
To validate the Brazilian Portuguese version of the Family Environment Assessment questionnaire (Inventaire du Milieu Familial).
MethodsThe validation process was carried out in two stages. First, translation and back-translation were performed, and in the second phase, the questionnaire was applied in 72 families of children between 0 and 24 months for the validation process. The tool consists of the following domains: mother's communication ability; behavior; organization of the physical and temporal environment; collection/quantity of toys; maternal attitude of constant attention toward her baby; diversification of stimuli; baby's behavior. The following was performed for the scale validation: 1 – content analysis (judgment); 2 – construct analysis (factorial analysis – Kaiser-Meyer-Olkin, Bartlett, and Pearson's correlation tests); 3 – criterion analysis (calculation of Cronbach's alpha coefficient, intraclass correlations, and split-half correlations).
ResultsThe mean age of the children was 9±6.7 months, and of these, 35 (48.6%) were males. Most correlations between items and domains were significant. In the factorial analysis of the scale, Kaiser-Meyer-Olkin values were 0.76, Bartlett's test showed a p-value<0.001, and correlation between items and domains showed a p-value<0.01. Regarding the validity, Cronbach's alpha was 0.92 (95% CI: 0.89–0.94). The intraclass correlation among the evaluators was 0.97 (0.96–0.98) and split-half correlations, r: 0.60, with p<0.01.
ConclusionsThe Portuguese version of the Inventaire du Milieu Familial showed good to excellent performance regarding the assessed psychometric properties.
Validar a versão em português do Questionário de Avaliação do Ambiente Familiar (Inventaire du Milieu Familial).
MétodosO processo de validação foi feito em duas etapas. Primeiramente, realizou-se a tradução e retrotradução e, na segunda fase, o questionário foi aplicado em 72 famílias de crianças entre zero e 24 meses para o processo de validação. O instrumento é formado pelos seguintes domínios: Capacidade de comunicação da mãe; Comportamento; Organização do ambiente físico e temporal; Acervo/quantidade de brinquedos; Implicação da mãe com seu bebê; Diversificação de estímulos; Comportamento do bebê. Para a validação da escala foi realizada: 1- análise de conteúdo (julgamento); 2- análise de construto (análise fatorial - testes Kaiser-Meyer-Olkin, Bartlett e correlação de Pearson); 3- análise de critério (cálculo do coeficiente alfa de cronbach, correlações intraclasse e correlações split-half).
ResultadosA média de idade das crianças foi 9±6,7 meses e, dessas, 35 (48,6%) eram do sexo masculino. A maioria das correlações entre os itens e os domínios foi significativa. Na análise fatorial da escala, os valores de Kaiser-Meyer-Olkin foram 0,76, teste de Bartlett com p<0,001 e correlação entre os itens e domínios p<0,01. Em relação à validade, o alfa de Cronbach foi de 0,92 (IC 95% 0,89-0,94). A correlação intraclasse entre os avaliadores foi de 0,97 (0,96-0,98) e correlações split-half r: 0,60 p<0,01.
ConclusõesA versão portuguesa do Inventaire du Milieu Familial apresentou um bom à excelente desempenho nas propriedades psicométricas avaliadas.
