


To investigate trends in breastfeeding indicators in the city of Feira de Santana, Brazil, and to identify population characteristics that might have influenced this trend.
MethodsThree methodologically comparable cross-sectional surveys performed in 1996, 2001, and 2009 were analyzed. These involved 2,159, 2,319, and 1,471 children younger than 1 year of age who were vaccinated in national multivaccination campaigns in the respective years. A standardized questionnaire was used, containing closed questions on consumption of breast milk and other foods on the day before the survey, along with questions regarding the characteristics of the population.
ResultsThe annual growth of the breastfeeding indicators was 2.1% for breastfeeding in the first hour of life (from 52.2% to 68.9%); 1.1% for breastfeeding among children aged 9 to 12 months (from 45% to 59.6%); and 0.8% for exclusive breastfeeding among infants younger than 6 months (from 36.9% to 47.4%). The median duration of exclusive breastfeeding increased from 52.3 to 84.3 days, and overall breastfeeding from 278 to 376 days. Some changes in the characteristics of the population were observed, which may have positively influenced the evolution of the breastfeeding indicators (better schooling level among the mothers, less use of dummies/pacifiers, and lower proportions of adolescent mothers), or negatively (greater proportions of primiparous mothers and cesarean deliveries, and lower frequency of births in Baby-Friendly Hospitals).
ConclusionThere were significant advances in breastfeeding indicators, although they are still far from ideal. Changes observed in population characteristics may have positively or negatively influenced this evolution.
Verificar a tendência dos indicadores de aleitamento materno (AM) em Feira de Santana, Brasil, e identificar características da população que possam ter influenciado essa tendência.
MétodosProcedeu-se a análise de três inquéritos transversais, metodologicamente comparáveis, realizados em 1996, 2001 e 2009, envolvendo 2.159, 2.319 e 1.471 menores de um ano vacinados na campanha nacional de multivacinação desses anos. Utilizou-se questionário contendo questões sobre o consumo de leite materno e outros alimentos no dia anterior ao inquérito, além de perguntas sobre características da população.
ResultadosO acréscimo anual nos indicadores de AM foi de 2,1 pontos percentuais para o AM na primeira hora de vida (de 52,2% para 68,9%); 1,1 pontos para o AM em crianças de 9 a 12 meses (de 45% para 59,6%); e de 0,8 pontos para o AM exclusivo (AME) em menores de seis meses (de 36,9% para 47,4%). A duração mediana do AME aumentou de 52 para 84 dias, e a de AM de 278 para 376 dias. Observou-se mudanças nas características da população, as quais podem ter influenciado a evolução dos indicadores do AM de forma positiva (melhor escolaridade das mães, decréscimo no uso de chupeta e menor prevalência de mães adolescentes), ou negativa (maior proporção de mães primíparas e de cesarianas, e menor frequência de nascimentos em Hospital Amigo da Criança).
ConclusãoHouve avanços significativos nos indicadores de AM em Feira de Santana, embora ainda estejam longe do ideal. Mudanças observadas nas características da população podem ter influenciado positiva ou negativamente essa evolução.
Considering the impact of breastfeeding (BF) on child health, with significant impact on infant mortality rates,1 the promotion, protection and support of BF have been increasingly prioritized in public health policies.
