



To verify the short-term influence of the kangaroo position (KP) on the electromyography activity of preterm newborns.
MethodA clinical study was conducted in a kangaroo unit sector (secondary and tertiary care) in the city of Recife, Brazil, with 44 preterm infants randomized to intervention (n=21) and control (n=23) groups. The KP was performed through a band that supports the newborn against the adult's thorax, in a prone and vertical position, and infants were dressed with few pieces of clothes, thus keeping skin-to-skin contact with the mother. Surface electromyography was used to investigate the muscle activity of the biceps brachii and hamstrings. The randomization of the groups was performed by the program R® (v. 3.3.1). The electromyography registrations were made at three different times: before the KP and after one and two hours of KP. In the control group, the registrations were performed at the times corresponding to those of the intervention group. The mean values of the electromyography activity among the times were analyzed by ANOVA for repeated measures and the Kruskal–Wallis test. The clinical trial was recorded in ClinicalTrials.gov (NCT02849665 - 07/28/2016).
ResultsIn the intervention group (n=21), there was a variation of the electromyography activity values between the three recording moments for both the biceps brachii and hamstrings. In the control group (n=23), there was no statistical difference between the recording moments for both.
ConclusionsThe KP increases the short-term electromyographic activity of the biceps brachii and hamstrings.
Verificar a influência de curto prazo da Posição Canguru (PC) sobre a atividade eletromiográfica de recém-nascidos prematuros.
MétodoFoi feito um estudo clínico em um setor da Unidade do Método Mãe Canguru (cuidado secundário e terciário) na cidade de Recife, com 44 neonatos prematuros randomizados em grupos de Intervenção (n=21) e Controle (n=23). A Posição Canguru foi feita por meio de uma faixa que apoia o recém-nascido de bruços contra o tórax do adulto, na posição vertical e vestido com poucas peças de roupa, mantém o contato pele a pele com a mãe. Foi usada a Eletromiografia Superficial para investigar a atividade muscular dos bíceps braquiais e músculos isquitobiais. A randomização dos grupos feita com o software R (versão 3.3.1)®. Os registros da eletromiografia foram feitos em três momentos: antes da PC e após uma e duas horas da Posição Canguru. No Grupo de Controle, os registros foram feitos nos momentos correspondentes àqueles do Grupo do Método Mãe Canguru. Os valores médios da atividade eletromiográfica entre esses momentos foram analisados pela análise de variância (Anova) de medidas repetidas e por um teste de Kruskal-Wallis. O ensaio clínico foi registrado no Clinical Trials (NCT02849665 – 28/07/2016).
ResultadosNo Grupo do Método Mãe Canguru (n=21), houve variação dos valores da atividade eletromiográfica entre os três momentos de registro de atividade dos bíceps braquiais e dos músculos isquitobiais. No Grupo de Controle (n=23), não houve diferença estatística entre os momentos de registro.
ConclusõesA PC aumenta a atividade eletromiográfica de curto prazo dos músculos bíceps braquiais e isquitobiais.
Kangaroo mother care (KMC) is a humanized and safe method of neonatal intervention, with established effectiveness in both the short- and mid-term.1,2 The main component of KMC is the kangaroo position, in which the infant is placed vertically in prone decubitus, between the mother’s breasts, with few clothes, and in contact with her skin.1–3
Due to its characteristics, the kangaroo position favors sensory stimulation of the tactile, proprioceptive, and vestibular systems4,5 of the newborn; these stimuli can facilitate tonic and postural adjustments, which may be relevant to motor development.
Studies show a positive effect of KMC on children's neurobehavioral and motor development.6–8 These studies have considered the influence of all components of the method (kangaroo position, exclusive breastfeeding, and early hospital discharge) and also have investigated general features of development.