The impact of the environment on the first years of life has been associated to human development. Studies in epigenetics have demonstrated an association between prenatal and postnatal adversities, with the development of diseases in the adult phase, such as depression, diabetes, obesity, aggressiveness, drug abuse, and early mortality.1 Studying the impact of the family environment on child development is of utmost importance, since environmental mechanisms can be rapidly modified and early interventions have shown lasting beneficial effects on the individuals’ health.2,3
Exposure during childhood to stressor factors results in progressive changes in gene expression, known as DNA methylation.3–7 DNA changes are associated with increased risk of unfavorable outcomes in childhood and adulthood, and may be manifested by changes in mental health, language, cognitive and brain development, and behavior.4–7 However, a favorable family environment, where children receive adequate stimuli to their development in early childhood, has shown a reduction in deleterious effects in the long term.4
Several tools that use quantitative and qualitative scales to measure the stimulus offered to the child in the family environment are available in the literature8,9 but have not yet been adapted for the Brazilian population. Among the tools used internationally is the Family Environment Assessment – (Inventaire du Milieu Familial [IMF]) questionnaire, which was first used in Canada in 19988 in its French-language version, validated and adapted from the American Home Observation for Measurement of the Environment (HOME) questionnaire.9 This tool has been widely used by researchers worldwide, and its association with child cognitive and social development is well documented.10
In Canada, the IMF, in its 2002 updated version, has been used for more than fifteen years in longitudinal studies with emphasis on child development, and has become an important tool for analyzing the family environment. In Brazil, there are no validated questionnaires similar to the IMF to assess the inclusion of infants and children in this context. The main objective of this questionnaire is to evaluate the quality and quantity of stimulus provided by the caregiver for the child's development. Moreover, it evaluates the applied parental techniques, the family environment, and the caregiver's behavior toward the child at home.8,11
Considering the need to provide a tool adapted to the particularities of the Brazilian population, that can assess child development and its inclusion in the family context, the main objective of this study was to validate the Portuguese version of the IMF. The choice of validation of this questionnaire is due to the fact that the authors are developing a study in Brazil with monozygotic twins in partnership with Canada, which uses the IMF. The IMF is a tool equivalent to the HOME questionnaire.
MethodsThis was a cross-sectional study for the validation of the IMF (French version of the Infant/Toddler HOME). In the period from July 2015 to May 2016, families of children of different social classes, ranging in age from zero to 24 months of age, of both genders, were included for convenience. The families participated in the study after signing the Informed Consent, and the research was carried out through home visits.
The IMF consists of 32 items, divided into seven domains. Domain A (mother's ability to communicate) consists of eleven questions that assess the development of the language offered to the child and the caregiver's communication ability with the child and the interviewer. Domain B (behavior) deals with restriction or punishment during the interview, including six questions about possible verbal or physical aggressions. Domain C (organization of the physical and temporal environment) consists of five questions and deals with the organization of the physical environment, the presence of pets, and the degree of activity in the household. In domain D (collection/quantity of appropriate toys), the interviewer must inquire about the number and quality of the toys offered to the child. Domain E (mother's fussy attitude toward her baby) includes questions about the mother's attitudes toward the baby, that is, if the child is kept within the maternal field of vision and whether it is stimulated in its development process. In domain F (stimulus diversification), information is collected on the number of people present in the household at the time of the tool application. Finally, in domain G (baby's behavior), the evaluator reports on the child's behavior during the application of the tool.
Most items (75%) are answered similarly, using a 6-point Likert scale, in which 1 is never, 2 is rarely, 3 is sometimes, 4 is often, 5 is always, and 6 is baby/twin is absent or sleeping.
The validation process was carried out in two phases: Phase One – translation process of the tool. Phase Two – field validation (testing of psychometric properties).
Phase One: This phase was carried out according to international recommendations for tool validations,12 which includes the following steps: 1 – translation by two French-Portuguese speaking translators; 2 – Harmonization between both versions, resulting in a single Portuguese version; 3 – Back-translation of the harmonized version initially, by two Portuguese-French translators; 4 – Harmonization between both translators, resulting in a single French version; 5 – General harmonization, where the resulting versions of the first and second harmonization are discussed by the four translators, aiming to obtain a consensus version. The last stage of the first phase consisted of application of the scale. The IMF scale was applied to ten participants in order to evaluate their understanding and include possible participants’ suggestions.
Phase Two – The validation of the IMF tool was carried out, through the analysis of content, construct, and criteria.
For content analysis (judgment), a team of health professionals analyzed the representativeness of the items in relation to content areas and the relevance of the objectives to be measured in the scale.