In Brazil, several measures have been implemented in the last 30 years, including the Baby-Friendly Hospital Initiative (Iniciativa Hospital Amigo da Criança–IHAC), Kangaroo Care; the creation of the Brazilian Network of Human Milk Banks (Rede Brasileira de Bancos de Leite Humano–BLH); the national commemoration of the World BF Week; the Brazilian Breastfeeding and Feeding Strategy, focused on the encouragement of breastfeeding in primary care; and recently, encouraging the installation of breastfeeding support rooms in the workplaces of nursing women, among others.2
As a result of these measures, significant advances have been observed in BF indicators in the country. Exclusive breastfeeding (EBF), which was virtually non-existent in the 1980s, was practiced by 38.6% of mothers of children younger than 6 months in 2006, and the BF median increased from 2.5 months in 1974 to 11.9 months in 2006.3 The two BF Prevalence Surveys (Pesquisas de Prevalência de Aleitamento Materno–PPAM) in Brazilian state capitals and the Federal District, held in 1999 and 2008,2,4 showed great variability in BF indicators between the capitals. In the 2008 survey, the median duration of EBF ranged from 0.7 days, in a capital of the Midwest, to 89 days in a Northern capital. The duration of BF ranged from 293 days in São Paulo, to 601 days in Macapá, in North Brazil.2,4 The comparison of the results of the PPAM in 1999 and 2008 also demonstrated large variations in the indicators’ evolution in different capitals. For instance, in Fortaleza there was a decrease in the prevalence of EBF in children younger than 4 months from 57% to 41% and in Campo Grande there was an increase in the prevalence of this indicator from 28% to 62%.4
Given the fact that BF indicators and their evolution vary significantly between Brazilian municipalities, it is important for each locality to know and monitor its indicators, assessing trends and factors associated with them. Demographic characteristics are associated with the practice of breastfeeding, such as age, education, parity, maternal employment, place of birth, type of delivery, and pacifier use, among others. The determinants of BF vary in magnitude and effect between different populations.5,6
Feira de Santana, in the countryside of the state of Bahia, has been highlighted due to its BF indicators and its work supporting BF. Noteworthy institutions include the city's implementation of the first human milk bank (HMB) in the state and the Breastfeeding Incentive Center (Centro de Incentivo em Aleitamento Materno–CIAMA), references in the state of Bahia, in addition to two IHAC-accredited hospitals, measures that allowed the implementation of actions to promote breastfeeding.7 In Bahia, there are only six HMBs and eight IHAC-accredited hospitals.
In view of the municipality's commitment to improve their BF indicators and the existence of three BF prevalence surveys with a representative sample, this study aimed to evaluate the trend of BF indicators in that city. In addition, this study sought to identify possible changes in population characteristics that may have influenced this trend.
MethodologyData from three BF prevalence surveys were used, whose methodological characteristics were similar, with cross-sectional design, performed in 1996, 2001, and 2009 in Feira de Santana, a large city with a population of 606,139 inhabitants in 2013.8
A probabilistic sample of children younger than 1 year was obtained in each of the studies; these children attended the second phase of the national multivaccination day in the respective years, through cluster samples, by drawing of the vaccination units and proportional probability to the size of the clusters. All children younger than 1 year of age, living in Feira de Santana, which attended the units that were drawn, were included in the studies. The sample estimates calculated for 1996, 2001, and 2009 were, respectively, 1,663, 1,587 and 1,420 children. A total of 2,159 children in 1996, 2,319 in 2001, and 1,471 in 2009 participated in the surveys.
While waiting for the vaccination, adult caregivers, after signing the informed consent, were interviewed by previously trained university students from the health area (40 in 1996, 104 in 2001, and 166 in 2009).
All the surveys used a standardized questionnaire with closed questions on the consumption of breast milk and other foods, including water, teas, and other types of milk, on the day before the survey. This type of survey (current status) is recommended by the World Health Organization (WHO)9 to assess BF indicators at the population level. In the 1996 survey, the data collection tool was created by the authors in accordance with WHO recommendations. In 2001 and 2009, the tool was based on the form prepared by the Ministry of Health, for the first and second PPAM, respectively.4 The data collected in 2009 were entered into a web application developed for the PPAM of the Ministry of Health in the year 2008,4 and the data were exported to SPSS (Inc. Released 2008. SPSS Statistics for Windows, Version 17.0. Chicago, USA), the same software used in the previous surveys.
In addition to the nutrition survey, in 2001 and 2009 the following information were obtained regarding the children: birth weight, gender, birth in a Baby Friendly Hospital (Hospital Amigo da Criança–HAC), and pacifier use; and maternal age, education, work outside the home, parity, and mode of delivery. The 1996 survey did not provide such data.
The data allowed for evaluation of the following BF indicators: BF in the first hour of life; prevalence of EBF in children younger than 6 months; prevalence of breastfeeding in children between 9 and 12 months, and median duration of BF and EBF. The BF indicator in the first hour of life was not studied in the 1996 survey. BF and EBF definitions adopted by the surveys are the same as those recommended by WHO.10 EBF was considered as children who received only breast milk; and BF as infants who were breastfed, regardless of receiving other foods.
The proportion of children younger than 1 year of age who were breastfed in the first hour of life, of children younger than 6 months who were EBF, and of children between 9 and 12 months who were BF was estimated. Then, the differences were measured regarding the prevalence of the indicators for the periods 1996-2001, 2001-2009, and 1996-2009, and the annual change in percentage was calculated. Pearson's chi-squared test was used to compare differences in prevalence between the three surveys, using a significance level of 5%. The estimated median duration of BF and EBF was calculated by logit analysis, which estimates, by statistical modeling, the odds of the event as a function of age.
