

Programs for parents have been found to have a direct positive impact on reducing the consumption of psychoactive substances by adolescents, as well as having an indirect impact on reducing risk factors and increasing protective factors. The present study aimed to verify if a telehealth prevention program based on a brief motivational intervention helps to reduce parental risk practices and increase parental protective practices for drug use in comparison with psychoeducation.
MethodsA pilot randomized controlled trial was performed at the National Service of Guidance and Information on Drug Use (Ligue 132), from September 2014 to December 2015, with the parents of adolescents (n=26). The outcome measures were parental style, risk, and protective parental practices.
ResultsThe brief motivational intervention was found to be more effective than psychoeducation in reducing the negligent behavior of parents. Furthermore, when comparing pre- and post-intervention data, the brief motivational intervention helped to change parental style and the large majority of parental practices: increasing positive monitoring, as well as decreasing physical abuse, relaxed discipline, inconsistent punishment, and negative monitoring.
ConclusionsThese results demonstrate that the telehealth intervention is effective in modifying the parental practices known to help in preventing drug use. Studies with more number of subjects are required so that the results can be substantiated and generalized.
Os programas para pais parecem ter um impacto positivo direto sobre a redução do consumo de substâncias psicoativas por adolescentes, bem como um impacto indireto sobre a redução dos fatores de risco e aumento dos fatores protetores. O presente estudo visou a verificar se um programa telessaúde de prevenção com base em uma intervenção breve motivacional ajuda a reduzir as práticas de risco dos pais e aumentar as práticas protetoras com relação ao uso de drogas, em comparação à psicoeducação.
MétodosUm ensaio piloto controlado randomizado foi feito no Serviço Nacional de Informações e Orientações sobre Drogas (Ligue 132), de setembro de 2014 a dezembro de 2015, com os pais de adolescentes (n = 26). As medições dos resultados foram o estilo dos pais e as práticas de risco e protetoras dos pais.
ResultadosA intervenção breve motivacional parece ser mais eficaz do que a psicoeducação na redução dos comportamentos negligentes dos pais. Adicionalmente, quando comparada aos dados pré e pós-intervenção, a intervenção breve motivacional ajudou a mudar o estilo dos pais e a grande maioria das práticas dos pais: aumentou o monitoramento positivo e reduziu o abuso físico, disciplina permissiva, punição não condizente e monitoramento negativo.
ConclusõesEsses resultados demonstram que a intervenção telessaúde é eficaz na mudança das práticas dos pais, conhecida por ajudar a prevenir o uso de drogas. Estudos com maior número de indivíduos são necessários para que os resultados possam ser comprovados e generalizados.
Alcohol and other drugs are well known causes of morbidity, mortality, and social damage around the world, and are considered an important component of the global burden of disease.1 In this scenario, prevention programs have been used to help these young people to avoid involvement in substance abuse. Skills training programs for parents have been found to have a direct positive impact on reducing the use of psychoactive substances by adolescents, as well as an indirect impact on reducing risk factors and increasing protective factors.2,3 Monitoring, supervision, communication, support, and parental involvement are protective behaviors associated with lower rates of use of alcohol, tobacco, and other drugs.4 In contrast, negligence,5 authoritarianism, and physical abuse by parents are described as risk factors, as they have been associated with increasing the vulnerability of adolescents to drug abuse.6
Despite the knowledge that parental styles influence resilience and vulnerability to drug use by adolescents, the effectiveness of prevention programs based on parental behaviors deserve further exploration.3 Considering the need for drug prevention programs to offer training in parenting skills in their curricula, the motivational intervention (MI) can be an excellent tool to help in the behavior change processes.7 MI has been previously evidenced in the literature related to prevention programs,8 and in drug use treatments,9 including in the telehealth approach.10
In this prevention scenario, telehealth prevention programs can make an important contribution, as they offer advantages over traditional programs of drug prevention, including cost reduction, remote intervention, and the guarantee of anonymity.11 Telehealth, in the context of this article, is defined as the provision of distance services by health professionals through technological means of information transmission.12
There is considerable evidence for the effectiveness of internet interventions targeting mental health and addictions disorders.13 Promising studies indicate that existing telehealth prevention programs for adolescents in schools have the potential to reduce drug use.14 A recent systematic review showed that there is evidence for computer-based delivery of parental interventions for alcohol use prevention.15 A family program that features the mailing of booklets with follow-up telephone calls significantly reduced the prevalence of smoking cigarettes and drinking alcohol among adolescents,16 as well as a computer-based prevention program for parents that reduced adolescent alcohol use and risky behaviors.17 Although the emerging evidence demonstrating that telehealth prevention programs for drug use among adolescents is an area of increasing promise, further replication work is required in order to determine their broader impact.18
Here, the objective is to present a pilot study of a randomized clinical trial performed to evaluate the feasibility and preliminary efficacy of a telehealth prevention program based on a brief motivational intervention (BMI) to help reduce parental risk practices and increase parental protective practices for drug use, in comparison with psychoeducation (PE).
