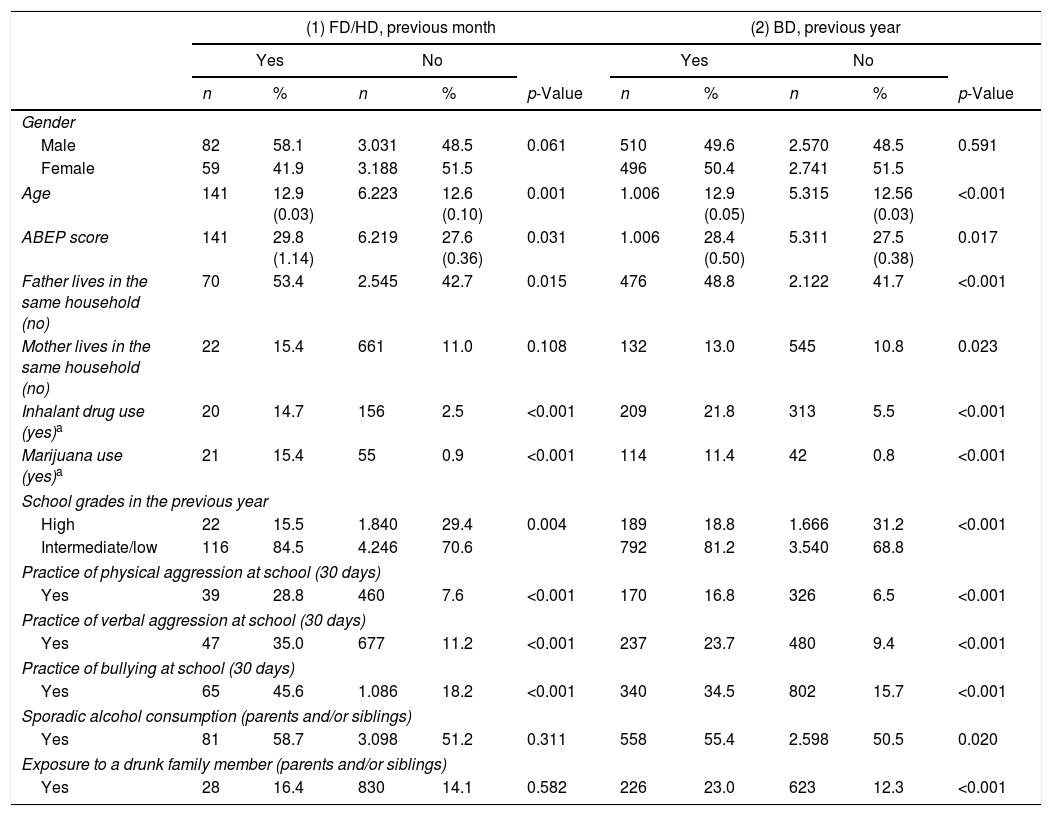
The proportion of boys among those who reported FD/HD (Table 2) was 58.5%. There was evidence of common positive associations between the practices of FD/HD and BD and the following behaviors: drug use in the previous month (cigarette smoking, use of inhalant drugs, and marijuana), episodes of violence in the previous month (physical and verbal aggression, and the practice of bullying) and the report of low or intermediate school grades in the previous year. Additionally, it was observed that not living with one's father was also associated with the practice of FD/HD. It was also observed that the BD pattern (Table 2) was associated with exposure to drunk relatives and those that consumed alcohol.
Sociodemographic, behavioral, and family characteristics, and drug use among the students related to: (1) frequent/heavy drinking habits in the previous month, and (2) binge drinking in the previous year.
