

Inhalation therapy is the main treatment for asthma and its adequate use has been a factor responsible for disease control; therefore, the aim of the study was to determine whether a digital media tool, which features portability on mobile phones, modifies the assimilation of the inhalation technique.
MethodsA total of 66 professionals working in the health care area with the pediatric population were selected. They were submitted to a pre-test on their knowledge of inhalation therapy. The professionals were randomized into two groups (A and B). Group A received a media application on their mobile phones showing the steps of inhalation therapy, while group B received the same information in written form only. A post-test was applied after 15 days. The results (pre- and post-) were analyzed by two pediatric pulmonologists.
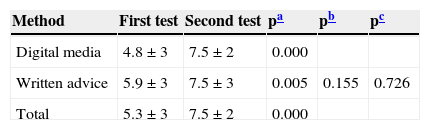
ResultsOf the 66 professionals, 87.9% were females. Of a total possible score of ten, the mean score obtained in the pre-test was 5.3±3, and in the second test, 7.5±2 (p<0.000). There were no significant differences when comparing the two groups (p=0.726). The nurses had the lowest mean scores in the initial test (2.3±2); however, they were the group that learned the most with the intervention, showing similar means to those of other groups in the second test (6.1±3).
ConclusionThere was significant improvement in knowledge about inhalation therapy in all professional categories using both methods, demonstrating that education, when available to professionals, positively modifies medical practice.
A Inaloterapia representa a principal forma de tratamento da asma e seu uso adequado tem sido fator responsável pelo controle da doença, desse modo o objetivo do estudo foi determinar se uma ferramenta de mídia digital, dotada de portabilidade na forma de telefonia móvel, modifica a assimilação da técnica inalatória.
MétodosForam selecionados 66 profissionais que atuam na área da saúde com população pediátrica. Estes foram submetidos a um pré-teste sobre seus conhecimentos de inaloterapia. Os profissionais foram randomizados em dois grupos (A e B). Grupo A recebeu em seu telefone móvel um aplicativo de mídia com os passos da inaloterapia, enquanto grupo B recebeu as mesmas informações apenas de forma escrita. Após 15 dias, realizou-se um pós-teste. Os resultados (pré e pós) foram analisados por dois pneumologistas pediátricos.
ResultadosDos 66 profissionais, 87,9% eram do sexo feminino. Num escore total possível de dez, a média das notas obtidas no pré-teste foi de 5,3±3 e as do segundo teste7,5±2 (p<000). Não houve diferenças significativas comparando os dois grupos (p=0,726). Os profissionais de enfermagem apresentaram a menor média nas provas iniciais (2,3±2), porém, foi o grupo que aprendeu mais com a intervenção, apresentando média similar aos outros grupos na segunda prova (6,1±3).
ConclusãoHouve melhora significativa no conhecimento sobre inaloterapia em todas as categorias profissionais usando ambos os métodos, comprovando que a educação quando disponibilizada aos profissionais, modifica positivamente a prática médica.
Asthma has an important role in pediatric clinical practice due to its prevalence. It currently affects roughly 300 million people worldwide.1
In Brazil, considering the overall prevalence of 10%, it is estimated that there are 20 million asthmatic individuals. A total of 160,000 hospitalizations were recorded in 2011, making asthma the fourth most frequent cause of hospitalization in the country.1
Several drugs and different routes of administration have been used for adequate disease control. The inhalation route is currently the most frequently used and studied for use both during crises and for maintenance drug therapy.2
Several factors may modify the pharmacokinetics of medication: age, breathing pattern, use of spacers, and aspects related to the correct use of the technique.3
The most commonly used inhalation devices in the pediatric population are pressurized metered-dose inhalers (MDI). These, when used in children, require the use of a spacer that minimizes the need to coordinate breathing and reduces the deposition of particles in the oral cavity, reducing side effects.
