

To identify the age of introduction of ultra-processed food and its associated factors among preschool children.
MethodsCross-sectional study carried out from March to June 2014 with 359 preschool children aged 17 to 63 months attending day-care centers. Time until ultra-processed food introduction (outcome variable) was described by the Kaplan–Meier analysis, and the log-rank test was used to compare the survival functions of independent variables. Factors associated with ultra-processed food introduction were investigated using the multivariate Cox proportional hazards model. The results were shown as hazard ratios with their respective 95% confidence intervals.
ResultsThe median time until ultra-processed food introduction was six months. Between the 3rd and 6th months, there is a significant increase in the probability of introducing ultra-processed food in the children's diet; and while the probability in the 3rd month varies from 0.15 to 0.25, at six months the variation ranges from 0.6 to 1.0. The final Cox proportional hazards model showed that unplanned pregnancy (1.32 [1.05–1.65]), absence of prenatal care (2.50 [1.02–6.16]), and income >2 minimum wages (1, 50 [1.09–2.06]) were independent risk factors for the introduction of ultra-processed food.
ConclusionUp to the 6th month of life, approximately 75% of preschool children had received one or more ultra-processed food in their diet. In addition, it was observed that the poorest families, as well as unfavorable prenatal factors, were associated with early introduction of ultra-processed food.
Identificar a idade e os fatores associados com a introdução de alimentos ultraprocessados (AUP) na alimentação de pré-escolares.
MétodosEstudo transversal realizado entre março e julho/2014 com 359 pré-escolares de 17 a 63 meses de idade matriculados em centros de educação infantil. O tempo até a introdução dos AUP (variável de desfecho) foi descrito por meio do estimador de Kaplan-Meiere o teste log-rank utilizado para comparar as funções de sobrevida das variáveis independentes. Por fim, analisou-se os fatores associados a introdução de AUP por meio de modelo múltiplo de riscos proporcionais de Cox. Os resultados foram apresentados como hazard ratios com seus respectivos intervalos de confiança de 95% (HR [IC95%]).
ResultadosA mediana de introdução de AUP foi de 6 meses. Entre o 3° e o 6° mês houve um incremento importante na probabilidade de introduzir AUP na alimentação das crianças; enquanto a probabilidade no 3° mês varia entre 0,15 e 0,25, no 6° mês a variação ocorre de 0,6 e 1,0. No modelo final de riscos proporcionais de Cox, identificamos que gravidez não desejada (1,32 [1,05–1,65]), não realização do pré-natal (2,50 [1,02–6,16]) e renda≥2 salários mínimos (1,50 [1,09–2,06]) se apresentaram como riscos independentes para a introdução de AUP.
ConclusãoIdentificamos que até o 6° mês de vida aproximadamente 75% dos pré-escolares já haviam recebido um ou mais AUP em sua alimentação. Além disso, observamos que as famílias mais pobres bem como fatores pré-natais desfavoráveis se associaram com a introdução precoce de AUP.
The first 1000 days of life, from conception to two years of age, are a fundamental period for an infant's full growth and development. It is recognized that exclusive breastfeeding (EBF) until the sixth month of life and the appropriate and timely introduction of foods1 contribute to health promotion, as well as physical and mental potentials, bringing benefits that are perpetuated not only in the short-term, but also in adult life.2
An inadequate diet from early childhood is among the modifiable risk factors for nutritional disorders, with worldwide repercussions in the context of public health: overweight, obesity, associated chronic diseases,3,4 and specific nutritional deficiencies,5 among which iron-deficient anemia, whose overall prevalence is 47.4% among preschoolers.5 In Brazil, 7.8% of preschool children have excess weight, and the annual percentage increase (1989–2006) is higher in the Northeast region (20.6%) than in the other macro-regions.6
This scenario is substantially derived from the lifestyle change process in contemporary society that have led to changes in the dietary pattern, characterized by the significant increase in the consumption of ultra-processed foods (UPF), which due to their formulation and presentation tend to be consumed in excess and to replace traditional foods.4,7
These foods have high energy density, high levels of free sugars, saturated and trans fats, sodium, and low supply of vitamins and minerals, contributing to the increase in overweight and its comorbidities.3,4 Furthermore, they are characterized by their extensive industrial processing (de-characterizing the food of origin) and inclusion of food additives.7 Thus, several researchers have tried to understand the factors that contribute to the early and continued consumption of UPF in different socioeconomic scenarios,8–11 aiming to subsidize strategies to curb the trend of uncontrolled UPF consumption.
Thus, the objective of this study was to identify the age and factors associated with the time of introduction of UPF in the diet of preschool children attending day-care centers (DCCs) in Maceió, state of Alagoas, Brazil.
