


To assess the association between general and abdominal obesity with high blood pressure in adolescents of both genders from the public school system.
MethodsThis was an epidemiological, descriptive, exploratory study, with a quantitative approach and local scope whose sample consisted of 481 high school students (aged 14–19), selected by using a random cluster sampling strategy. Blood pressure was measured through the use of automated monitor and was considered high when the pressure values were at or above the 95th percentile. The analyses were performed using the chi-squared test and binary logistic regression.
ResultsThe prevalence of high blood pressure was 6.4%, and it was higher among boys (9.0% vs. 4.7%, p<0.05). There was no significant difference between general (p=0.903) and abdominal obesity (p=0.157) when genders were compared. After adjusting for age, high blood pressure was associated with general (OR=6.4; p<0.001) and abdominal obesity (OR=7.0; p<0.001) only among boys, when comparing the fourth quartile with the first quartile of body mass index (≤18.6kg/m2vs. ≥23.5kg/m2) and waist circumference (≤69cm vs. ≥80.1cm).
ConclusionIt was observed that general and abdominal obesity are associated with high blood pressure only in boys, regardless of age.
Analisar a associação entre obesidade geral e abdominal com a pressão arterial elevada em adolescentes de ambos os gêneros da rede de ensino público.
MétodosTrata-se de um estudo epidemiológico, descritivo, exploratório, com abordagem quantitativa e abrangência municipal cuja amostra foi constituída de 481 estudantes (14-19 anos) do ensino médio, selecionado por meio de uma estratégia de amostragem aleatória de cluster. A pressão arterial foi medida através da utilização de equipamentos automáticos, sendo considerada elevada quando os valores pressóricos estivessem iguais ou acima do percentil 95. As análises foram realizadas através do teste de Qui-quadrado e da regressão logística binária.
ResultadosA prevalência de pressão arterial elevada foi de 6,4%, sendo maior entre os rapazes (9,0% vs. 4,7%, p<0,05). Não foi observada diferença significante entre a obesidade geral (p=0,903) e abdominal (p=0,157) quando comparados os gêneros. Após o juste pela idade, a pressão arterial elevada foi associada com a obesidade geral (OR=6,4; p<0,001) e abdominal (OR=7,0; p<0,001) apenas entre os rapazes, quando comparado o quarto quartil com o primeiro quartil do índice de massa corporal (≤ 18,6 Kg/m2 Vs ≥23,5 Kg/m2) e da circunferência da cintura (≤ 69cm Vs ≥80,1cm).
ConclusãoFoi observado que a obesidade geral e abdominal está associada com a pressão arterial elevada apenas entre os rapazes, independentemente da idade.
High blood pressure (HBP) is considered a major risk factor for cardiovascular disease for adults, as well as children and adolescents.1,2 Its diagnosis and early treatment can prevent the occurrence of future adverse cardiovascular events, since HBP in childhood is a predictor of hypertension in adulthood.3 In Brazil, the prevalence of HBP in children ranges from 2.5%4 to 44.7%5; as it is asymptomatic, the identification and treatment of HBP is often neglected.6
By consensus, general and abdominal obesity are considered as predisposing factors for HBP onset7; moreover, excess body fat accumulation in the early stages of life is associated with the onset of cardiovascular and metabolic diseases in adulthood.8 However, there is evidence demonstrating that body fat distribution is more important than obesity alone.9,10 In this sense, it has been observed that abdominal fat accumulation is closely related to HBP, and it is considered the biggest contributor to metabolic complications of the obese population.11
Another factor that can influence blood pressure (BP) values is the difference between genders.12,13 Studies have confirmed that boys have higher BP than girls.14–16 However, the association between obesity and HBP is usually assessed, but the interaction in relation to gender is not tested, and this factor can distort the found results.1,16 Therefore, the objective of this study was to analyze the association between general and abdominal obesity with HBP in adolescents from public schools, while considering the difference between genders.
MethodsThis was a descriptive study with a quantitative approach that integrated a school-based cross-sectional epidemiological survey of municipal scope. The sample consisted of students aged 14–19 years, of both genders, enrolled in the state public high schools in the city of Caruaru, state of Pernambuco, Brazil. The total population was estimated at 8833 young individuals distributed in 15 schools, according to the State Secretariat of Education and Culture.
The following parameters were used to calculate sample size: 95% of confidence interval; maximum tolerable error of 2 percentage points; design effect (deff)=2; and, because this study comprehended the analysis of multiple risk behaviors and different frequencies of occurrence, the estimated prevalence was defined as 50%. Additionally, to minimize the limitations caused by eventual losses in the application and/or inadequate completion of the questionnaires, it was decided to add 20% to the sample size.