| (1) FD/HD, previous month | (2) BD, previous year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | |||||||
| n | % | n | % | p-Value | n | % | n | % | p-Value | |
| Gender | ||||||||||
| Male | 82 | 58.1 | 3.031 | 48.5 | 0.061 | 510 | 49.6 | 2.570 | 48.5 | 0.591 |
| Female | 59 | 41.9 | 3.188 | 51.5 | 496 | 50.4 | 2.741 | 51.5 | ||
| Age | 141 | 12.9 (0.03) | 6.223 | 12.6 (0.10) | 0.001 | 1.006 | 12.9 (0.05) | 5.315 | 12.56 (0.03) | <0.001 |
| ABEP score | 141 | 29.8 (1.14) | 6.219 | 27.6 (0.36) | 0.031 | 1.006 | 28.4 (0.50) | 5.311 | 27.5 (0.38) | 0.017 |
| Father lives in the same household (no) | 70 | 53.4 | 2.545 | 42.7 | 0.015 | 476 | 48.8 | 2.122 | 41.7 | <0.001 |
| Mother lives in the same household (no) | 22 | 15.4 | 661 | 11.0 | 0.108 | 132 | 13.0 | 545 | 10.8 | 0.023 |
| Inhalant drug use (yes)a | 20 | 14.7 | 156 | 2.5 | <0.001 | 209 | 21.8 | 313 | 5.5 | <0.001 |
| Marijuana use (yes)a | 21 | 15.4 | 55 | 0.9 | <0.001 | 114 | 11.4 | 42 | 0.8 | <0.001 |
| School grades in the previous year | ||||||||||
| High | 22 | 15.5 | 1.840 | 29.4 | 0.004 | 189 | 18.8 | 1.666 | 31.2 | <0.001 |
| Intermediate/low | 116 | 84.5 | 4.246 | 70.6 | 792 | 81.2 | 3.540 | 68.8 | ||
| Practice of physical aggression at school (30 days) | ||||||||||
| Yes | 39 | 28.8 | 460 | 7.6 | <0.001 | 170 | 16.8 | 326 | 6.5 | <0.001 |
| Practice of verbal aggression at school (30 days) | ||||||||||
| Yes | 47 | 35.0 | 677 | 11.2 | <0.001 | 237 | 23.7 | 480 | 9.4 | <0.001 |
| Practice of bullying at school (30 days) | ||||||||||
| Yes | 65 | 45.6 | 1.086 | 18.2 | <0.001 | 340 | 34.5 | 802 | 15.7 | <0.001 |
| Sporadic alcohol consumption (parents and/or siblings) | ||||||||||
| Yes | 81 | 58.7 | 3.098 | 51.2 | 0.311 | 558 | 55.4 | 2.598 | 50.5 | 0.020 |
| Exposure to a drunk family member (parents and/or siblings) | ||||||||||
| Yes | 28 | 16.4 | 830 | 14.1 | 0.582 | 226 | 23.0 | 623 | 12.3 | <0.001 |
ABEP, scale used to assess socioeconomic class.
Due to the temporal difference of the outcome, when BD was the dependent variable, the variables cigarette smoking, use of inhalant drugs, and marijuana were considered in the previous 12 months. When FD/HD was the dependent variable, the variables cigarette smoking, use of inhalant drugs, and marijuana were considered in the previous 30 days.
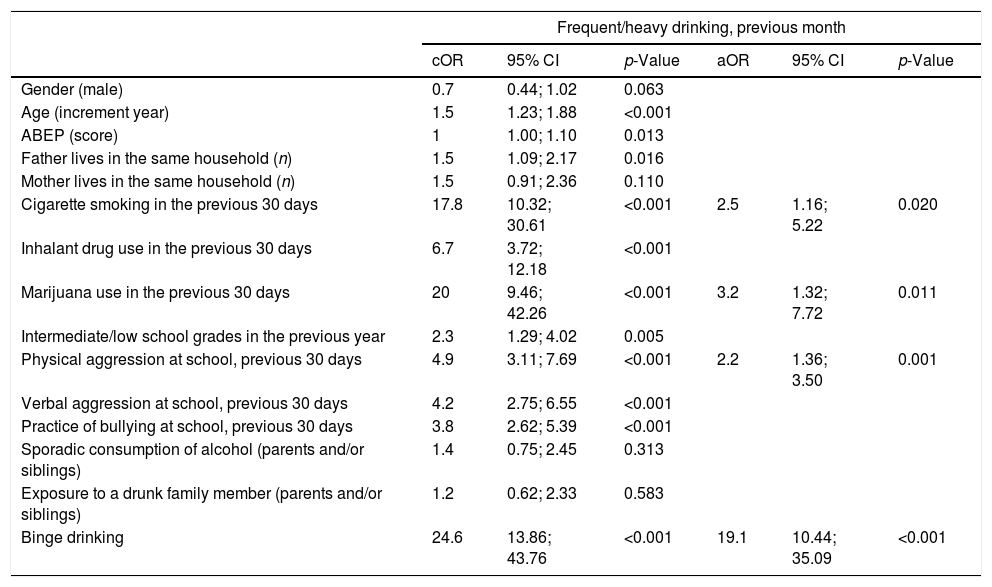
In the adjusted logistic regression model for the practice of FD/HD (Table 3), independent of BD, the factors that showed association were drug consumption (cigarette smoking and use of marijuana), physical aggression, and BD.