However, few studies9,10 have specifically investigated the influence of the kangaroo position on the motor activities of newborns, particularly on physiological muscular responses. These studies have shown that preterm newborn placed in kangaroo position disclosed a continuous increase of electromyography activity in the period from 24h to 96h,9 a response that was not observed in newborns that were not placed on the position.10 These studies provided relevant information by observing an important modification in the muscular physiology of the newborns. Moreover, they used a more accurate tool to assess muscle tone, by measuring the electromyography activity of the muscle at rest.9,10 Nevertheless, some questions arise concerning this issue, such as the mechanisms by which the kangaroo position is capable of inducing this response, as well as how much time in the kangaroo position would be sufficient to induce changes in the electromyography behavior of preterm newborns. For the time being, no scientific investigations are studying this issue.
Therefore, the objective of this study was to verify the short-term influence of the kangaroo position on the electromyography activity of preterm newborns.
MethodsParticipantsA randomized clinical trial was conducted in the city of Recife, Brazil, from January to July 2017, with preterm newborns that were randomized into two groups: a kangaroo group (n=21) and a control group (n=23).
Instituto de Medicina Integral Professor Fernando Figueira (IMIP)’s Kangaroo Unit covers a surface area of 600m2 and has a ward with 22 beds for clinically stable preterm newborns (with a respiratory frequency of between 30–60 inspirations per minute, a heart rate of between 120–160 beats per minute, peripheral oxygen saturation of over 89%, absence of signs of respiratory distress, absence of cyanosis or pallor and pain.) The newborns had to tolerate food, to breathe without the use of an apparatus, and to weigh more than 1,250g.
This study included preterm newborns with gestational ages older or equal than 28 and less than 37 completed weeks of gestation (Ballard Method), hospitalized at IMIP in the Kangaroo Unit, with a corrected age less than 37 weeks at the moment of the evaluation, and who were not submitted to the kangaroo position previously. Neonates were included only when their Brazelton state during electromyographic recording was 4 or 5 (inactive alert or alert with activity).
The exclusion criteria were Apgar score less than 7 at 5min, previous history of intracranial hemorrhage (diagnosed by ultrasonography and recorded in the medical record), previous convulsion history; congenital infection, infections of the central nervous system (meningitis or encephalitis), malformations in the central nervous system; congenital cardiovascular disease, trauma during delivery; gastroesophageal reflux disease, phototherapy, and anemia.
All these inclusion and exclusion factors were evaluated using data collected from the medical records of patients evaluated by neonatologists of the Neonatal Intensive Care Unit, the Kangaroo Unit, and the Nursery.
The randomization for allocation to the kangaroo group or the control group was performed by the program R (v. 3.3.1) in which, from a list of 50 numbers (ranging from 1 to 50), a random sample of 25 numbers was drawn and indicated the order of entry in the kangaroo group. The control group was defined by the complement of this list. From the knowledge of the order of the numbers, the newborns were allocated to the groups according to the admission in the sector.
A flowchart (Fig. 1) was completed according to the recommendations of the CONSORT Statement.11
.")
For the sample calculation, this study considered the standard deviation values of the electromyographic activity of 5.0 μV for the kangaroo group and 4.0 μV for the control group according to a previous study,10 and an estimate of the minimum difference of means to be detected of 4.0 μV. The alpha error adopted was 0.05 and the power was 80%, resulting in a value of 20 children for each group.
The project was submitted to the Human Research Ethics Committee of IMIP and was approved (52381915.5.0000.5201). The clinical trial was recorded in ClinicalTrials.gov (NCT02849665 - 07/28/2016).
Data collectionThe acquisition of the electromyographic signal was performed through the electromyograph Miotool 400® (Miotec Equipamentos Biomédicos – Brazil). During collection, the infant was positioned in a high dorsal decubitus position, with a slope of approximately 30 degrees, the right side of the body in contact with the mother's abdomen, and the head resting on the left elbow fold of the mother.
The electrodes were placed in the central portion of the biceps brachii and hamstrings (in the region corresponding to the biceps femoris) of the left side of the body, positioned between the motor point and the myotendinous junction, and oriented parallel to the muscle fibers, as recommended by the Surface Electromyography for the Non-Invasive Assessment of Muscles project (SENIAM).12 The reference electrode was always placed in the lateral malleolus contralateral to the evaluated muscle. For each muscle, the records of the electromyographic activity were completed in the previously determined period of one minute.