To select the required sample, a two-stage random cluster sampling strategy was used, and “school” and “class” represented, respectively, the sample units in the first and second stage. All public schools in the city of Caruaru were considered eligible for inclusion in the study. In the first stage, school density was used as the stratification criterion in each microregion of the city (Gerência Regional de Educação – Gere), according to their size. In the second stage, the density of classes in the selected schools was considered by school shift (day and night) as a criterion to choose, by drawing lots, those in which the questionnaires would be applied. All students in the selected classes were asked to participate in the study, regardless of their age. After their application, the questionnaires answered by students older than the established age (19 years) were excluded.
Data collection was carried out from June to November of 2014. The questionnaires were collectively applied in the classroom, without the presence of their teachers, and the students were continuously assisted by five researchers (two professors and three undergraduate students), to clarify doubts when filling out the questionnaires. The study was approved by the Ethics Committee in Research with human beings of Faculdade Asces (CAAE-22210913.8.0000.5203/CEP-ASCES: 072403/2013). Subject participation was voluntary and anonymous, and a passive parental consent form was obtained.
Personal information, as well as socioeconomic and sociodemographic variables, were acquired through the translated and adapted version of the Global School-based Student Health Survey (GSHS), proposed by the World Health Organization (WHO). At the anthropometric measurements, all adolescents wore light clothing and were barefoot. Body mass was measured in an electronic Beurer scale (Beurer GmbH, Ulm, Germany) with a maximum capacity of 150kg and accuracy of 100g. Height was measured using a portable stadiometer (Wiso, SC, Brazil) with an accuracy of 0.5cm. Body mass index (BMI) was calculated by dividing body weight in kilograms by the square of height in meters. Waist circumference (WC) was determined as the minimum circumference between the iliac crest and the last rib, using a non-extendable metric tape (Sanny, SP, Brazil) graduated in millimeters. After the calculations of BMI and waist circumference, the data were categorized into quartiles as used in a previous study with adolescents.17
Blood pressure was measured using an automated oscillometric device (Omron HEM-742, Omrom Healthcare, INC, IL, USA) was used, which was previously calibrated and validated for adolescents.18 Cuff adjustment followed the recommendations of the American Heart Association.19 Three blood pressure measurements were taken, after a one-minute interval between them, carefully following the protocols recommended by the VI Brazilian Guidelines on Hypertension,20 as well as in relation to the positioning of the arm and body, prior rest, instrument calibration, size of the sphygmomanometer cuff, number of measurements taken, and the choice of the value used to determine prevalence.
Regarding the BP value used, the first measurement was discarded and the mean of the last two measurements was used, both for the systolic and diastolic pressure. The criteria used to classify the subjects were those established by the National High Blood Pressure Education Program21; thus, for the age group 14–17 years, HBP was considered when the systolic blood pressure (SBP) or diastolic blood pressure (DBP) was equal to or greater than the 95th percentile of the Task Force Report High Blood Pressure in Children and Adolescents, 1996 reference tables for age and gender, adjusted for the height percentile of the assessed adolescent. For students aged 18–19, the values used for young adults were considered as parameters.
The final data tabulation was performed using the EpiData program, version 3.1 (Epidata Association, Odense, Denmark), a public domain system, which was also used to carry out the electronic procedures for data entry control through the check function (controls). In order to detect errors, data entry was repeated and, using the duplicate file comparison function, typing errors were detected and corrected.
Data analysis was performed using SPSS (SPSS Inc. Statistics for Windows, Version 10.0, IL, USA). Frequency distribution was observed in the descriptive analysis. Pearson's chi-squared test was used in the inferential analysis to analyze the isolated association between HBP and general and abdominal obesity, the difference between the BP of boys and girls, and general and abdominal obesity between boys and girls, as well as to analyze the variables in the model, explore the potential confounders, and identify the need for statistical adjustment of the analyses.
In the multivariate analysis, binary logistic regression was used, by estimating the odds ratio (OR) and 95% confidence intervals to express the degree of association between the independent variables (general and abdominal obesity) and the dependent variable (HBP), using adjustment for age, as performed in other studies.22,23 In addition to the biological plausibility, the age variable showed, in relation to BP, a statistical significance level<0.20 (p<0.20), a criterion used for entry in the statistical model using the backward method. After obtaining the predictive variables of the final model, the interaction occurrence was tested. The significance level was set at p<0.05 for all tests.
Skin color, maternal level of schooling, occupation, and place of residence did not enter the statistical model, as they had a statistical significance level<0.20 in relation to BHP: p=0.764, p=0.884, p=0.259, and p=0.526, respectively.
ResultsNine schools of the public state educational system located in the city of Caruaru were assessed. Of the 569 students who were in class on the day of data collection, 31 adolescents refused to participate and 26 were not allowed to participate in the study by their parents or guardians, totaling 57 refusals. Data were collected from 512 adolescents; however, the final sample, corresponding to students aged between 14 and 19 years, comprised 481 students, of whom 54.1% were females. The characteristics of the adolescents are shown in Table 1.