Applying the adequate technique using the MDI with spacer is not a consensus among health care professionals. Few know how to perform or properly teach the technique to their patients. According to literature data, technical adequacy rates can range from 15% to 69% among these professionals, considering different professional areas.4 Studies comparing success rates and assimilation technique have been more successful regarding strategies that include a process of continuing education and periodic revision.5
Although one study4 has demonstrated improved technique among health professionals who receive adequate information and those who review it frequently, there is no suggestion in the literature for a simple, effective, and low-cost way to provide this training.
Furthermore, the importance of performing the inhalation technique is still seldom discussed during medical training, lacking adequate emphasis in textbooks that are not specific to the area, and focusing such knowledge only on specialists.
Considering the idea of improving asthma control and treatment through health professional and patient education, the authors developed a mobile application for continuing education directed at the adequate use of inhalers in the pediatric population, thereby creating a teaching tool available to all professionals.
The aim of this study was to evaluate the knowledge of different health professionals on the use of inhalation therapy and determine whether the digital media tool, available for the Android (Google Inc, CA, USA) and/or iOS platform (Apple Inc, CA, USA) for use in mobile phones, modifies the assimilation of the presented content, thus more comprehensively disseminating knowledge on inhalation therapy.
MethodsAt the initial stage of research development, a video was created disclosing the correct technique for using the pressurized MDI+spacer. The video was divided into two segments, considering differences in the age stratum. The first segment explained and demonstrated, with the help of a 3-year-old child, the appropriate technique for using a mask. In the second, a 12-year-old child demonstrated the technique for patients older than 7 years. The actors were selected from the clinical office of one of the researchers (SLA), were familiar with the procedure, and were considered very adequate as technique performers. To standardize the procedure and create a measurable test tool, this study used the step-by-step pattern recommended by The Lung Association (Canadian Lung Association, ON, Canada).6
Based on the video, an application prototype was developed, compatible with all mobile phone platforms with Internet access, and easily used by participants (Fig. 1).

To test the application, professionals were selected who worked in a pediatric referral hospital (Hospitalda Criança Santo Antônio [HCSA], Porto Alegre, RS, Brazil).
Based on a proportion of adequate knowledge among health professionals of approximately 40% (mean of results in learning studies), considering a suggested proportion of knowledge of 70% (to be achieved post-intervention), for a level of significance of 5% and power of 80%, the minimum sample size of subjects to be allocated per group was estimated at 16, constituting a global population of 64 subjects (four research groups).
A clinical trial was designed aiming to compare the performance on the adequate use of inhalation therapy among four groups of hospital professional categories. The selection was randomized from the list of the members of these professional categories, obtained from the Human Resources Department. The groups were constituted as follows: medical pediatric residents (n=16), from a total of 21; pediatric nurses (n=16), from a total of 47; pediatric emergency physicians (n=16), from a total of 25; and pediatric ICU physicians (n=16), from a total of 28. A second randomization was performed within the groups to determine which participants would have access to the video and which would receive only written material. The knowledge of the professionals was compared within groups and between groups.
All participants were asked to write, in their own words, a sequential numerical description of the inhalation technique. The only information available was three images (pressurized inhaler, spacer, and patient), representing all parts involved in the inhalation technique process.
Based on a randomization process (1:1), half of each professional group had the application available on their mobile phones. During the process, they were instructed on how to use it. The other half received only the written guidelines.
Professionals selected from the randomization list that did not have a mobile phone with Internet access were excluded from the study, and were replaced by the next listed member. Two pediatric emergency physicians and six nurses were replaced because they did not have mobile phones compatible with the application.
Two weeks after the first test, the researchers visited the participants in their workplace once again and re-applied the test.
After the two steps were completed, both tests were corrected by two pediatric pulmonologists, who did not participate in the selection and teaching process. In a preliminary step, they developed a standardized correction tool that scored on a scale from 0 to 10. Four domains were considered the most important for the characterization of the evaluation process: 1) Order of steps associated with the correct procedure; 2) Most adequate choice of spacer availability technique according to age (oral inhalation through a mouthpiece versus inhaling through a face mask); 3) Process of shaking the medication canister; 4) Performance of adequate inspiratory technique. Each domain scored 2.5 points, and was considered only as achieved or not achieved, based on the written description of the technique by the participants. Notes from the pre- and post-test were then compared.