During the recording of the electromyographic activity, the newborns remained in the states of Brazelton 4 (alert inactive) or 5 (alert with activity).13 Signal registration was initiated when the newborns remained with the assessed muscle at rest. When active movements of the newborn occurred during the recording, the electromyographic signal was rejected and a new recording was performed.
The electromyographic records were performed at three different moments (T0, T1, and T2) in both groups. In the kangaroo group, the first record (T0) was performed immediately before submitting to the kangaroo position. Immediately after this registration, the newborn was placed in the position for one hour and then the second register (T1) was conducted. After that, the newborns were kept in the kangaroo position for another hour, and then the third register was performed (T2). The kangaroo position adopted was that recommended by the Kangaroo Unit through a band that supports the newborn against the adult's thorax, in a prone and vertical position, and dressed with few pieces of clothes, thus keeping skin-to-skin contact with the mother. In the control group, the newborns were not submitted to the kangaroo position (remaining resting in a small wedge-shaped cushion at an angle of 30° relative to the horizontal plane), but the electromyographic records were performed at times corresponding to those of the kangaroo group. The electromyographic records were always made by the same researchers (KTD and RMM).
The observance of the children's permanence in the appropriate conditions for both the kangaroo group and the control group was supervised by the researchers.
Data processingThe raw electromyographic signal captured during recording in the data collection was transformed by the root mean square (RMS) function. The data processing software presents a command for this transformation. Then the data were normalized (transformation of the absolute value of the amplitude of the electromyographic signal into a relative value, in which 100% is assigned to the maximum signal peak in the recording period).13 Thus, the measure considered for the comparison of the electromyographic activity between the groups was normalized RMS. A period of 10s (windowing) of the total electromyographic reading (30s) was used.
Statistical analysisAnalysis of variance (ANOVA) for repeated measures (parametric data) or the Kruskal–Wallis test (non-parametric data) was applied to compare the means of electromyographic activity in the three recording moments in the same group. When these data were significant, multiple comparisons were made through the Tukey test in the first case and the Dunn test in the second case. Student's t-test (parametric data) and the Mann-Whitney test (non-parametric) were used, as well as the chi-squared test to compare clinical and biological characteristics among the newborns of the two groups. The Mann-Whitney test was used to compare the RMS values in the first electromyographic record (T0) between the two groups and for the two muscles studied. The alpha error for rejection of the null hypothesis was p<0.05.
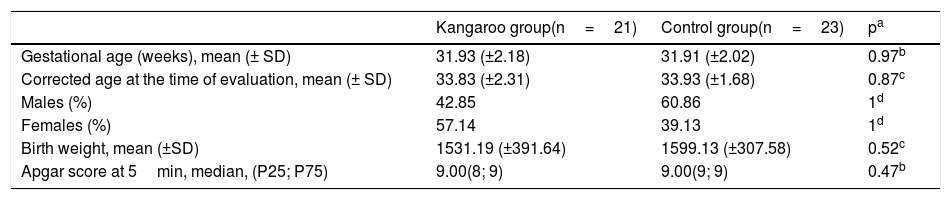
ResultsThe mothers of the newborns had an average age of 25.5 (±7.4) years and 26.2 (±6.5) years for the kangaroo group and control group, respectively. There were no significant differences between the two groups for the maternal characteristics evaluated (age, number of prenatal consultations, and type of delivery). The clinical and biological characteristics of the newborns are shown in Table 1.