MethodsStudy designA cross-sectional study entitled “Nutritional status of children in public day-care centers and dietary and nutrition actions in basic health care: an intersectoral approach”, conducted in the seventh sanitary district of Maceió, AL, Brazil, which is characterized by having the highest socioeconomic vulnerability of the municipality.
The study was carried out between March and July 2014 and included the DCCs (n=5) of the seventh district. All children enrolled in DCC (n=366) who did not have physical/motor or intellectual disabilities were considered eligible for the study. Of these, only two were not enrolled, due to refusal by the parents/guardians to authorize participation in the research, as well as five children whose parents/guardians did not attend the interview, comprising a total of 359 children of both genders, aged 17–63 months.
The evaluations and interviews were carried out by trained and supervised nutritionists, and the data obtained were entered in the Epi-Info 7 software (CDC – Atlanta, USA) with double independent typing and subsequent validation.
Studied variablesThe outcome variable was the time until the introduction of the UPF in the child's diet, considering the classification proposed by Monteiro et al.,7 obtained retrospectively through a structured questionnaire, which was constructed based on the following foods: bouillon cubes, processed meats, soft drinks and artificial juices, sandwich and plain cookies, petit-suisse cheese, industrial food thickeners, industrial baby food, snacks and chips, instant noodles, ice-cream, gelatin, sweets (candy, lollipops, and chocolate) and margarine. The time until the “event” was defined as the shortest interval between birth and the month when one of the previously listed UPF were introduced in the infant's diet.
Regarding the independent variables, those describing sociodemographic characteristics (maternal age, marital status, family income, and access to basic sanitation services), gestational characteristics (planned pregnancy, number of prenatal consultations, parity, and maternity leave), behavioral characteristics (breastfeeding, use of pacifiers and bottle feeding, complementary feeding characteristics, maternal perception of whether the child's diet outside of the DCC was healthy, and access to information on infant feeding), and biological antecedents (presence of anemia [hemoglobin<11mg/dL] and excess weight [Z-score of the body mass index-for-age index>+2D]), which are important factors in the nutritional analysis of populations, especially regarding the association of food patterns with the development of childhood obesity.
Data analysisThe generated database was converted to the Stata/IC 12.0 format (StataCorp LP, College Station, TX, USA), where all analyses were performed.
The time until the introduction of the UPF was described through the Kaplan–Meier estimator, which makes it possible to identify the cumulative conditional probability of the “event” as a function of a certain time interval (S(t)). However, to improve the interpretation of the analyses and graphical visualization of the curves, the estimator was used as 1−S(t), that is, the inverse of the accumulated survival function or accumulated failure function. Additionally, due to the low frequency of events between 12 and 36 months (n=10), observations were right-censored at 12 months.
The comparison between the functions of survival according to the selected independent variables was performed using the log-rank test. Finally, a multiple Cox proportional hazards model was constructed from the variables that showed p<0.20 in the log-rank test, adjusting the model for age at the time of the survey and gender. Risk proportionality assumption was assessed using the Schoenfeld test. The stepwise-forward method was used to introduce the variables into the multiple model, and the results are shown as hazard ratios with their respective 95% confidence intervals (HR [95% CI]).
Ethical aspectsThis study was submitted to and approved by the Research Ethics Committee of Universidade Federal de Alagoas (CAAE:18616313.8.0000.5013).
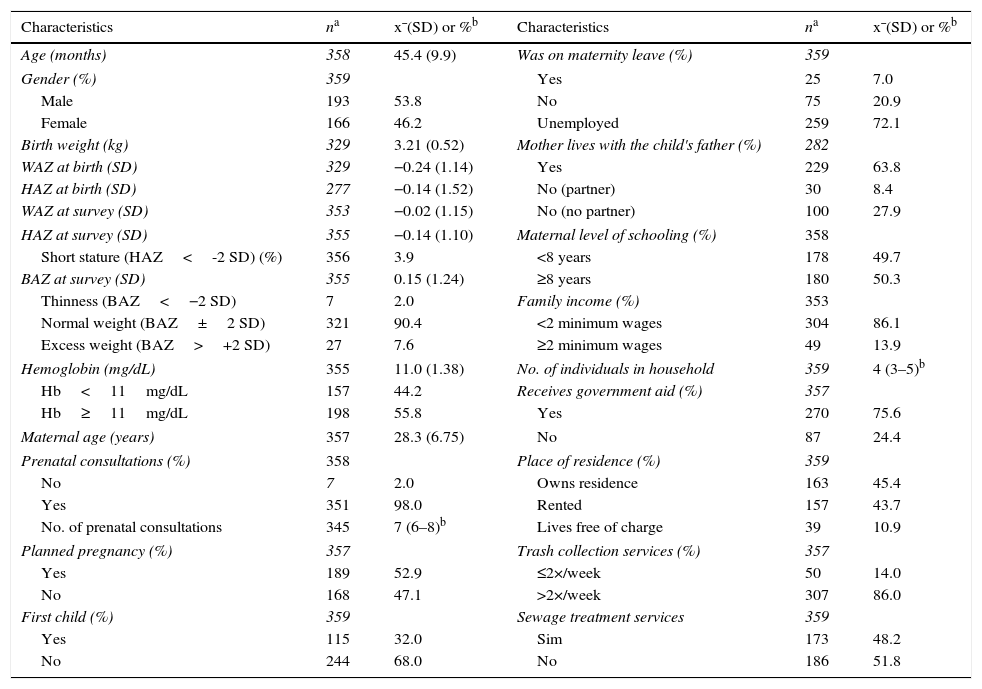
ResultsIn total, data were collected from 359 preschool children enrolled in the DCC of the seveth district of Maceió, AL. The mean age of the population was 45.4 months, with a similar frequency distribution between the genders. Among the nutritional deviations evaluated at the time of the survey, only excess weight was highlighted, with a prevalence of 7.6% (27/355; Table 1).