MethodsThis article is a pilot study of a randomized controlled trial using telehealth methodology. Data collection was performed at the National Service of Guidance and Information on Drug Use (Ligue 132), from September 2014 to December 2015. This telehealth service is a toll free, anonymous telephone line that can be accessed by the Brazilian population. The study included 26 parents of adolescents, aged 10 to 18, who called “Ligue 132” seeking a drug use prevention program and agreed to participate after reading the Informed Consent. The study excluded the parents of adolescents who had difficulties understanding the questions and the parents who reported drug use problems.
ProceduresThe prevention program “Ligue 132” was launched and publicized through the Internet, television, newspaper, and through letters sent to schools. Parents who were interested in participating and called to the service were randomized through a specific software package developed for the program into the Psychoeducation (PE) group or the BMI group. The assessments were administered (pre- and post-intervention) in the control and experimental intervention by telephone. All procedures were performed by consultants who were supervised by masters and doctoral students, all of whom were from the healthcare system. As described elsewhere,19 the training of the consultants was based on drug abuse and BMI knowledge with practical training hours. All consultants were evaluated regarding the quality of BMI, using the BECCI scale (Behaviour Change Counselling Index).20
Participants were informed about the research through a free and informed consent form. The study was approved by the Ethics Committee of Federal University of Health Sciences of Porto Alegre (No. 27079814.5.0000.5345) and registered as a Clinical Trial (No. NCT02386280).
InterventionsThe theoretical nature of the program was based on a complex model that integrates the well documented knowledge about parental risk and protection practices,21 and integrates theories such as social learning theory,22 and a motivational tele-intervention model to change the codependent behavior of family members of drug users.23 The theory of social development suggests that adolescents learn behavior patterns, such as drug use, through their first models of socialization.22 The motivational tele-intervention model is based on the theoretical perspective on motivational intervention7 and stages of change.24
The first contact of the parents was reactive in both groups. The parents spontaneously called the service seeking help to prevent the use of drugs by their teen children. In this first call, the nature of the prevention program was explained, and then the baseline assessments were administered (pre-intervention). Once randomized, the first intervention was performed according to the group (BMI or PE). Subsequent calls were scheduled for later dates, and the follow-up calls were made proactively by the service. The dates scheduled for the subsequent interventions were seven and 14 days after the first call (considered the baseline of the study). Twenty-eight days after the first assessment, the follow up measures were collected in order to assess the subsequent change in parental practices and style. The parents were blinded to the interventions carried out. The consort diagram (Fig. 1) provides an outline of the procedures, as well as participant enrollment and retention data.
- •
PE group: the control group received the usual service intervention, which consists of a psychoeducational intervention, aimed only at informing parents about general aspects concerning the prevention of drug use in adolescence. Specific information was provided on each day of the follow-up. Information included the damage of drug use in adolescence, as well as parental protective and risk practices through reading informational materials.
- •
BMI group: In the experimental group, a brief motivational intervention was performed with the aim of helping parents to change their behavior in order to increase parental protective practices and decrease parental risk practices.7 BMI was applied to change parental practices according to the transtheoretical model of motivational stages of change.24 According to the analysis of parental practices (as measured by the PSI scale), the telephone consultants helped parents to modify risk behaviors by BMI with individually-tailored approaches according to the stage of change by BMI main components: expressing empathy, reflective listening, avoiding argumentation, supporting self-efficacy, developing discrepancy, individualized feedback, and evocation of the reasons for the change.7
- •
Booster mailing: After the first call, a booster brochure called “Drugs: Primer for Parents of Teens” prepared by the National Drug Policy was sent to the study participants in both groups. This brochure provides information about drugs in general and the actions that can be taken by parents so that adolescents are less likely to abuse drugs in the future.
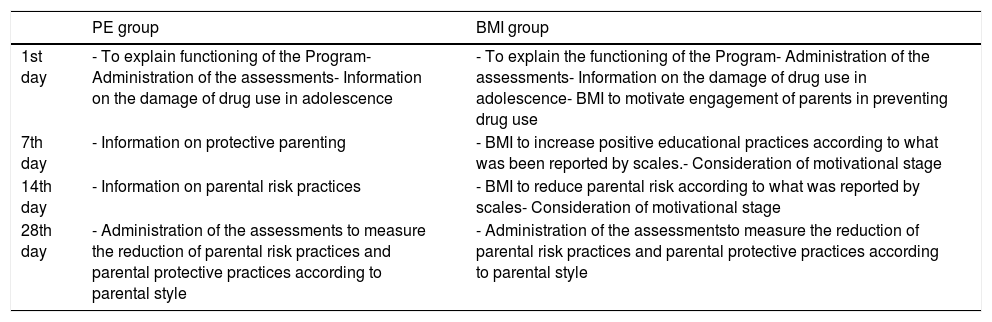
The objectives of the interventions of each day are detailed in Table 1.
Table 1.Objectives of the phases based on days of follow-up in the control psychoeducational (PE) group and in the brief motivational intervention (BMI) group.