The characteristics of children and mothers of the 2001 and 2009 surveys were compared using Pearson's chi-squared test and a significance level<5%.
Each of the studies observed the legislation regarding human subjects (National Health Council Resolution 196/96),11 in accordance with the Declaration of Helsinki. Studies performed in 1996, 2001, and 2009 were approved, respectively, by the Ethics Committee of Hospital Geral Clériston Andrade (HGCA), by the Ethics and Research Committee of Universidade Federal da Bahia, and by the Ethics and Research Committee of Universidade Estadual de Feira de Santana (UEFS).
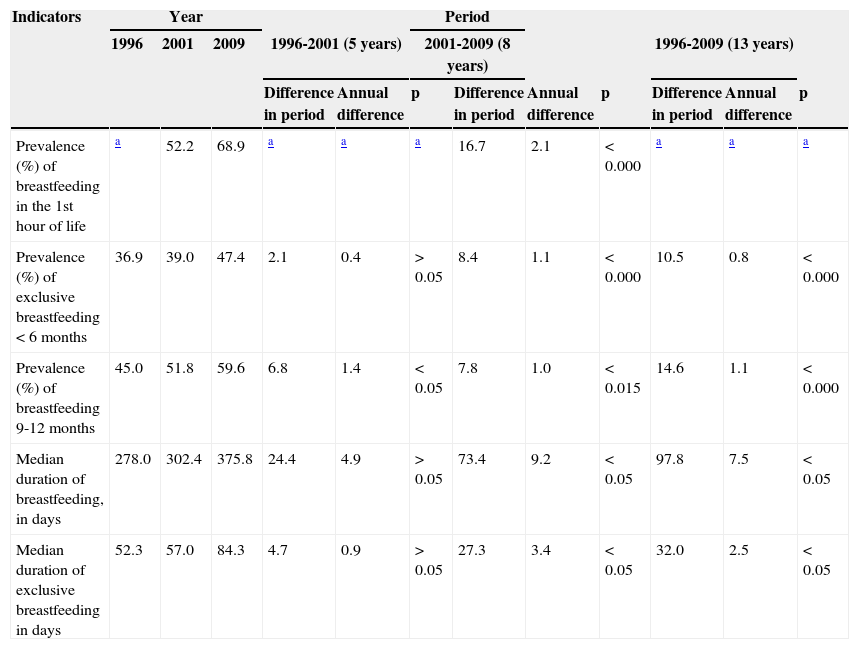
ResultsTable 1 shows the BF indicators in each survey and their trends over the 13 years between the first and third surveys. Significant improvements in all indicators were observed. BF in the first hour of life showed an annual increase of 2.1% (considering the eight years between the second and third surveys). For BF in children from 9 to 12 months, the annual increase was 1.1%, and the EBF in children younger than 6 months was 0.8%, considering the interval of 13 years. EBF prevalence rates in children younger than 6 months and BF in children younger than 1 year, in monthly age intervals, from the surveys applied in 1996, 2001 and 2009 in Feira de Santana, are shown, respectively, in Figs. 1 and 2.
Breastfeeding indicators. Feira de Santana, Brazil, 1996, 2001, and 2009.
| Indicators | Year | Period | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1996 | 2001 | 2009 | 1996-2001 (5 years) | 2001-2009 (8 years) | 1996-2009 (13 years) | |||||||
| Difference in period | Annual difference | p | Difference in period | Annual difference | p | Difference in period | Annual difference | p | ||||
| Prevalence (%) of breastfeeding in the 1st hour of life | a | 52.2 | 68.9 | a | a | a | 16.7 | 2.1 | < 0.000 | a | a | a |
| Prevalence (%) of exclusive breastfeeding<6 months | 36.9 | 39.0 | 47.4 | 2.1 | 0.4 | > 0.05 | 8.4 | 1.1 | < 0.000 | 10.5 | 0.8 | < 0.000 |
| Prevalence (%) of breastfeeding 9-12 months | 45.0 | 51.8 | 59.6 | 6.8 | 1.4 | < 0.05 | 7.8 | 1.0 | < 0.015 | 14.6 | 1.1 | < 0.000 |
| Median duration of breastfeeding, in days | 278.0 | 302.4 | 375.8 | 24.4 | 4.9 | > 0.05 | 73.4 | 9.2 | < 0.05 | 97.8 | 7.5 | < 0.05 |
| Median duration of exclusive breastfeeding in days | 52.3 | 57.0 | 84.3 | 4.7 | 0.9 | > 0.05 | 27.3 | 3.4 | < 0.05 | 32.0 | 2.5 | < 0.05 |


The median duration of EBF increased from 52.3 days (95% CI: 44.8 to 60.7) in 1996 to 84.3 days (95% CI: 73.7 to 94.9) in 2009, whereas BF increased from 278 days (95% CI 264.1 to 292.3) to 375.7 days (95% CI: 342.5 to 409.0) in the same years, both statistically significant (Table 1).