Individual, maternal and household characteristics of pre-school children attending day-care centers in Maceió, AL, Brazil, 2014.
| Characteristics | na | x¯(SD) or %b | Characteristics | na | x¯(SD) or %b |
|---|---|---|---|---|---|
| Age (months) | 358 | 45.4 (9.9) | Was on maternity leave (%) | 359 | |
| Gender (%) | 359 | Yes | 25 | 7.0 | |
| Male | 193 | 53.8 | No | 75 | 20.9 |
| Female | 166 | 46.2 | Unemployed | 259 | 72.1 |
| Birth weight (kg) | 329 | 3.21 (0.52) | Mother lives with the child's father (%) | 282 | |
| WAZ at birth (SD) | 329 | −0.24 (1.14) | Yes | 229 | 63.8 |
| HAZ at birth (SD) | 277 | −0.14 (1.52) | No (partner) | 30 | 8.4 |
| WAZ at survey (SD) | 353 | −0.02 (1.15) | No (no partner) | 100 | 27.9 |
| HAZ at survey (SD) | 355 | −0.14 (1.10) | Maternal level of schooling (%) | 358 | |
| Short stature (HAZ<-2 SD) (%) | 356 | 3.9 | <8 years | 178 | 49.7 |
| BAZ at survey (SD) | 355 | 0.15 (1.24) | ≥8 years | 180 | 50.3 |
| Thinness (BAZ<−2 SD) | 7 | 2.0 | Family income (%) | 353 | |
| Normal weight (BAZ±2 SD) | 321 | 90.4 | <2 minimum wages | 304 | 86.1 |
| Excess weight (BAZ>+2 SD) | 27 | 7.6 | ≥2 minimum wages | 49 | 13.9 |
| Hemoglobin (mg/dL) | 355 | 11.0 (1.38) | No. of individuals in household | 359 | 4 (3–5)b |
| Hb<11mg/dL | 157 | 44.2 | Receives government aid (%) | 357 | |
| Hb≥11mg/dL | 198 | 55.8 | Yes | 270 | 75.6 |
| Maternal age (years) | 357 | 28.3 (6.75) | No | 87 | 24.4 |
| Prenatal consultations (%) | 358 | Place of residence (%) | 359 | ||
| No | 7 | 2.0 | Owns residence | 163 | 45.4 |
| Yes | 351 | 98.0 | Rented | 157 | 43.7 |
| No. of prenatal consultations | 345 | 7 (6–8)b | Lives free of charge | 39 | 10.9 |
| Planned pregnancy (%) | 357 | Trash collection services (%) | 357 | ||
| Yes | 189 | 52.9 | ≤2×/week | 50 | 14.0 |
| No | 168 | 47.1 | >2×/week | 307 | 86.0 |
| First child (%) | 359 | Sewage treatment services | 359 | ||
| Yes | 115 | 32.0 | Sim | 173 | 48.2 |
| No | 244 | 68.0 | No | 186 | 51.8 |
x¯, mean; SD, standard deviation; %, frequency; WAZ, weight-for-age Z-score; HAZ, height-for-age Z-score; BAZ, BMI-for-age Z-score.
One-third of the study population consisted of firstborns, and although the number of mothers was small, all those who did not attended prenatal care consultations indicated that the pregnancy was unwanted. Still in relation to maternal characteristics, 50.3% (180/358) of the mothers had more than eight years of schooling and approximately 65% (229/282) lived with the child's biological father (Table 1).