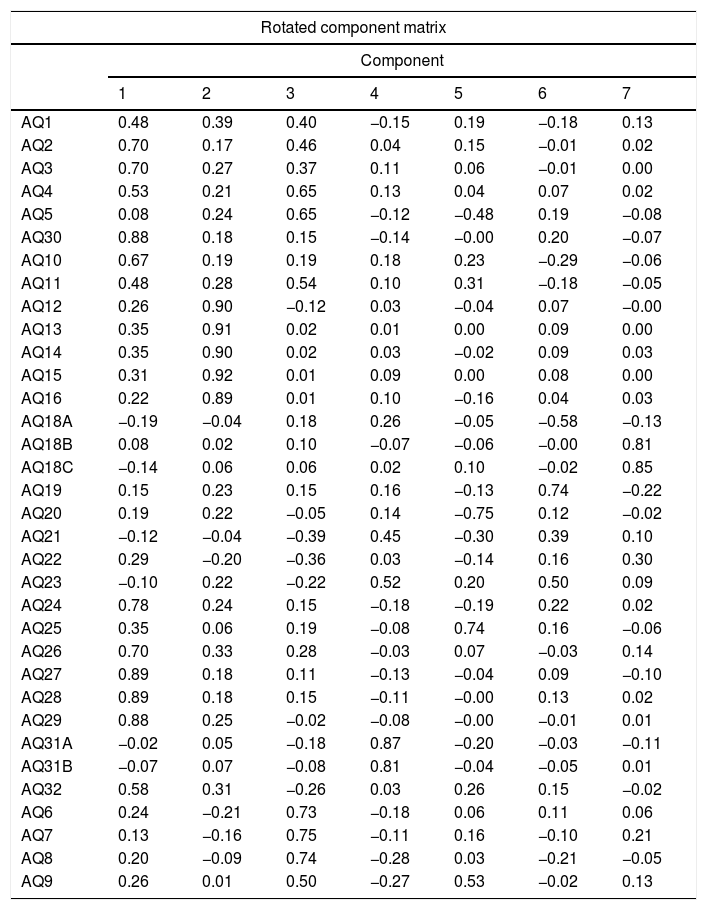
For the construct analysis, the factorial analysis of the questionnaire was performed using the following tests: Kaiser-Meyer-Olkin (KMO – Table 1), Bartlett's test, and Pearson's correlation.
Kaiser-Meyer-Olkin (KMO) test.
| Rotated component matrix | |||||||
|---|---|---|---|---|---|---|---|
| Component | |||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| AQ1 | 0.48 | 0.39 | 0.40 | −0.15 | 0.19 | −0.18 | 0.13 |
| AQ2 | 0.70 | 0.17 | 0.46 | 0.04 | 0.15 | −0.01 | 0.02 |
| AQ3 | 0.70 | 0.27 | 0.37 | 0.11 | 0.06 | −0.01 | 0.00 |
| AQ4 | 0.53 | 0.21 | 0.65 | 0.13 | 0.04 | 0.07 | 0.02 |
| AQ5 | 0.08 | 0.24 | 0.65 | −0.12 | −0.48 | 0.19 | −0.08 |
| AQ30 | 0.88 | 0.18 | 0.15 | −0.14 | −0.00 | 0.20 | −0.07 |
| AQ10 | 0.67 | 0.19 | 0.19 | 0.18 | 0.23 | −0.29 | −0.06 |
| AQ11 | 0.48 | 0.28 | 0.54 | 0.10 | 0.31 | −0.18 | −0.05 |
| AQ12 | 0.26 | 0.90 | −0.12 | 0.03 | −0.04 | 0.07 | −0.00 |
| AQ13 | 0.35 | 0.91 | 0.02 | 0.01 | 0.00 | 0.09 | 0.00 |
| AQ14 | 0.35 | 0.90 | 0.02 | 0.03 | −0.02 | 0.09 | 0.03 |
| AQ15 | 0.31 | 0.92 | 0.01 | 0.09 | 0.00 | 0.08 | 0.00 |
| AQ16 | 0.22 | 0.89 | 0.01 | 0.10 | −0.16 | 0.04 | 0.03 |
| AQ18A | −0.19 | −0.04 | 0.18 | 0.26 | −0.05 | −0.58 | −0.13 |
| AQ18B | 0.08 | 0.02 | 0.10 | −0.07 | −0.06 | −0.00 | 0.81 |
| AQ18C | −0.14 | 0.06 | 0.06 | 0.02 | 0.10 | −0.02 | 0.85 |
| AQ19 | 0.15 | 0.23 | 0.15 | 0.16 | −0.13 | 0.74 | −0.22 |
| AQ20 | 0.19 | 0.22 | −0.05 | 0.14 | −0.75 | 0.12 | −0.02 |
| AQ21 | −0.12 | −0.04 | −0.39 | 0.45 | −0.30 | 0.39 | 0.10 |
| AQ22 | 0.29 | −0.20 | −0.36 | 0.03 | −0.14 | 0.16 | 0.30 |
| AQ23 | −0.10 | 0.22 | −0.22 | 0.52 | 0.20 | 0.50 | 0.09 |
| AQ24 | 0.78 | 0.24 | 0.15 | −0.18 | −0.19 | 0.22 | 0.02 |
| AQ25 | 0.35 | 0.06 | 0.19 | −0.08 | 0.74 | 0.16 | −0.06 |
| AQ26 | 0.70 | 0.33 | 0.28 | −0.03 | 0.07 | −0.03 | 0.14 |
| AQ27 | 0.89 | 0.18 | 0.11 | −0.13 | −0.04 | 0.09 | −0.10 |
| AQ28 | 0.89 | 0.18 | 0.15 | −0.11 | −0.00 | 0.13 | 0.02 |
| AQ29 | 0.88 | 0.25 | −0.02 | −0.08 | −0.00 | −0.01 | 0.01 |
| AQ31A | −0.02 | 0.05 | −0.18 | 0.87 | −0.20 | −0.03 | −0.11 |