Clinical and biological characteristics of the newborns.
| Kangaroo group(n=21) | Control group(n=23) | pa | |
|---|---|---|---|
| Gestational age (weeks), mean (± SD) | 31.93 (±2.18) | 31.91 (±2.02) | 0.97b |
| Corrected age at the time of evaluation, mean (± SD) | 33.83 (±2.31) | 33.93 (±1.68) | 0.87c |
| Males (%) | 42.85 | 60.86 | 1d |
| Females (%) | 57.14 | 39.13 | 1d |
| Birth weight, mean (±SD) | 1531.19 (±391.64) | 1599.13 (±307.58) | 0.52c |
| Apgar score at 5min, median, (P25; P75) | 9.00(8; 9) | 9.00(9; 9) | 0.47b |
SD, standard deviation; P, percentile.
In relation to the biceps brachii muscle (Table 2), it was observed that in the kangaroo group, there was a variation of the RMS values between the three recording moments (F (2.41)=21.24, p<0.001), with the T1 value being higher than T0 (p<0.05) and T2 higher than T1 (p<0.05). In the control group, no statistical difference was observed between the three moments evaluated (H=0.34, p=0.84).
Electromyographic activity (RMS%) of the biceps brachii of preterm newborns submitted and not submitted to the kangaroo position at different moments.
| Times | |||||
|---|---|---|---|---|---|
| Groups | T0 | T1 | T2 | p | |
| KangarooX¯ (±SD) | 10.8 (±2.4) | 16.1 (±3.8) | 19.3 (±4.9) | F21.24 | <0.001 |
| ControlMd (P25-P75) | 12.7(10.6–16.0) | 13.0(10.7–17.8) | 13.0(11.5–17.7) | H0.34 | 0.84 |
X¯, mean, SD, standard deviation; Md, median; P, percentile; T0, T1, and T2, first, second, and third moments of electromyographic recording.
RMS%, root mean square, normalized.
Kangaroo group: ANOVA with repeated measurements (F) and multiple comparisons (Tukey test): T0vs. T1 (p<0.05), T0vs. T2 (p<0.05), T1vs. T2 (p<0.05).
Control group: Kruskal–Wallis test (H).
In relation to the hamstrings (Table 3), it was observed that in the kangaroo group there was a variation of the RMS values between the three recording moments (H=11.19; p=0.004), with the T2 value being higher than T0 (p<0.05), and no significant differences were found between the values of T0 and T1, nor between T1 and T2. In the control group, no statistical difference was observed between the three moments (H=1.05, p=0.58).
Electromyographic activity (RMS%) of the hamstrings of preterm newborns submitted and not submitted to the kangaroo position at different moments.
| Times | |||||
|---|---|---|---|---|---|
| Groups | T0 | T1 | T2 | p | |
| KangarooMd (P25-P75) | 13.1(10.4–22.5) | 18.1(15.5–29.3) | 21.5(17.8–34.3) | H11.19 | 0004 |
| ControlMd (P25-P75) | 13.0(10.7–35.5) | 11.8(9.9–21.3) | 11.6(9.3–21.8) | H1.05 | 0.54 |
Md, median; P, percentile; T0, T1, and T2, first, second, and third moments of electromyographic recording.
Kangaroo group, Kruskal–Wallis test (H) and multiple comparisons (Dunn test): T0vs. T2 (p<0.05).
RMS%, root mean square, normalized.
Control group, Kruskal-Wallis test (H).
There was no statistical difference (Mann-Whitney test) for RMS values between the kangaroo group and the control group in the first electromyographic record (T0).
DiscussionThe results of this study showed that a very short time in the kangaroo position is sufficient to induce a physiological muscular response in the infant, since one hour of kangaroo position was able to increase the electromyographic activity of the biceps brachii, and the same response was observed in the hamstrings after two hours in this position. This is an important fact, because the electromyographic activity of a muscle at rest represents the state of its muscular tone.14 Thus, it was demonstrated that the flexor muscle tone of these newborns increased with the stimulus provided by the kangaroo position, an important effect, since poor muscle tone prevents the adequate postural organization of preterm newborns (PTNBs), resulting in delays of motor acquisitions and, consequently, in the motor development of these children.15
In addition, considering that the newborn full-term presents a flexor posture, with a predominance of a flexor muscle tone,16 this finding becomes even more relevant, because it shows an increase in flexor muscle tone in PTNBs. The flexor muscle tone of the newborn full-term results not only from neural maturation during fetal life17 but also from the tactile, proprioceptive, and kinesthetic stimulation promoted by the intrauterine environment, especially in the last trimester of gestation.18 Thus, the tactile and proprioceptive stimuli promoted by the kangaroo position, in addition to the position in flexion assumed during this practice, may favor flexor muscle tone in PTNBs, in the extrauterine environment, and with a very short period (1–2h) of stimulation.