The socioeconomic status and housing conditions of the study population can be characterized as low income, since 86% (304/353) lived with less than two Brazilian minimum wages (MW)/month, the median of the household residents was four individuals, 75.6% (270/357) received some form of government aid, and half of the households (186/359) did not have adequate sewage treatment services (Table 1).
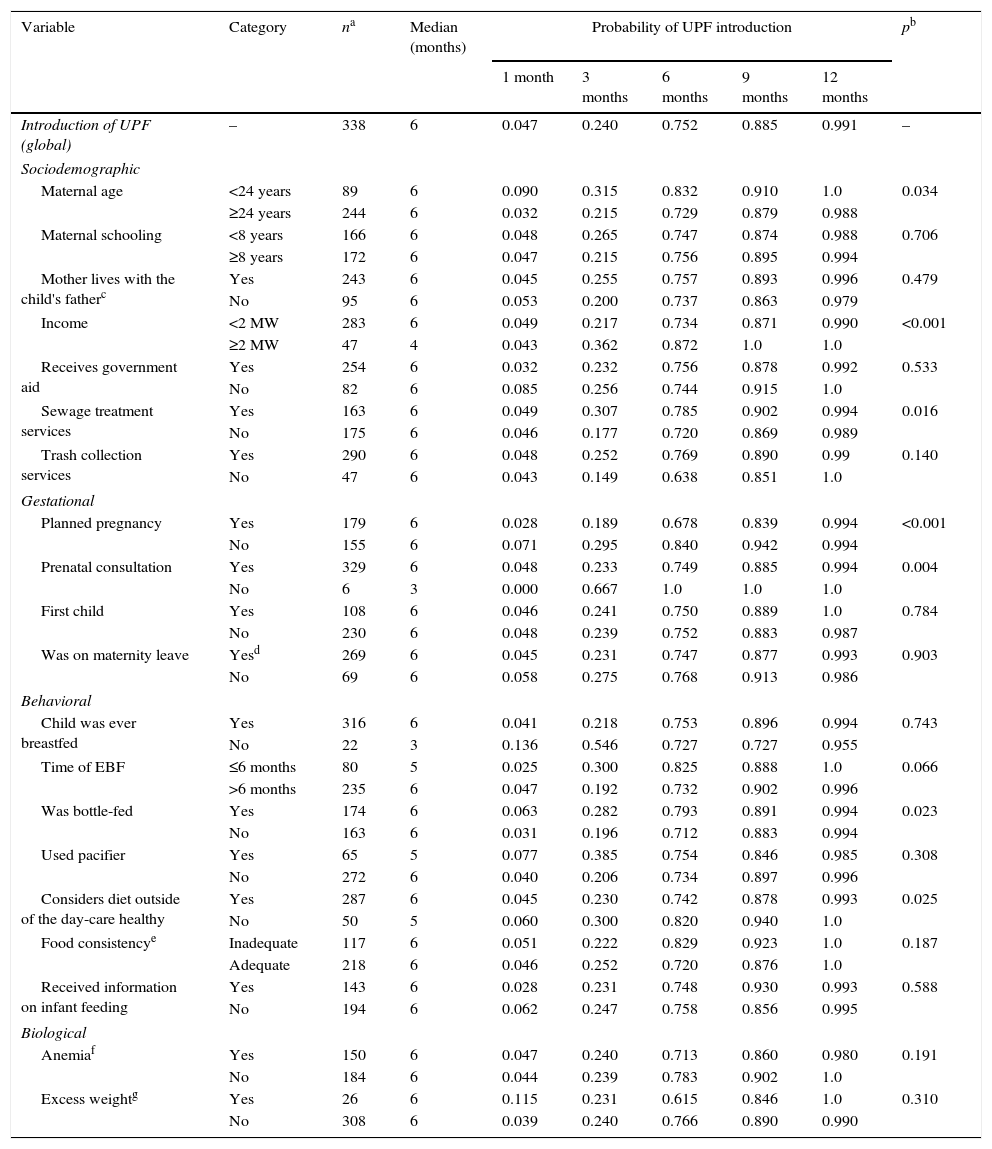
In the overall analysis, the median time to UPF introduction was six months. However, it is important to note that between the third and the sixth months of life, there is a significant increase in the probability of introducing UPF in the children's diet; while the probability in the third month ranges from 0.15 to 0.25, in the sixth month it ranges from 0.6 to 1.0 (Table 2). Moreover, it was observed that this increase in the probability of UPF introduction in the diet occurs mainly from the fifth to the sixth months. This finding is shown in Table 2; regardless of the selected variable, the median time to UPF introduction is six months, but the probability is ∼0.75, that is, the probability in the fifth month is <0.50. Fig. 1 shows the Kaplan–Meier curves of variables associated with UPF introduction.