| AQ31B | −0.07 | 0.07 | −0.08 | 0.81 | −0.04 | −0.05 | 0.01 |
| AQ32 | 0.58 | 0.31 | −0.26 | 0.03 | 0.26 | 0.15 | −0.02 |
| AQ6 | 0.24 | −0.21 | 0.73 | −0.18 | 0.06 | 0.11 | 0.06 |
| AQ7 | 0.13 | −0.16 | 0.75 | −0.11 | 0.16 | −0.10 | 0.21 |
| AQ8 | 0.20 | −0.09 | 0.74 | −0.28 | 0.03 | −0.21 | −0.05 |
| AQ9 | 0.26 | 0.01 | 0.50 | −0.27 | 0.53 | −0.02 | 0.13 |
For the criterion analysis, the correlation between the observers, item-by-item correlation, and Cronbach's alpha coefficient were verified.
The socioeconomic level classification was measured using Brazil Criterion, based on the Brazilian Association of Market Research Institutes (Associação Brasileira de Empresas de Pesquisa [ABEP]), version.13
Statistical analysisQualitative variables were described as absolute or relative frequencies, and quantitative variables through means and standard deviations. For the validation process, the questionnaire factorial analysis was performed by calculating Spearman's correlation coefficient, considering acceptable values > 0.2, and by applying the KMO test and Bartlett's test. To perform the correlations between the observers and item-by-item correlations, Cronbach's alpha coefficients were evaluated, considering adequate values ≥ 0.6 and split-half correlations.
Data analysis and processing were performed using the SPSS program, version 17.0 (SPSS Inc. – Chicago, IL, United States). The level of significance was set at 5%. The sample size was considered as a minimum number of five participants for each item of the tool.
The study was approved by the Research Ethics Committee of Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), according to CAEE 1,087,639. The children's parents or guardians signed an informed consent.
ResultsIn total, 72 families participated in the study. The children's mean age was 9±6.7 months and of these, 35 (48.6%) were males. The families that participated in the study belonged to social classes A (9.68%), B (22.58%), C (33.87%), and D and E (33.87%) according to the ABEP criterion, and 50% of the families had less than nine years of schooling.