Socioeconomic and demographic characteristics and prevalence of high blood pressure and general and abdominal obesity in high school students from state public schools, Pernambuco, Brazil, 2014.
| Variables | Total=481 | |
|---|---|---|
| n | % | |
| Gender | ||
| Boys | 221 | 45.9 |
| Girls | 260 | 54.1 |
| Age (years) | ||
| 14–15 | 183 | 38.1 |
| 16–17 | 219 | 45.6 |
| 18–19 | 78 | 16.3 |
| Place of residence | ||
| Urban | 407 | 84.6 |
| Rural | 74 | 15.4 |
| Skin color | ||
| White | 128 | 26.7 |
| Non-white | 351 | 73.3 |
| Maternal education | ||
| >8 years of schooling | 47 | 11.6 |
| <8 years of schooling | 359 | 88.4 |
| Occupation | ||
| Works | 122 | 25.5 |
| Does not work | 357 | 74.5 |
| High blood pressure | ||
| No | 450 | 93.6 |
| Yes | 31 | 6.4 |
| Body mass index | ||
| Very low risk (≤18.6) | 121 | 25.2 |
| Low risk (18.7–20.6) | 120 | 24.9 |
| Moderate risk (20.7–23.4) | 120 | 24.9 |
| High risk (>23.5) | 120 | 24.9 |
| Waist circumference | ||
| Very low risk (≤69) | 136 | 28.3 |
| Low risk (69.1–73) | 108 | 22.5 |
| Moderate risk (73.1–80) | 123 | 25.6 |
| High risk (>80.1) | 114 | 23.7 |
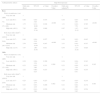
The prevalence of HBP was 6.4%, being higher among boys (9.0% vs. 4.7%, p<0.05). There was no significant difference between general (p=0.903) and abdominal (p=0.157) obesity when genders were compared, as shown in Fig. 1.
 and abdominal (WC>80.1) obesity and high blood pressure (percentile>95th) in high school students of both genders from state public schools, Pernambuco, Brazil, 2014. *p<0.05.")
After adjusting for age, as shown in Table 2, HBP was associated with general (OR=6.44; p=0.001) and abdominal (OR=6.97; p=0.001) obesity only in boys, when comparing the fourth quartile with the first quartile of the BMI (≤18.6kg/m2) vs. ≥23.5kg/m2) and waist circumference (≤69cm vs. ≥80.1cm).
Raw and adjusted odds ratio between high blood pressure and general and abdominal obesity (quartiles) in high school students of both genders, from state public schools, Pernambuco, Brazil, 2014.
| Anthropometric indices | High blood pressure | |||||||
|---|---|---|---|---|---|---|---|---|
| Odds ratio (Raw) | 95% CI | p-Value | Overall p-Value | Odds ratio (adjusteda) | 95% CI | p-Value | Overall p-Value | |
| Boys | ||||||||
| Waist circumference (cm) | ||||||||
| Very low risk (≤69) | 1 | <0.001 | 1 | <0.001 | ||||
| Low risk (69.1–73) | 0.46 | 0.04–5.26 | 0.535 | 0.38 | 0.03–4.40 | 0.439 | ||
| Moderate risk (73.1–80) | 1.75 | 0.31–10.00 | 0.526 | 1.31 | 0.22–7.76 | 0.765 | ||
| High risk (>80.1) | 7.93 | 1.69–37.18 | 0.009 | 6.97 | 1.47–33.15 | 0.015 | ||
| Body mass index (kg/m2) | ||||||||
| Very low risk (≤18.6) | 1 | <0.001 | 1 | <0.001 | ||||
| Low risk (18.7–20.6) | 0.46 | 0.04–5.19 | 0.527 | 0.38 | 0.03–4.43 | 0.442 | ||
| Moderate risk (20.7–23.4) | 2.70 | 0.50–14.59 | 0.247 | 2.31 | 0.42–12.73 | 0.337 | ||
| High risk (>23.5) | 7.57 | 1.60–35.70 | 0.011 | 6.44 | 1.33–31.04 | 0.020 | ||
| Girls | ||||||||
| Waist circumference (cm) | ||||||||
| Very low risk (≤69) | 1 | 0.260 | 1 | 0.245 | ||||
| Low risk (69.1–73) | 0.38 | 0.04–3.54 | 0.399 | 0.34 | 0.04–3.15 | 0.343 | ||
| Moderate risk (73.1–80) | 0.33 | 0.03–3.06 | 0.331 | 0.33 | 0.04–3.10 | 0.335 | ||
| High risk (>80.1) | 2.22 | 0.60–8.25 | 0.233 | 2.23 | 0.59–8.41 | 0.235 | ||
| Body mass index (kg/m2) | ||||||||
| Very low risk (≤18.6) | 1 | 0.462 | 1 | 0.463 | ||||
| Low risk (18.7–20.6) | 0.25 | 0.03–2.34 | 0.227 | 0.24 | 0.03–2.24 | 0.210 | ||
| Moderate risk (20.7–23.4) | 0.23 | 0.03–2.16 | 0.200 | 0.21 | 0.02–2.00 | 0.174 | ||
| High risk (>23.5) | 1.52 | 0.41–5.68 | 0.529 | 1.54 | 0.41–5.82 | 0.524 | ||
CI, confidence interval.