Median and cumulative probability of the time until the introduction of ultra processed foods among preschoolers attending day-care centers in Maceió, AL, Brazil, 2014.
| Variable | Category | na | Median (months) | Probability of UPF introduction | pb | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1 month | 3 months | 6 months | 9 months | 12 months | |||||
| Introduction of UPF (global) | – | 338 | 6 | 0.047 | 0.240 | 0.752 | 0.885 | 0.991 | – |
| Sociodemographic | |||||||||
| Maternal age | <24 years | 89 | 6 | 0.090 | 0.315 | 0.832 | 0.910 | 1.0 | 0.034 |
| ≥24 years | 244 | 6 | 0.032 | 0.215 | 0.729 | 0.879 | 0.988 | ||
| Maternal schooling | <8 years | 166 | 6 | 0.048 | 0.265 | 0.747 | 0.874 | 0.988 | 0.706 |
| ≥8 years | 172 | 6 | 0.047 | 0.215 | 0.756 | 0.895 | 0.994 | ||
| Mother lives with the child's fatherc | Yes | 243 | 6 | 0.045 | 0.255 | 0.757 | 0.893 | 0.996 | 0.479 |
| No | 95 | 6 | 0.053 | 0.200 | 0.737 | 0.863 | 0.979 | ||
| Income | <2 MW | 283 | 6 | 0.049 | 0.217 | 0.734 | 0.871 | 0.990 | <0.001 |
| ≥2 MW | 47 | 4 | 0.043 | 0.362 | 0.872 | 1.0 | 1.0 | ||
| Receives government aid | Yes | 254 | 6 | 0.032 | 0.232 | 0.756 | 0.878 | 0.992 | 0.533 |
| No | 82 | 6 | 0.085 | 0.256 | 0.744 | 0.915 | 1.0 | ||
| Sewage treatment services | Yes | 163 | 6 | 0.049 | 0.307 | 0.785 | 0.902 | 0.994 | 0.016 |
| No | 175 | 6 | 0.046 | 0.177 | 0.720 | 0.869 | 0.989 | ||
| Trash collection services | Yes | 290 | 6 | 0.048 | 0.252 | 0.769 | 0.890 | 0.99 | 0.140 |
| No | 47 | 6 | 0.043 | 0.149 | 0.638 | 0.851 | 1.0 | ||
| Gestational | |||||||||
| Planned pregnancy | Yes | 179 | 6 | 0.028 | 0.189 | 0.678 | 0.839 | 0.994 | <0.001 |
| No | 155 | 6 | 0.071 | 0.295 | 0.840 | 0.942 | 0.994 | ||
| Prenatal consultation | Yes | 329 | 6 | 0.048 | 0.233 | 0.749 | 0.885 | 0.994 | 0.004 |
| No | 6 | 3 | 0.000 | 0.667 | 1.0 | 1.0 | 1.0 | ||
| First child | Yes | 108 | 6 | 0.046 | 0.241 | 0.750 | 0.889 | 1.0 | 0.784 |
| No | 230 | 6 | 0.048 | 0.239 | 0.752 | 0.883 | 0.987 | ||
| Was on maternity leave | Yesd | 269 | 6 | 0.045 | 0.231 | 0.747 | 0.877 | 0.993 | 0.903 |
| No | 69 | 6 | 0.058 | 0.275 | 0.768 | 0.913 | 0.986 | ||
| Behavioral | |||||||||
| Child was ever breastfed | Yes | 316 | 6 | 0.041 | 0.218 | 0.753 | 0.896 | 0.994 | 0.743 |
| No | 22 | 3 | 0.136 | 0.546 | 0.727 | 0.727 | 0.955 | ||
| Time of EBF | ≤6 months | 80 | 5 | 0.025 | 0.300 | 0.825 | 0.888 | 1.0 | 0.066 |
| >6 months | 235 | 6 | 0.047 | 0.192 | 0.732 | 0.902 | 0.996 | ||
| Was bottle-fed | Yes | 174 | 6 | 0.063 | 0.282 | 0.793 | 0.891 | 0.994 | 0.023 |
| No | 163 | 6 | 0.031 | 0.196 | 0.712 | 0.883 | 0.994 | ||
| Used pacifier | Yes | 65 | 5 | 0.077 | 0.385 | 0.754 | 0.846 | 0.985 | 0.308 |
| No | 272 | 6 | 0.040 | 0.206 | 0.734 | 0.897 | 0.996 | ||
| Considers diet outside of the day-care healthy | Yes | 287 | 6 | 0.045 | 0.230 | 0.742 | 0.878 | 0.993 | 0.025 |
| No | 50 | 5 | 0.060 | 0.300 | 0.820 | 0.940 | 1.0 | ||
| Food consistencye | Inadequate | 117 | 6 | 0.051 | 0.222 | 0.829 | 0.923 | 1.0 | 0.187 |
| Adequate | 218 | 6 | 0.046 | 0.252 | 0.720 | 0.876 | 1.0 | ||
| Received information on infant feeding | Yes | 143 | 6 | 0.028 | 0.231 | 0.748 | 0.930 | 0.993 | 0.588 |
| No | 194 | 6 | 0.062 | 0.247 | 0.758 | 0.856 | 0.995 | ||
| Biological | |||||||||
| Anemiaf | Yes | 150 | 6 | 0.047 | 0.240 | 0.713 | 0.860 | 0.980 | 0.191 |
| No | 184 | 6 | 0.044 | 0.239 | 0.783 | 0.902 | 1.0 | ||
| Excess weightg | Yes | 26 | 6 | 0.115 | 0.231 | 0.615 | 0.846 | 1.0 | 0.310 |
| No | 308 | 6 | 0.039 | 0.240 | 0.766 | 0.890 | 0.990 | ||
MW, minimum wage; UPF, ultraprocessed food; EBF, exclusive breastfeeding.