Means and standard deviations, distribution of frequencies, and percentages were used for quantitative data analysis. All analyses complied with the respective theoretical criteria for their performance.7 Bivariate analysis was used for continuous variables with non-normal distribution and for categorical ones (Mann-Whitney) to compare responses between tests. For categorical variables (McNemar test) and for continuous ones (Wilcoxon test) and for comparison between groups (Kruskal Wallis). Statistically significant associations were set at p<0.05. Data processing and analysis was performed using Stata software, release 11 (Stata Corp, College Station, TX, USA).
The study was submitted to and approved by the Research Ethics Committee of Universidade Federal de Ciências da Saúde de Porto Alegre (CAAE: 17165313.0.0000.5345). All participants signed an informed consent.
ResultsA total of 66 professionals who worked in the HCSA participated in the study. Of these, 58 (87.9%) were females and eight (12.1%) were males. All randomized participants completed the first step of the research. When applying the second intervention, six professionals were excluded from the study (a pediatric ICU physician, two pediatric nurses, two pediatric emergency physicians, and one pediatric resident).
The professionals who completed the tests demonstrated a significant development in the knowledge of inhalation technique. The mean score in the first test was 5.3±3 and the mean in the second test was 7.5±2 (p<0.000). There was no significant difference between the improvement in the scores between the group receiving the video compared to the group receiving written information, as shown in Table 1 (p=0.726).
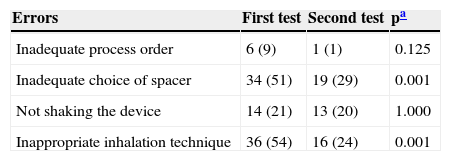
Test correction was concentrated in four areas considered important for inhalation technique. Errors in the first assessment occurred mostly regarding the adequate choice of the technique, 34 (51%), and the appropriate inspiratory technique, 36 (54%). These were also the items that showed greater progress in learning, with a decrease to 19 (29%) in errors associated with choice of technique (p=0.001) and to 16 (24%) in errors related to the adequate inspiratory technique (p=0.001; Table 2).
Assessment of errors between tests.
| Errors | First test | Second test | pa |
|---|---|---|---|
| Inadequate process order | 6 (9) | 1 (1) | 0.125 |
| Inadequate choice of spacer | 34 (51) | 19 (29) | 0.001 |
| Not shaking the device | 14 (21) | 13 (20) | 1.000 |
| Inappropriate inhalation technique | 36 (54) | 16 (24) | 0.001 |
Sample size=66 participants. Data presented as n (%).
There was no statistical difference between the types of errors made by participants in the two groups.
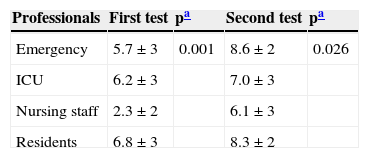
When analyzing the results considering the different professional groups, it was verified that the group of nurses had the lowest mean at the initial assessment (2.3±2), but was also the group with the highest evolution after the intervention, with a mean similar to that of the other groups in the post-test (Table 3).
DiscussionSuccessful asthma treatment can be attributed 10% to medication and 90% to education. Regardless of the medication composition, if it does not achieve an adequate dose in the lower airways, it will not provide effective treatment. Based on this rationale, the education of patients and health professionals on the proper use of inhalers is one of the mainstays for the treatment of asthma in the pediatric population.8–11
In spite of the relevance that this subject may deserve, little information is provided on the importance of the correct inhalation therapy in technical books.10 Currently, such information has been regarded as valuable appreciated in international consensuses, specialty societies, and formal guidelines established by disease control initiatives.
However, it is not clear how to proceed in order to adequately teach patients, considering the variability (31-85%) of health professionals who can adequately perform the inhalation technique.12,13 This was the main challenge that motivated the development of the present study. This proposal to create a practical teaching tool with easy access to health professionals is unprecedented, and is aligned with current trends of behavior.