Estimates of crude (cOR) and adjusted odds ratios (aOR) for heavy/frequent drinking habits in the previous month, according to the sociodemographic, behavioral, and family characteristics, and drug use among the students.
| Frequent/heavy drinking, previous month | ||||||
|---|---|---|---|---|---|---|
| cOR | 95% CI | p-Value | aOR | 95% CI | p-Value | |
| Gender (male) | 0.7 | 0.44; 1.02 | 0.063 | |||
| Age (increment year) | 1.5 | 1.23; 1.88 | <0.001 | |||
| ABEP (score) | 1 | 1.00; 1.10 | 0.013 | |||
| Father lives in the same household (n) | 1.5 | 1.09; 2.17 | 0.016 | |||
| Mother lives in the same household (n) | 1.5 | 0.91; 2.36 | 0.110 | |||
| Cigarette smoking in the previous 30 days | 17.8 | 10.32; 30.61 | <0.001 | 2.5 | 1.16; 5.22 | 0.020 |
| Inhalant drug use in the previous 30 days | 6.7 | 3.72; 12.18 | <0.001 | |||
| Marijuana use in the previous 30 days | 20 | 9.46; 42.26 | <0.001 | 3.2 | 1.32; 7.72 | 0.011 |
| Intermediate/low school grades in the previous year | 2.3 | 1.29; 4.02 | 0.005 | |||
| Physical aggression at school, previous 30 days | 4.9 | 3.11; 7.69 | <0.001 | 2.2 | 1.36; 3.50 | 0.001 |
| Verbal aggression at school, previous 30 days | 4.2 | 2.75; 6.55 | <0.001 | |||
| Practice of bullying at school, previous 30 days | 3.8 | 2.62; 5.39 | <0.001 | |||
| Sporadic consumption of alcohol (parents and/or siblings) | 1.4 | 0.75; 2.45 | 0.313 | |||
| Exposure to a drunk family member (parents and/or siblings) | 1.2 | 0.62; 2.33 | 0.583 | |||
| Binge drinking | 24.6 | 13.86; 43.76 | <0.001 | 19.1 | 10.44; 35.09 | <0.001 |
ABEP, scale used to assess socioeconomic class.
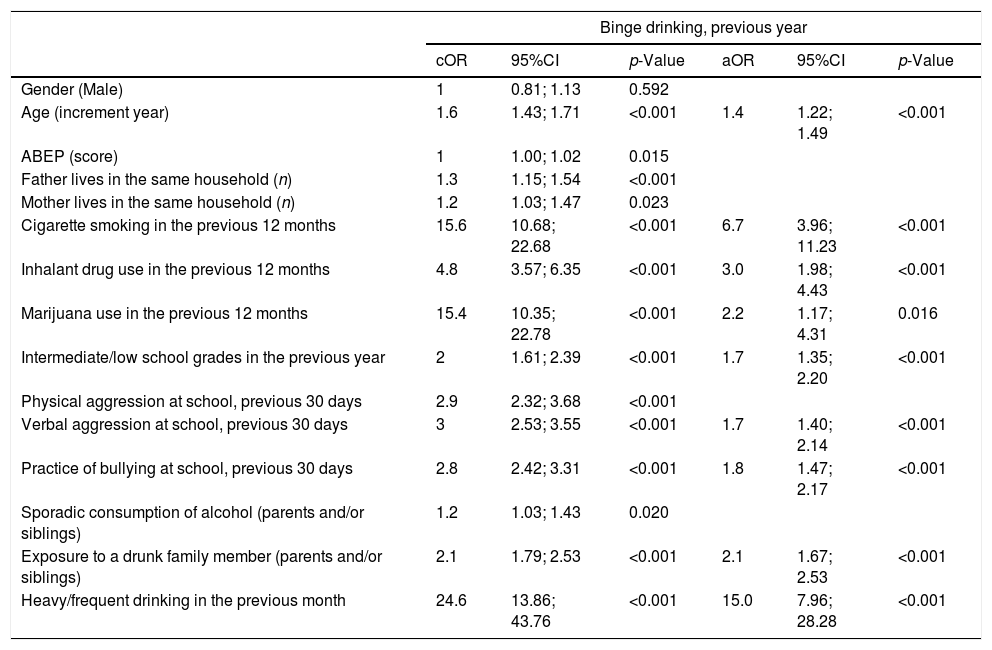
In the adjusted logistic regression model for the practice of BD (Table 4), controlled by FD/HD, the associated factors were cigarette smoking, use of marijuana and inhalant drugs, exposure to a drunk relative, the practice of bullying, verbal aggression, intermediate or low grades at school, and age.