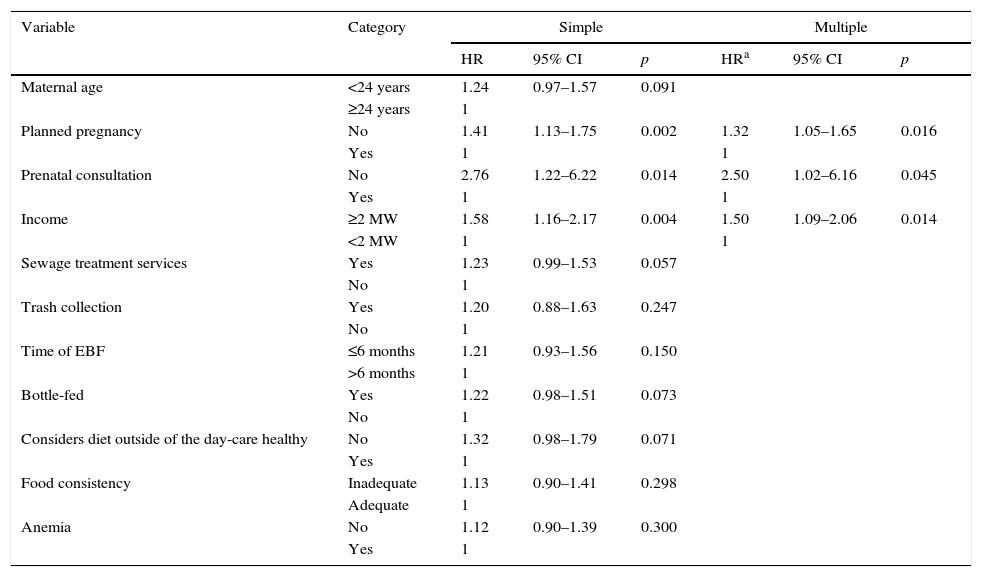
In the final Cox proportional hazards model, it was observed that unwanted pregnancy (1.32 [1.05–1.65]), absence of prenatal care (2.50 [1.02–6.16]), and income ≥2MW (1.50 [1.09–2.06]) were independent risks for the early introduction of UPF in the preschool children's diet (Table 3).
Simple and multiple analyses of Cox proportional hazards for ultra processed food introduction among preschoolers attending day-care centers in Maceió, AL, Brazil, 2014.
| Variable | Category | Simple | Multiple | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HRa | 95% CI | p | ||
| Maternal age | <24 years | 1.24 | 0.97–1.57 | 0.091 | |||
| ≥24 years | 1 | ||||||
| Planned pregnancy | No | 1.41 | 1.13–1.75 | 0.002 | 1.32 | 1.05–1.65 | 0.016 |
| Yes | 1 | 1 | |||||
| Prenatal consultation | No | 2.76 | 1.22–6.22 | 0.014 | 2.50 | 1.02–6.16 | 0.045 |
| Yes | 1 | 1 | |||||
| Income | ≥2 MW | 1.58 | 1.16–2.17 | 0.004 | 1.50 | 1.09–2.06 | 0.014 |
| <2 MW | 1 | 1 | |||||
| Sewage treatment services | Yes | 1.23 | 0.99–1.53 | 0.057 | |||
| No | 1 | ||||||
| Trash collection | Yes | 1.20 | 0.88–1.63 | 0.247 | |||
| No | 1 | ||||||
| Time of EBF | ≤6 months | 1.21 | 0.93–1.56 | 0.150 | |||
| >6 months | 1 | ||||||
| Bottle-fed | Yes | 1.22 | 0.98–1.51 | 0.073 | |||
| No | 1 | ||||||
| Considers diet outside of the day-care healthy | No | 1.32 | 0.98–1.79 | 0.071 | |||
| Yes | 1 | ||||||
| Food consistency | Inadequate | 1.13 | 0.90–1.41 | 0.298 | |||
| Adequate | 1 | ||||||
| Anemia | No | 1.12 | 0.90–1.39 | 0.300 | |||
| Yes | 1 | ||||||
HR, hazard ratio; 95% CI, 95% confidence interval; MW, minimum wage; EBF, exclusive breastfeeding.