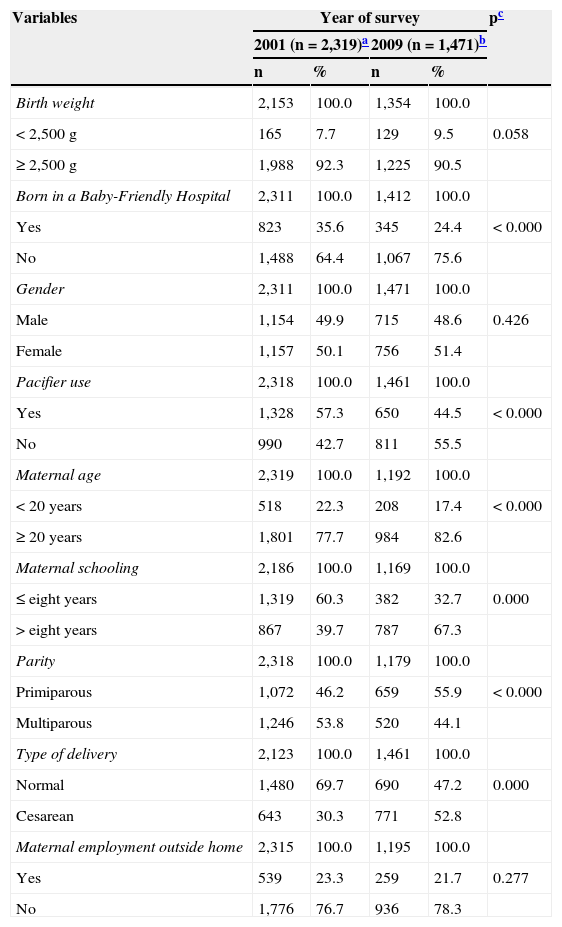
Table 2 compares maternal and children's characteristics in 2001 and 2009. In 2009 there was a higher proportion of mothers aged 20 or older (+ 4.9%) and higher education (+ 27.6%), primiparous (+ 9.7%) and cesarean deliveries (+ 22.5%); and lower frequency of births in HAC (- 11.2%) and pacifier use (- 12.8%).
Description and comparison of maternal characteristics and of children younger than 1 year. Feira de Santana, Brazil, 2001 and 2009.
| Variables | Year of survey | pc | |||
|---|---|---|---|---|---|
| 2001 (n=2,319)a | 2009 (n=1,471)b | ||||
| n | % | n | % | ||
| Birth weight | 2,153 | 100.0 | 1,354 | 100.0 | |
| < 2,500g | 165 | 7.7 | 129 | 9.5 | 0.058 |
| ≥ 2,500g | 1,988 | 92.3 | 1,225 | 90.5 | |
| Born in a Baby-Friendly Hospital | 2,311 | 100.0 | 1,412 | 100.0 | |
| Yes | 823 | 35.6 | 345 | 24.4 | < 0.000 |
| No | 1,488 | 64.4 | 1,067 | 75.6 | |
| Gender | 2,311 | 100.0 | 1,471 | 100.0 | |
| Male | 1,154 | 49.9 | 715 | 48.6 | 0.426 |
| Female | 1,157 | 50.1 | 756 | 51.4 | |
| Pacifier use | 2,318 | 100.0 | 1,461 | 100.0 | |
| Yes | 1,328 | 57.3 | 650 | 44.5 | < 0.000 |
| No | 990 | 42.7 | 811 | 55.5 | |
| Maternal age | 2,319 | 100.0 | 1,192 | 100.0 | |
| < 20 years | 518 | 22.3 | 208 | 17.4 | < 0.000 |
| ≥ 20 years | 1,801 | 77.7 | 984 | 82.6 | |
| Maternal schooling | 2,186 | 100.0 | 1,169 | 100.0 | |
| ≤ eight years | 1,319 | 60.3 | 382 | 32.7 | 0.000 |
| > eight years | 867 | 39.7 | 787 | 67.3 | |
| Parity | 2,318 | 100.0 | 1,179 | 100.0 | |
| Primiparous | 1,072 | 46.2 | 659 | 55.9 | < 0.000 |
| Multiparous | 1,246 | 53.8 | 520 | 44.1 | |
| Type of delivery | 2,123 | 100.0 | 1,461 | 100.0 | |
| Normal | 1,480 | 69.7 | 690 | 47.2 | 0.000 |
| Cesarean | 643 | 30.3 | 771 | 52.8 | |
| Maternal employment outside home | 2,315 | 100.0 | 1,195 | 100.0 | |
| Yes | 539 | 23.3 | 259 | 21.7 | 0.277 |
| No | 1,776 | 76.7 | 936 | 78.3 | |
The trends of BF in the city during the 13 years showed significant improvement in the median duration of EBF and BF, and EBF prevalence in children younger than 6 months and BF in children from 9 to 12 months, in addition to the increased prevalence of BF in the first hour of life over eight years.