Estimates of crude (cOR) and adjusted odds ratios (aOR) for binge drinking in the previous year, according to the sociodemographic, behavioral, and family characteristics, and drug use among the students.
| Binge drinking, previous year | ||||||
|---|---|---|---|---|---|---|
| cOR | 95%CI | p-Value | aOR | 95%CI | p-Value | |
| Gender (Male) | 1 | 0.81; 1.13 | 0.592 | |||
| Age (increment year) | 1.6 | 1.43; 1.71 | <0.001 | 1.4 | 1.22; 1.49 | <0.001 |
| ABEP (score) | 1 | 1.00; 1.02 | 0.015 | |||
| Father lives in the same household (n) | 1.3 | 1.15; 1.54 | <0.001 | |||
| Mother lives in the same household (n) | 1.2 | 1.03; 1.47 | 0.023 | |||
| Cigarette smoking in the previous 12 months | 15.6 | 10.68; 22.68 | <0.001 | 6.7 | 3.96; 11.23 | <0.001 |
| Inhalant drug use in the previous 12 months | 4.8 | 3.57; 6.35 | <0.001 | 3.0 | 1.98; 4.43 | <0.001 |
| Marijuana use in the previous 12 months | 15.4 | 10.35; 22.78 | <0.001 | 2.2 | 1.17; 4.31 | 0.016 |
| Intermediate/low school grades in the previous year | 2 | 1.61; 2.39 | <0.001 | 1.7 | 1.35; 2.20 | <0.001 |
| Physical aggression at school, previous 30 days | 2.9 | 2.32; 3.68 | <0.001 | |||
| Verbal aggression at school, previous 30 days | 3 | 2.53; 3.55 | <0.001 | 1.7 | 1.40; 2.14 | <0.001 |
| Practice of bullying at school, previous 30 days | 2.8 | 2.42; 3.31 | <0.001 | 1.8 | 1.47; 2.17 | <0.001 |
| Sporadic consumption of alcohol (parents and/or siblings) | 1.2 | 1.03; 1.43 | 0.020 | |||
| Exposure to a drunk family member (parents and/or siblings) | 2.1 | 1.79; 2.53 | <0.001 | 2.1 | 1.67; 2.53 | <0.001 |
| Heavy/frequent drinking in the previous month | 24.6 | 13.86; 43.76 | <0.001 | 15.0 | 7.96; 28.28 | <0.001 |
ABEP, scale used to assess socioeconomic class.
The present study analyzed the associations between sociodemographic, school, and family factors and alcohol consumption patterns (BD, FD/HD) in early adolescence, through a large sample of students from Brazilian public schools. The main results of this study were: (1) harmful patterns of alcohol use are already prevalent in early adolescence; (2) drug use was shown to be associated with both BD and FD/HD; (3) intermediate and lower school grades also showed an association with BD; (4) school violence showed an association with both BD and FD/HD behaviors; and (5) drunkenness episodes in family members were associated only with the practice of BD among the adolescents.
This study identified an annual prevalence of 16.5% in the practice of BD and a 2.2% monthly prevalence for HD/FD among students with a mean age of 12.6 years attending the Brazilian public school network. It is worth noting that the annual measure was used to evaluate BD, as it is a more acute consumption, with larger amounts consumed within a shorter time, more common on weekends, at parties, and in bars.4 A previous study revealed a 53% prevalence of BD per year among Brazilian male adolescents aged 14–19 years and a 9.1% prevalence of FD.24 Another Brazilian study carried out with adolescents aged 14–18 years found an annual prevalence of 32% for BD.6 A high prevalence of annual BD was also observed among adolescents from European countries, such as the United Kingdom (47.0%)25 and Sweden (30.8%).26 The prevalence rates observed in previous studies were higher when compared to those of the present study, probably due to the fact that the students participating in the previous studies were older. The present research is one of the few that enrolled students at the start of adolescence, which makes it an innovative study, by assessing patterns of harmful consumption closer to the onset of their occurrence. Another important point to be mentioned is that 80% of the students with FD/HD pattern also showed the BD behavior, which indicates an association between the different patterns of risk consumption of alcohol in adolescence.