This study aimed to analyze the age of introduction of UPF in preschool children's diet enrolled in the DCCs of the region with the greatest social vulnerability of the capital of the state of Alagoas. The economic characteristics and those prior to the child's birth were shown to be important factors for the early introduction of UPF; furthermore, it was observed that the critical period for the introduction of these foods occurred between the third and fifth months of life.
Another important aspect to be highlighted is that the present study was the first to analyze the introduction of UPF through the Kaplan–Meier estimator and Cox proportional hazards model, which, in this context, had been used only for analysis of the partial or total interruption of breastfeeding. Similar approaches were identified in the literature; however, they focused on the time for the introduction of supplementary feeding as a whole, without specifying a group of foods that are known to be deleterious to health, such as the analyses carried out by Boudet-Berquier et al.12 Therefore, the present study objectively identified the onset of a food behavior that is considered unhealthy, which allows the planning of actions aimed at changing this modifiable risk factor.
Conversely, it is important to note that the main limitation of the present study was the recall bias, which is inherent in cross-sectional research, regarding the information about the introduction of UPF in the diet of preschoolers while still infants, which could occur differently depending on the amplitude of the age range of the assessed children (17–63 months). However, even if the accuracy of the information is lower than those prospectively collected, this limitation is minimized by the proximity between the event of interest and the child's age at the time of the survey.
The construction of eating habits begins in the first two years of life, with a profound impact in subsequent years, since it is during this period that children discover the sensory (texture, taste, and smell), nutritional (self-regulation of consumption based on the energy density of foods), and behavioral characteristics (definition of time and environment) related to foods and the eating habits.13 It is currently a consensus that UPF should be avoided in the first years of life and consumed with restrictions in all other phases, as they contribute to a significant increase in the daily energy intake due to its excessive content of refined sugars and saturated fat; additionally, they have high sodium density and food additives and reduced contents of micronutrients and dietary fiber.14
The increased and chronic consumption of this group of foods has clinical and biochemical consequences to children's health in the short term, such as obesity and changes in the lipoprotein profile, representing an early risk for the development of chronic non-communicable diseases.15 A study by Pan et al.11 with North-American children followed-up from the last gestational trimester until 6 years of age, demonstrated that the child's chance of becoming obese was 92% higher in those who consumed sugary drinks in the first semester of life, when compared with those who did not. In the same perspective, Rauber et al.15 demonstrated an association between the consumption of these foods and an increase in total cholesterol and LDL levels from preschool to school age.
Another aspect that cannot be neglected in this scenario is the negative impact on culture (devaluation of local food practices and of the relationship of the population with food), social life (loss of commensality aspects and sharing of meals, since the products are intended for individual consumption and can be consumed in any place, dispensing with the need to dedicate a period to live the social experience of food), and the environment (threat on the sustainability of the planet, from the production and disposal of the packaging, through the extensive monocultures dependent on transgenic seeds, the aggressive use of agrochemicals, chemical fertilizers, and water, to logistics distribution channels, increasing pollution levels due to the scarcity of highly energy-efficient transportation systems).15,16
Although the harms associated with such eating behavior are clear, this situation does not appear to be resolving in Brazil, as well as in the rest of the world, since global trends indicate the increase of UPF consumption, especially among children, in different geographic and socioeconomic scenarios.9–12
In an ecological analysis, Moodie et al.17 accumulated trends regarding the acquisition of UPF in countries of different economic statuses, showing an annual growth of the consumed per capita volume equivalent to 2.0% in low- and middle-income countries and 1.4% in high-income countries between 1997 and 2009; as a result of this increase, 75% of the world's food sales comprise processed or UPF, 1/3 of which is controlled by transnational corporations. In Brazil, the main companies/conglomerates involved in the production and sale of these foods, including those for children, are Nestlé, Brazil Foods, Kraft Foods, Unilever, and Danone.17
Aiming to address this situation, the literature highlights the introduction of taxes on unhealthy foods and subsidies on foods considered to be healthy as a potential strategy.18 For instance, Hungary has imposed a tax on foods high in sugar, sodium or caffeine; France, which imposed a tax on soft drinks, or Finland, on confectionery products.19 Mexico, which has the second-highest obesity rate worldwide, has introduced taxes on sweetened beverages and foods rich in saturated fat, sugar, and sodium.20
In addition, it is necessary to focus on efforts to increase the availability of fruits and vegetables, with sale points located in small and large towns, including peripheral neighborhoods, which favors the more frequent purchase of perishable foods.21 In Brazil, there are no special taxation or pricing schemes on foods that aim to discourage UPF consumption.