Comparing the 2009 survey results with the II PPAM in 2008,4 it can be observed that the BF indicator in the first hour of life in Feira de Santana (68.9%) was similar to that found for the group of Brazilian capitals (67.7%) and the Northeast region (66.9%), but higher than that found in Salvador (58.5%), the capital of Bahia. According to parameters adopted by WHO,12 this indicator in Feira de Santana can be classified as good.
A high level of homogeneity can be observed when comparing the BF indicator in children aged 9-12 months (59.6%) with that of Salvador (59.1%), that of the Northeast (59.1%), and all of the state capitals (58.7%).4 This indicator was used in this study as an indicator of BF continuity, as it was not possible to calculate, as suggested by the WHO, the proportion of children between 12 and 15.9 months, considering the investigation included only children younger than 1 year. The situation of Feira de Santana regarding the duration of breastfeeding is considered poor (376 days) according to the WHO criteria,12 although it is better than that of all the state capitals (342 days).
Feira de Santana shows an advantage on the EBF indicator in children younger than 6 months (47.4%) when compared with Salvador (36.5%), the Northeast (37.0%), and all of the Brazilian capitals (41%).4 Nevertheless, this situation is only considered reasonable by the WHO (between 12% and 49%).12 The median duration of EBF in Feira de Santana (84 days) exceeds by 50 days that of the Northeast (34 days), and by a month that of the Brazilian capitals (54 days). This information is relevant, as it is known that EBF protects against diseases and infant deaths.1
As for the evolution of BF indicators in Feira de Santana, there was considerable progress in all, particularly in the proportion of children breastfed in the first hour of life (increase of 16.7% in eight years), an average increase of approximately 2% per year. This annual increase is two-fold higher than that found for Brazil. The national demographic research in health in 199613 and 200614 showed an increase of 10.2% (from 32.8% to 43.0%) in 10 years, or roughly 1% per year. However, according to the same research, the increase observed in this study was lower than that observed for the Northeast (4.4% per year), increasing from 7.3% in 1996 to 51.4% in 2006. A recent meta-analysis found that the BF in the first hour of life is associated with a reduction of 44% to 45% of neonatal deaths from all causes and from infection.15 It is possible that the increase in this indicator in Feira de Santana is one of the factors that has contributed to this municipality demonstrating the highest decrease in neonatal mortality rate in the state of Bahia, from 27.8/1,000 live births in 2006 to 11.3/1,000 in 2012.16
The evolution of the BF continuity indicator, BF in children aged 9-12 months (increase of 14.6% in 13 years), was slightly lower than the evolution of this indicator in all the state capitals - 1.1% per year in Feira de Santana versus 1.8% per year in the capitals. This can be explained by the fact that the city is in a better position regarding this indicator in previous researches; the prevalence of BF in children aged 9-12 months in Feira de Santana in 1996 was higher than that in all the capitals in 19992 (45% versus 42.4%). Comparison of the results of the two PPAMs in the Brazilian capitals, conducted in 1999 and 2008, clearly showed that there was a greater increase in BF indicators in the capitals with worse conditions in 1999 and, on the other hand, more discreet advances or even regression in places where conditions were more favorable.2
Although Feira de Santana shows a privileged position regarding the EBF indicator in children younger than 6 months, this was the indicator that showed least development (increase of 10.5% in 13 years), with an increase of 0.8% per year. The fact that Feira de Santana had, in 1996, a prevalence of EBF in children younger than 6 months that was higher than the average found in the Brazilian capitals in 1999 (36.9% versus 26.7%),3 may explain, at least in part, this result.