The data indicate favorable responses in all professional categories, regardless of the educational tool used. This study was unable to identify differences in learning between the two educational techniques. However, it is noteworthy that the time interval between the applications of the two assessment methods (15 days) may have contributed to a lack of difference in results. Memory biases are often found in longer periods of intervention between the tests, which could result in a greater difference between the tools.
The frequency of access to the two training modalities could influence the learning curves and the attained results. However, this variable was not measured, making it impossible to determine whether the result could have been influenced by a higher frequency of access.
In the authors’ view, more important than the frequency of access is the result obtained from the provided information. The frequency of access may be intrinsically associated with the method.
At a time of undeveloped digital media (1982), patients disclosed that they did not consider written information to be very useful in terms of recommendations and that they often disposed of it out without reading it.14 Moreover, a study regarding the considerations of healthcare professionals and patients on the use of mobile technology for asthma control showed that 43% of the professionals and 52% of the patients credited to this technology the capacity to contribute to a better control of the disease;15 however, it was not possible to confirm such behavior.
The literature demonstrates the preference of professionals and patients for the use of digital media.16–18 A study focused on the comparison of teaching through video or written texts showed a better understanding of the procedures in teaching techniques with video. Furthermore, the study showed that images improve long-term memory of the obtained knowledge.19
Inhalation therapy is a matter of relevance within the pediatric practice; however, a consensus on the best technique to consolidate this knowledge has not been established. The use of a video reduces the time spent by the professional teaching this practice, making it more feasible in everyday life. The use of digital media also becomes important in light of the need for a more interactive education that meets the needs of a new generation of professionals who use technology as a work tool.17 Studies on education have found that students do not want to read long texts, and are stimulated by rapid learning and media tools where information is made available in a more dynamic manner.16
Some characteristics inherent to the developed technology have interesting features regarding any educational process: rapid access, constant availability, and its adaptation to a communication tool routinely used by the professionals. Of the 66 randomized participants, only eight did not have a smartphone and, thus, were replaced by the next randomized participant. This indicates that most of the selected health professionals (87.5%) can access the application without difficulty.
Studies have shown that regular repetition is an important factor for maintaining knowledge associated with the use of inhaling devices.4,17 At eight months after the educational intervention, only 59% of physicians still performed the inhalation technique adequately, reinforcing the need for constant re-training.12 Considering this finding, the intrinsic characteristics of digital media (availability and portability) may contribute to this ongoing process of learning.
The group of nurses had the lowest initial mean, which is noteworthy as they represent the professional class that is assigned to perform the inhalation technique together with the patient. However, it was also the group that showed the greatest improvement between the two tests, equaling the performance of other groups in the final assessment. This demonstrates that more frequent application of educational processes could influence memorization and learning of the technique.
Asthma, as all other chronic diseases, represents an important economic burden for patients, as well as for the health system.9 Expenses related to the incorrect use of medications for asthma vary between seven and 15 billion dollars/year in the USA. The estimated cost for the education of patients with chronic diseases is US$ 30 per patient.
If it is considered that there are 30 million inhaler users, there will be a cost of 900 million dollars in education alone.10 The training of health professionals through the application, considering that it is easy to use and free of charge, could reduce these costs and allow the use of public resources in other areas, such as medication supply.
The lack of difference between the two interventions should not be seen as a discouragement to the implementation of any one of the tools, considering the overall improvement attained. This finding further supports the importance of creating strategies in continuing education for inhaling technique training, especially among professionals who practice it daily.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the professionals who participated in the study, as well as the expertise of marketing professional Bernardo Fleck Manganelli, for the support and development of the digital media.
Please cite this article as: Velasco HF, Cabral CZ, Pinheiro PP, Azambuja RC, Vitola LS, Costa MR, et al. Use of digital media for the education of health professionals in the treatment of childhood asthma. J Pediatr (Rio J). 2015;91:183–8.