Therefore, considering the biological, social, and economic consequences of the early and continuous consumption of UPF, it is urgent that health professionals involved in primary care take action in relation to this problem, adding dietary information to the child care guidelines provided during the prenatal care and the puerperium periods.1,22 It is important to note that, within this context, the potential beneficial effect of breastfeeding on maintaining a healthy weight gain and preventing excess weight can be reduced in the presence of unhealthy eating patterns.6,23
Among the variables associated with the introduction of UPF, those related to prenatal care access, planned/unplanned pregnancy, and family income were identified as most relevant.
Although there has been an increase in prenatal care coverage in Brazil since the 1990s,24 inequalities in the access to health care services persist, and women with lower levels of education and income, as well as those living in the North and Northeast regions have less access to prenatal care.25 As a consequence, data on a birth cohort from Recôncavo Baiano showed that, in the absence of prenatal care, there was a 173% increase in the risk of shorter EBF duration and 38% in the risk of breastfeeding discontinuation.
Regarding the socioeconomic status, similar findings were identified in a cohort in Diamantina, in the state of Minas Gerais, which concluded that the children of mothers with higher per capita income (>1/2 MW) had twice the chance, when compared to those with lower income, of consuming unhealthy foods more frequently.26 Nonetheless, relativization is worthwhile, considering the geographic and social contexts of the role of higher income in the consumption of unhealthy foods, since in the comparison between high and low income families, UPF consumption was significantly higher among the wealthiest individuals.23 Therefore, within groups with lower purchasing power, the higher the income, the greater the consumption; however, this statement is not true in the comparison between very different economic classes.
The interpretation and use of the results should be made with caution and considering the multifactorial nature of the dietary behavior formation process – which reflects in the magnitude of the associations observed in the multiple Cox model. In the case of the association between an unwanted pregnancy and the early introduction of UPF, this variable was a negative factor for health outcomes,27,28 which in turn suggests its association with the maternal disinterest for information related to childcare, in this context, about adequate and healthy food. Conversely, this question only accounts for the mother's initial intention, and not to the maintenance of this position in relation to the pregnancy. The mother might not have wanted the pregnancy; however, this does not imply in a negative reaction toward this new condition by herself and the family.
Therefore, within a scenario of high socioeconomic vulnerability, the present study suggests that access to health care services (prenatal consultations) has an important role in the delay of the introduction of UPF, which may be directly related to the increase in the duration of the EBF. Additionally, the 95% CI variability may provide another interpretation of the phenomenon, indicating the effect not only of the access to prenatal care, but also of its quality. Thus, the authors emphasize the relevance of the humanized contact between healthcare professionals and the pregnant woman, identifying her perception about the pregnancy, to provide comprehensive care.
Finally, in a case-control study carried out in Maceió, it was observed that children whose mothers were followed at the Basic Health Units of the Brazilian Unified Healthcare System had a significantly higher median score of industrialized food consumption than those followed-up in private clinics. However, this difference was not necessarily due to the quality of the service provided (whose data is not available), but probably due to the social gap found in the municipality, reflected in the differences between the levels of education of those responsible for the child, family income, and vulnerability to media influence.29
Considering the objectives of the present study, it can be concluded that the median time until the introduction of UPF was six months; however, when they reached this age, ∼75% of preschoolers had already received one or more UPFs in their diets. Additionally, it was observed that an unplanned pregnancy, prenatal consultations, and family income <2 MWs were associated with the early introduction of UPF in the diet of preschoolers attending DCCs in Maceió. Therefore, the present results are in line with the increasing body of evidence that indicates the prenatal period as an appropriate moment to carry out nutritional and dietary education strategies, aiming not only to prolong breastfeeding time, but also to introduce healthy and adequate complementary feeding.
FundingFundação de Amparo à Pesquisa do Estado de Alagoas (FAPEAL), Process no. 60030000692/2013.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Longo-Silva G, Silveira JA, Menezes RC, Toloni MH. Age at introduction of ultra-processed food among preschool children attending day-care centers. J Pediatr (Rio J). 2017;93:508–16.
Study developed at Universidade Federal de Alagoas (UFAL), Faculdade de Nutrição (FANUT), Programa de Pós-Graduação em Nutrição, Maceió, AL, Brazil.