The acceptance of the IMF by the participants was 100%; i.e., no individuals abandoned the study after the tool began to be applied.
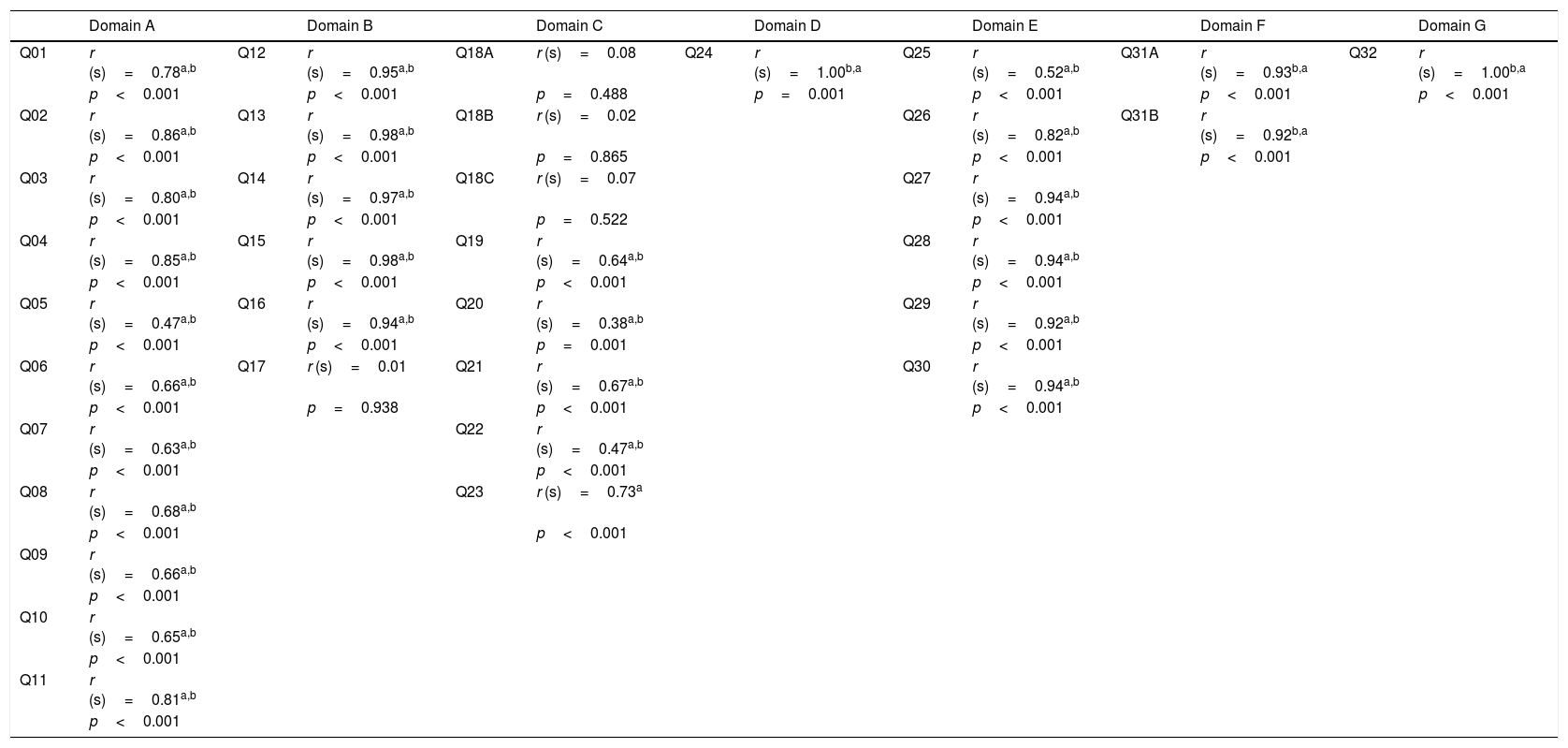
ValidityMost correlations between items and domains were significant. Questions about pets and electronic devices that were on during the interview were not significant with their domains (Table 2). The Cronbach's alpha of the questionnaire was 0.92 (95% CI: 0.89–0.95). Cronbach's alpha values greater than 0.8 were found in almost all domains, except in the C domain (Cα – 0.39 (95% CI: 0.16–0.58). Cronbach's alpha values in the domains A, B, D, E, F, and G were, respectively: A – Cα 0.96 (95% CI: 0.87–0.93); B – Cα 0.93 (95% CI: 0.91–0.95); D – Cα 0.92 (95% CI: 0.89–0.95); E – Cα 0.92 (95% CI: 0.89–0.95); F – Cα 0.83 (95% CI: 0.79–0.86), and in the G domain – Cα 0.92 (95% CI: 0.86–0.95). After excluding each one of the items, the Cronbach's alpha value was higher than 0.9. The intraclass correlation among the evaluators was 0.97 (95% CI: 0.96–0.98). When split-half correlations were analyzed, they showed r: 0.60, with p<0.001.