To understand the temporal changes of BF indicators, it is necessary to consider the factors that may have influenced these changes in the city, because health indicator trends should be interpreted according to individual, social, and cultural determinants and public health policies. The development in BF indicators in Brazil has been supported by the National Policy for the Protection, Support, and Promotion of Breastfeeding.2,17
The implementation of various strategies of this policy in Feira de Santana may have contributed to the improvement of the BF indicators. The implementation of CIAMA/BLH (Reference Centre for the Promotion of Breastfeeding/Human Milk Bank), 1987, the creation of the second BLH, 1992, and the accreditation of two hospitals in IHAC in the mid-1990s started the increasing care for nursing mothers and training of human resources. In CIAMA/BLH, a total of 9,141, 27,118, and 80,691 women were treated, respectively, in the periods of 1987-1995, 1996-2000, and 2001-2008. During the same periods, a total of 143, 1,079, and 161 middle-level health care workers and 184, 146, and 225 upper-level health care workers were trained in breastfeeding management, in addition to mobilization during World BF Weeks.
The partnership between the BLHs, Universities, and the Municipal Health Secretariat allowed twelve BF events to be held for college students and health professionals and five “BF Meetings”, aimed at children and adolescents in the municipal schools. There is no assessment of the impact of these actions alone, but it is believed that all these actions contributed to the improvement of BF indicators in Feira de Santana. A study involving 111 municipalities of São Paulo found a 2.4-higher chance of EBF in children younger than 6 months when the municipality had four or more pro-BF actions.18
In addition to public investments for the protection, support, and promotion of breastfeeding in Feira de Santana, it is possible that changes of some population characteristics have influenced the BF indicators. Comparing maternal and children's variables in the last two surveys, it was observed that some changes may be favoring or hindering the development of BF indicators. Among the maternal factors that may be contributing positively are the lower proportion of adolescent mothers and higher educational level. Although there is no consensus on the association between younger maternal age and lower rates of BF, studies have shown this association in Brazil.4,19 Similarly, most studies have reported a positive association between higher maternal educational level and duration of BF, especially EBF, with a dose-response effect.4,6,18,20
Regarding the children's characteristics, the decrease in the prevalence of pacifier use is probably associated with the positive evolution of BF indicators in Feira de Santana. The association between pacifier use and BF duration has been demonstrated in virtually all studies.6,21 However, it is important to emphasize that the involved mechanisms remain unclear. A recent meta-analysis suggests that pacifier use by children of women that were highly motivated to breastfeed was not associated with shorter duration of BF, regardless of the age at which the pacifier use was started.22
Although some changes in population characteristics may have promoted the positive development of BF indicators in the city, others may have inhibited further advancement, such as the increase in the proportion of primiparous mothers and cesarean deliveries. Although primiparous women wish to initiate breastfeeding, they usually practice it for less time.23,24 Regarding the type of delivery, studies have found a lower prevalence of BF24,25 and EBF6,23,25 in women undergoing surgical deliveries. Feira de Santana follows the national trend of increasing prevalence of cesarean delivery in Brazil.26
In addition to the already mentioned individual factors, the decrease of births in HAC may have negatively influenced the evolution of BF indicators, as the positive influence of IHAC on the prevalence of BF has been well documented.27,28
The main methodological limitations of this study are due to its design, which does not establish a perfect causal association between the change in population characteristics and the evolution of BF, as it was a cross-sectional survey. Additionally, some sociodemographic characteristics were not studied, such as family income, prenatal information, and paternal variables, among others;6 and the absence of information on the BF indicator in the first hour of life and population characteristics in the 1996 survey. However, the methodological approach is feasible and replicable,29 allowing monitoring of BF indicators over time, which is important for the planning of actions at the local level.
In conclusion, this study found a growing trend of the main BF indicators in Feira de Santana and additional knowledge related to changing population characteristics that may have positively or negatively influenced the observed trends. However, as observed in other parts of the country, these indicators are still far from being acceptable for the WHO, indicating the need to increase the practice of breastfeeding in the country.
FundingFundação de Amparo à Pesquisa do Estado da Bahia (FAPESB). Grant Term 73/04.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Vieira GO, Reis MR, Vieira TO, Oliveira NF, Silva LR, Giugliani ER. Trends in breastfeeding indicators in a city of northeastern Brazil. J Pediatr (Rio J). 2015;91:270–7.