This study aimed to analyze the association between general and abdominal obesity with HBP in adolescents of both genders. The main findings were: (i) the prevalence of HBP was higher in boys; (ii) there was no significant difference between general and abdominal obesity when comparing genders; and (iii) HBP was associated with general and abdominal obesity only in boys.
The prevalence of HBP observed in this study was 6.4%, lower than that found in other studies with adolescents using the HBP>95th percentile as a criterion for HBP diagnosis.14,15,24–26 However, methodological differences, number of measurements, and the different reference criteria are the main causes of the great variability found in HBP prevalence among the investigations. In this study, the authors chose to use greater accuracy when diagnosing HBP, considering that a higher methodological stringency based on the hypertension guideline may result in a lower prevalence of HBP.27
As in other studies,14–16 boys had higher BP than girls. In this sense, studies using ambulatory BP monitoring techniques in children showed that with increasing age, there is an increase in blood pressure in both boys and girls; however, after puberty onset, BP in boys is higher than that of girls of the same age.28 Corroborating these findings, a longitudinal study of 1267 adolescents found that male adolescents were more likely to develop HBP in their lifetime.12
One of the major risk factors for hypertension is general obesity.2,16 A systematic review with meta-analysis showed that obese children had blood pressure levels approximately 40% higher than children with normal weight.2 Regarding body fat location, an association between general and abdominal obesity with HBP, through BMI and WC, was observed in a study with adolescents; however, sample stratification by gender was not performed at the analysis and the interaction between variables was not tested.24
Usually, there is a correlation between a possible increase in blood pressure in boys and a higher prevalence of fat accumulation in the abdominal region, but curiously, even with no difference between general and abdominal obesity when comparing genders, it was observed that the HBP was associated with general and abdominal obesity only in boys. These results are similar to those observed by Payeb et al.23 In a study carried out in Iran with 13,486 adolescents, those authors found a higher percentage of obesity in girls, although the HBP values were higher in boys.
A possible explanation for the higher HBP in boys is that sex hormones play an important role in BP regulation,29 as increased levels of gonadal hormones may occur during childhood and adolescence and these can modify the synthesis, release, and bioactivity of these factors, inducing vascular relaxation and consequently influencing BP.13 Moreover, Landazuri et al.30 verified that the levels of angiotensin-converting enzyme (ACE) were increased in boys aged 11–17 years, while they were decreased in girls of the same age group. ACE was the main enzyme of the renin-angiotensin system, which in turn plays an important role in heart function and BP regulation. The significant reduction in ACE activity observed in girls, but not in boys, indicates that estradiol and testosterone may have a diverse influence on angiotensin converting enzyme (ACE) activity in humans, particularly in relation to HBP.
The study has strengths and limitations that deserve to be mentioned. The cross-sectional design and the correlative nature of the data prevent us from establishing a causal association between HBP and obesity. Moreover, the adolescents’ maturational age, a point which may be related to hormonal release, was not assessed. Among the strengths, this study had a representative sample; the sampling procedures were established to ensure that the sample consisted of adolescent students that attended schools at different school shifts, and methodological stringency was employed when collecting BP data.
According to the data obtained during the study, it was observed that even with no difference in fat distribution between genders, general and abdominal obesity are associated with HBP only in boys, regardless of age. The results show the need to stratify the sample by gender when the aim is assessing BP in adolescents. Additionally, it was observed that HBP in boys may not be related to the prevalence of general and abdominal fat accumulation. In this sense, it is recommended to carry out studies using a longitudinal design to assess the influence of sex hormones on BP in adolescents.
FundingThe research was funded by Faculdade ASCES Scientific Initiation Program.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silva AO, Silva MV, Pereira LK, Feitosa WM, Ritti-Dias RM, Diniz PR, et al. Association between general and abdominal obesity with high blood pressure: difference between genders. J Pediatr (Rio J). 2016;92:174–80.
Study carried out at Faculdade Associação Caruaruense de Ensino Superior e Técnico (ASCES), Caruaru, PE, Brazil.