Psychometric properties of the Family Environment Assessment.
| Domain A | Domain B | Domain C | Domain D | Domain E | Domain F | Domain G | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q01 | r (s)=0.78a,b | Q12 | r (s)=0.95a,b | Q18A | r (s)=0.08 | Q24 | r (s)=1.00b,a | Q25 | r (s)=0.52a,b | Q31A | r (s)=0.93b,a | Q32 | r (s)=1.00b,a |
| p<0.001 | p<0.001 | p=0.488 | p=0.001 | p<0.001 | p<0.001 | p<0.001 | |||||||
| Q02 | r (s)=0.86a,b | Q13 | r (s)=0.98a,b | Q18B | r (s)=0.02 | Q26 | r (s)=0.82a,b | Q31B | r (s)=0.92b,a | ||||
| p<0.001 | p<0.001 | p=0.865 | p<0.001 | p<0.001 | |||||||||
| Q03 | r (s)=0.80a,b | Q14 | r (s)=0.97a,b | Q18C | r (s)=0.07 | Q27 | r (s)=0.94a,b | ||||||
| p<0.001 | p<0.001 | p=0.522 | p<0.001 | ||||||||||
| Q04 | r (s)=0.85a,b | Q15 | r (s)=0.98a,b | Q19 | r (s)=0.64a,b | Q28 | r (s)=0.94a,b | ||||||
| p<0.001 | p<0.001 | p<0.001 | p<0.001 | ||||||||||
| Q05 | r (s)=0.47a,b | Q16 | r (s)=0.94a,b | Q20 | r (s)=0.38a,b | Q29 | r (s)=0.92a,b | ||||||
| p<0.001 | p<0.001 | p=0.001 | p<0.001 | ||||||||||
| Q06 | r (s)=0.66a,b | Q17 | r (s)=0.01 | Q21 | r (s)=0.67a,b | Q30 | r (s)=0.94a,b | ||||||
| p<0.001 | p=0.938 | p<0.001 | p<0.001 | ||||||||||
| Q07 | r (s)=0.63a,b | Q22 | r (s)=0.47a,b | ||||||||||
| p<0.001 | p<0.001 | ||||||||||||
| Q08 | r (s)=0.68a,b | Q23 | r (s)=0.73a | ||||||||||
| p<0.001 | p<0.001 | ||||||||||||
| Q09 | r (s)=0.66a,b | ||||||||||||
| p<0.001 | |||||||||||||
| Q10 | r (s)=0.65a,b | ||||||||||||
| p<0.001 | |||||||||||||
| Q11 | r (s)=0.81a,b | ||||||||||||
| p<0.001 |
Correlation is significant at the 0.05 level (two extremities).