The results of this study indicate that the use of other drugs is associated with the different patterns of alcohol consumption, both with BD and FD/HD. Another Brazilian study also found an association between BD and the use of illicit drugs,27 and longitudinal international studies have confirmed this same trend.15 These findings suggest that the risk consumption of alcohol in adolescence may precede the use of other drugs, which corroborates previous evidence showing that alcohol is the first drug consumed by adolescents and that some of them progress to the use of other drugs. However, since this study had a cross-sectional design, order and causality cannot be established.
Regarding the school factors, this study found an association between the risk consumption of alcohol and violence outcomes. Other studies also found this association between alcohol and violence among adolescents.8,14 Students who practice bullying may have emotional and adaptive difficulties in the school environment, which may interfere with the learning process,28 making them more vulnerable to other risk behaviors, such as the risk use of alcohol. The report of intermediate and low school grades was shown to be associated with BD, since the student with low and intermediate school grades may also show an increased risk of alcohol consumption due to the consequent decrease in self-esteem,11 relationships with deviant peers,29 or due to the presence of some psychiatric comorbidity.30 In turn, low academic performance and the practice of violence can also be explained as a consequence of alcohol use, caused by the changes in the cognitive development resulting from the risk consumption of alcohol in adolescence.31
It is noteworthy that exposure to a drunk parent seemed to be associated with BD in early adolescence. Many studies suggest that parents can be seen as a model of behavior for their children, reinforcing the findings of this study.3,12 Thus, it seems that parents who have an alcohol use disorder are more tolerant regarding the start of their children's alcohol consumption and create a favorable environment for the occurrence of this consumption.32 These findings indicate the need for preventive programs to be directed at parents, in parallel to those exclusively aimed at adolescents, in order to alert about the influence of the parents’ alcohol consumption on the use of alcohol by their children.
The first limitation to be considered in this study refers to the fact that all information was obtained through a self-completion questionnaire, which may bring an information bias to the study. However, this is a common bias for the vast majority of studies in the drug abuse field,21 and the authors tried to minimize it by ensuring anonymity and the absence of a teacher in the classroom during data collection. Another limitation is the fact that the results refer to students enrolled in public schools and, thus, the data might be extrapolated to students attending private schools, for whom the prevalence of BD may be higher.6 The potential loss of 20% of students who were not present in the classroom on the day of the study should also be mentioned. The initial number of students potentially enrolled in the study (n=8247) was estimated based on the students’ database provided by INEP; however, it was verified that not all enrolled students were actually attending the school. This discrepancy is a problem of the Brazilian social context, where the school attendance of the enrolled children constitutes a challenge. Additionally, the fact that this was a cross-sectional study limited the causal interpretation of the associations between the analyzed factors and the outcomes.
In conclusion, this study identified the patterns of BD and FD/HD behaviors in Brazilian adolescents that recently started adolescence, and found a number of risk factors that are associated with these patterns: involvement with other drugs, low academic performance, aggressiveness, and alcohol use disorder of a family member. By understanding these behaviors associated with risk drinking in adolescence, it is suggested that school prevention programs include the topics of drug use and violence into their curricula through multicomponent interventions, and provide a brief intervention aimed at the parents who need support to reduce harmful alcohol consumption.
Conflicts of interestThe authors declare no conflicts of interest.
FundingThis study was funded by the Ministry of Health of Brazil (TED 89/2014). The authors thank the staff of the Ministry of Health and the United Nations Office on Drugs and Crime (UNODC). They especially thank the principals and teachers of the schools, field researchers, and most of all the students who participated in the study.
The submitted manuscript was read and approved by all authors. All authors acknowledge they exercised due care to ensure the integrity of the work. LC was responsible for writing the manuscript and reviewing the literature, and also wrote the first version of the manuscript. CBM performed the statistical analysis and wrote the results. SA was responsible for sampling and sample weight. JYV was responsible for the critical review of the entire manuscript and wrote its second version. ZS supervised all stages of the manuscript as the study main investigator and was responsible for the final version submitted to publication. No original material contained in this manuscript has been submitted for consideration to another journal, nor will be published elsewhere.
Please cite this article as: Conegundes LS, Valente JY, Martins CB, Andreoni S, Sanchez ZM. Binge drinking and frequent or heavy drinking among adolescents: prevalence and associated factors. J Pediatr (Rio J). 2020;96:193–201.