Findings from previous studies evidenced the influence of a very short period (1–4h)19–21 of the kangaroo method on physiological features of the newborn, such as reduction both of heart and respiratory rates, and an increase in body temperature and oxygen saturation. However, until now there was no evidence that a very short period in the kangaroo position is also capable of inducing physiological responses in muscle activity, as evidenced by the present results. Thus, the ability of the kangaroo position to induce these changes in tone in such a short period further strengthens the need to utilize this position, but now also as an early form of motor stimulation.
The influence of kangaroo position on the electromyographic response of preterm infants had previously been studied, evidencing an increase in electromyographic activity.9,10 However, this response had been evaluated after a period equal to or longer than 24h of kangaroo position intermittently, but not continuously. The present results add the information that this response can already be observed in a very short period of the kangaroo position and they reinforce the hypothesis that an increase in muscle tone can be associated with skin-to-skin contact, and to vestibular and proprioceptive stimuli induced by this position.
Others studies22,23 support this thesis, because they have shown that multisensory stimulation of premature infants through short periods of tactile and vestibular stimuli (3–15min per day) seems to have an immediate and beneficial effect on neuromotor development,18 as well as inducing an alert behavioral state in these children.19 The effect on neuromotor development was attributed by these authors to the development of normal muscular tone, observed only in those children who received the stimuli. It is known that the vestibular system exerts influence on muscle tone and consequently on the postural control, balance, and movement of the newborn.24
Considering the age of the children studied here, it is important to emphasize that the tactile and vestibular systems are the first two sensory systems developing in the newborn, the latter being fully functional in full-term newborns.25 Thus, a motor response observed after short periods of sensory stimulation may occur due to the quick development of sensory systems which may, therefore, accelerate its maturation when receiving stimuli, even for a short period.
A limitation of this study was the absence of motor development assessment to correlate with electromyographic activity. Also, other physiological parameters such as heart rate, respiratory rate, and arterial oxygen saturation could be measured to strengthen the results.
In conclusion, the skin-to-skin contact and verticality of the infant during the kangaroo position demonstrate that this position provides several sensory inputs to the preterm newborn, contributing to the tonic-postural adjustment with a positive impact on motor development, even if it is carried out for a very short period. Therefore this intervention induces changes in the flexor function of the muscle (flexor tonus), thereby making it possible to influence the motor development of the newborn.
This is, to the best of the authors’ knowledge, the first study that has evaluated the electromyographic activity of preterm infants after a very short period of kangaroo position. Further studies are necessary to determine the clinical relevance of these findings.
FundingKaísa Trovão Diniz - Postgraduate Scholarship from Fundação de Amparo à Ciência e Tecnologia de Pernambuco (FACEPE).
Rafael Moura Miranda - Postgraduate Scholarship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
José Eulálio Cabral Filho - Research Productivity Grant from O Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq); and Chamada Universal 2014/ 458163/2014-7.
Conflicts of interestThe authors declare no conflicts of interest.
The authors wish to thank the children, parents, and especially the nursing technicians of the Kangaroo Unit at the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Recife, Brazil.
They would also like to thank the translator Técio Oliveira Macedo, Master of Arts in Linguistics, for editing the text in the English language.
Please cite this article as: Diniz KT, Cabral Filho JF, Miranda RM, Lima GM, Figueredo NP, Araújo KF. Short-time effect of the kangaroo position on electromyographic activity of premature infants: a randomized clinical trial. J Pediatr (Rio J). 2020;96:741–7.
Study conducted at Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Recife, PE, Brazil.