Domain A, Mother's communication ability. Domain B, Behavior. Domain C, Organization of the physical and temporal environment. Domain D, Collection/quantity of appropriate toys. Domain E, Maternal attitude of constant attention toward her baby. Domain F, Diversification of stimuli. Domain G, Baby's behavior. Q1, The mother vocalizes (produces sounds)/speaks spontaneously with her baby. Q2, The mother responds to the baby's vocalizations/words. Q3, The mother gives the baby/twin the name of any object during the visit or gives the name of a person or object in a pedagogical way. Q4, The mother's speech to the baby/twin is distinct, clear, audible (easily intelligible). Q5, During the interview the mother: speaks little; has an almost unintelligible language; speaks moderately and coherently; speaks almost constantly. Q6, The mother initiates verbal exchanges with the interviewer, asks questions, makes comments spontaneously. Q7, The mother expresses her ideas freely and easily has answers that constitute an appropriate extension to the conversation (i.e., gives brief answers). Q8, The mother spontaneously praises the qualities or behavior of her baby. Q9, When she talks about her baby or with her baby, the mother's voice expresses positive feelings. Q10, The mother caresses or hugs the baby during the visit. Q11, The mother expresses positive feelings when the interviewer compliments her baby. Q12, The mother yells at the baby. Q13, The mother seems clearly troubled by her baby and shows hostility toward him/her. Q14, The mother hits the baby and slaps him/her on the buttocks during the visit. Q15, The mother scolds and criticizes the baby. Q16, The mother intervenes in the baby's actions and restricts his/her movements. Q17, The family has a pet. Q18, During the visit, the following devices are on: television; radio; Q20 During the visit, disturbing noises of human voices, television, radio or other sources were heard. Q20, The degree of activity in the house during the interview may be classified as: slow; active but not turbulent; very active and turbulent, but not during the entire visit; very active and very turbulent during most of the visit. Q21, Does the layout of the windows and doors of the house allow the baby to have a view of the outside environment? Q22, The environment where the baby plays seems safe and not dangerous. Q23, Overall, the inside of the house was: quite in order and clean; in order and clean; a little cluttered, but clean; a little cluttered and dirty; quite cluttered, but clean; quite cluttered and dirty. Q24, The mother provides interesting toys or activities to the baby. Q25, The mother tends to keep the baby in her field of vision and watches him/her often. Q26, The mother talks to her baby while working or doing her chores. Q27, The mother consciously encourages the baby's progress in his/her development. Q28, The mother values educational toys for the attention she dedicates to them. Q29, The mother structures the baby's periods of playing to develop new skills. Q30, The mother offers the baby stimulating toys. Q31A, How many people were present at the house during the visit? Number. Q31B, How many of these people do not live regularly in the house? (excluding the interviewer). Q32, During the visit the baby was: irritable; awake and active; awake but passive; sleeping; absent.
In the factorial scale analysis, the KMO values (Table 1) were 0.76, Bartlett's test showed p<0.001, and the correlation between items and domains had p<0.01. In variable 17 of the IMF questionnaire, the communality test was p<0.46. When this variable was removed, the value increased to p>0.8. Variable 17 refers to the presence of pets in the household.
DiscussionThe results found in this study show the excellent performance of the IMF questionnaire regarding its validity for use in the Brazilian population.
When evaluating the psychometric properties of the tool, the Brazilian version of the IMF performed well regarding its validity, particularly in the domains of mother's communication; collection/quantity of toys; mother's fussy attitude toward her baby; stimulus diversification; and baby's behavior.
The results of this study showed a good correlation with most of the items and domains that show a direct association between the mother's communication and the child. The items for which an adequate association was not shown, such as TV, dog, and toys, are not directly related to the child's bond with the parents.
The importance of the family environment and parental relationships in child development has been widely described in the literature.9,10,14 Studies show the importance of environmental stimuli and family care in the child's development and cognitive performance.9,10,14–18 The present results corroborate findings from previous studies that used the HOME scale,9,10,14 by suggesting that caregivers who give the most attention to the bond maintained with the child (maternal attitude of constant attention with her baby), have better communication capacity and also provide a greater number of stimuli appropriate to their development.
The use of scales that evaluate the family environment in different social and cultural contexts has indicated the importance of the socioeconomic level and the cultural context as predictors of the quality of family environment. The higher the socioeconomic level and the level of schooling of the caregivers, the higher the quality of family environment.14,19,20
One of the limitations of this study was the inclusion of economically disadvantaged families. More than 60% of the study population showed an economic classification below the C1 level, according to the ABEP criteria, which corresponds to the lower middle class in Brazil. Even so, the results did not show any harm to the assessment of the main questionnaire domains.
Another limiting factor of the study was the application of the tool associated to the home visit, with direct observation of the caregiver by professionals. Some of these families live in an area marked by social vulnerability and are followed by the local community health team. It was observed that some caregivers felt intimidated by the evaluator's presence and attempted to demonstrate a greatly increased bond with the child. Many of these disadvantaged families rely on the local health team's evaluation to receive the social benefits, which could influence their attitude during the visit. To maintain the tool's reliability, families from higher social classes also participated.
The tool was applied even when the child remained asleep during home observation, since one of the responses of all items in the domains comprises the Absent/Sleeping Baby/Twin option. This fact could directly interfere with the observation of the bond established between the caregiver and the child and, similarly, with the progress of the family environment. However, the good performance of the questionnaire indicates that this was not a relevant limitation.
Although there are no other scales similar to the present scale so that comparisons could be made, there are studies that have analyzed the reliability of HOME, such as the one by Elardo et al. in 1975. The authors found an internal consistency ranging from moderate to strong (0.44–0.89)2 when analyzing the psychometric properties of the tool. The use of the HOME questionnaire in different populations (preterm, low-social class families, families with low levels of schooling) also showed adequate internal consistency.10,20–22
In 2000, Holditch-Davis and colleagues validated the HOME questionnaire in clinically-ill children and found an internal consistency coefficient of 0.84 at 6–12 months of age. The authors studied the intraclass correlation indexes between the different domains of the HOME tool and the general correlation index of the questionnaire, which ranged from 0.6 to 0.8.23
In addition to studies evaluating the psychometric properties of the HOME tool, several authors found a positive predictive value of the tool in determining the child's cognitive development, especially the verbal communication development. These studies show the importance of the HOME tool both for use in clinical practice and in future child development studies.19,21–29
The family is the first context of child socialization and development, and probably the one with the greatest significance in determining the more or less adaptive developmental trajectories of children. The systematized analysis of the family environment allows us to study the influence of the family and the parental system on children's development. The HOME inventory is the most frequently used family environment assessment measure worldwide. The IMF is a scale equivalent to the HOME questionnaire. There are four versions of HOME, and the original versions used in small children (0–2 years of age) were adapted in 2003.13
Although both the national and international literature show a growing interest in the influence of the family environment on child development, research in this area is still scarce. In Brazil, there are no validated scales for the Portuguese language that allow such research to be carried out.
The present study allowed the validation of the IMF tool in Brazil, taking care to assess families from different social classes. It is known that families differ substantially in the quality of the environment they provide to children and that differences are even higher in other social classes.14,15
The validation into the Portuguese language of the IMF the French version of the Infant/Toddler HOME, will enable the use of this tool in Brazilian children, allowing the assessment of the family environment and the quality of the stimuli offered to child development in new studies and clinical practice Brazil.
In conclusion, the IMF showed good performance regarding the assessed psychometric properties: validity.
FundingEdital Pesquisador Gaúcho 2013 – Fundo de Amparo à Pesquisa do Estado do Rio Grande do Sul.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Sudbrack S, Barbosa FP, Mattiello R, Booij L, Estorgato GR, Dutra MS, et al. Validation of the Inventaire du Milieu Familial Questionnaire (French version of the Infant/Toddler HOME) into the Brazilian Portuguese language. J Pediatr (Rio J). 2019;95:314–20.
Study carried out at Escola de Medicina, Programa de Pós-Graduação em Pediatria e Saúde da Criança Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Instituto do Cérebro (InsCer-BraIns), Porto Alegre, RS, Brazil.