PE group BMI group 1st day - To explain functioning of the Program- Administration of the assessments- Information on the damage of drug use in adolescence - To explain the functioning of the Program- Administration of the assessments- Information on the damage of drug use in adolescence- BMI to motivate engagement of parents in preventing drug use 7th day - Information on protective parenting - BMI to increase positive educational practices according to what was been reported by scales.- Consideration of motivational stage 14th day - Information on parental risk practices - BMI to reduce parental risk according to what was reported by scales- Consideration of motivational stage 28th day - Administration of the assessments to measure the reduction of parental risk practices and parental protective practices according to parental style - Administration of the assessmentsto measure the reduction of parental risk practices and parental protective practices according to parental style

- •
Feasibility: Feasibility was assessed based on the number of families enrolled in the study and the number who completed the prevention intervention.
- •
Distribution of sociodemographic data: A computerized general protocol of the Service (unregistered software that also contains tools for gauging the study variables, which will be queried during the phone call) was used to provide general user data such as gender, age, marital status, occupation, family income, education level, and state, as well as data on question classification, including treatment centers, drug information, informative material, and the drugs that have been abused by the service user.
- •
Parental style and practices: The parental styles inventory (PSI) was used to assess parental style, referring to the strategies and techniques used by parents to educate their children through seven parental practices style. Five of these were related to the development of risk behaviors: negligence, inconsistent punishment, relaxed discipline, negative monitoring, and physical abuse; two were related to the development of protective behaviors: moral behavior and positive monitoring. Neglect occurs when parents are not attentive to the needs of their children, are absent from their responsibilities, and interact without affection. Inconsistent punishment is when parents punish or reinforce the behavior of their children according to their mood, and is not contingent on the child's behavior. Negative monitoring is characterized by excessive parental supervision over their children's lives and a large number of intrusive actions. Physical abuse occurs when parents hurt or cause pain to their children on the grounds of educating them. Positive monitoring is defined as the set of parental practices that involve affection, attention, and knowledge of parents about their child. Moral behavior refers to the transmission of values such as honesty, generosity, and a sense of justice to the children. The inventory consists of 42 questions, each one consisting of a phrase to which the father/mother replies, indicating the frequency with which he or she acts according to the situation described in the sentence. The answer is based on recalling about ten occasions: never, if they never have acted in such a way; zero to twice; sometimes, if on ten occasions they acted in such a way from three to seven times; and always, if on ten occasions they acted in such a way from eight to ten times. The scores obtained through the answers are transformed into a parental style index, with a score ranging from 1 to 99.25
- •
Stage of motivation: the Contemplation Ladder Scale was used to evaluate the stage of motivation for parental behavior changes, through five statements. Each statement indicates a stage of readiness to change, such as pre-contemplation, contemplation, preparation, and action.26
Data were recorded in a software package and later transferred to a Microsoft Excel spreadsheet. Analysis was conducted using SPSS, version 19.0.
Quantitative data were described as medians and percentiles (25–75), while qualitative data were measured in absolute and percentage frequency. Comparison of categorical variables was performed using the chi-squared test, and the continuous variables were compared using the nonparametric test for independent samples, and the Mann–Whitney, Kolmogorov–Smirnov, and Wilcoxon tests. The data were considered statistically different when the p-value was under 0.05.
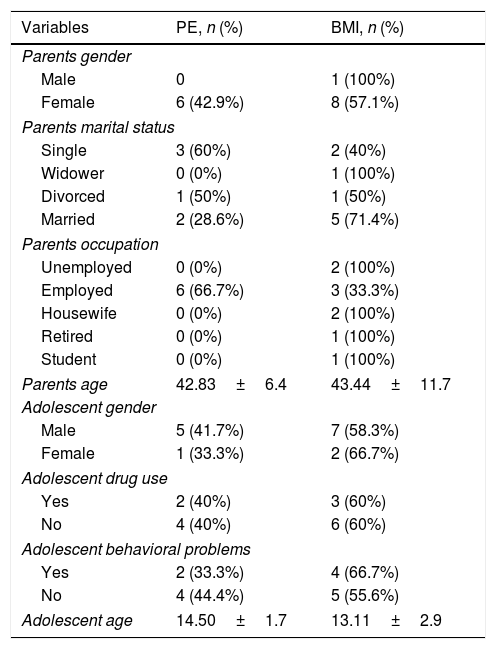
ResultsThe final data to be used for the analyses were composed of 15 parents of adolescents, divided into the control (n=6) and BMI (n=9) groups. There were seven losses in the follow-up of the control group and a lower number (n=4) in the BMI group. Mothers predominated (93%), mean age was 43.6 years, 46.6% were married, and 60% were employed. Regarding the teens, males were predominant (80%) and the mean age was 13.6. According to parental reports, a significant number of teenagers (33.3%) had already experienced drug use or there was a suspicion that they had used some type of drug, marijuana being the most prevalent (48%). Furthermore, many parents described their children as already presenting behavioral problems (40%). Table 2 shows the socio-demographic data of the BMI and control groups, with no significant differences between the two randomized groups at baseline.
Comparison of the distribution of sociodemographic data in BMI (n=9) and PE (n=6) groups.
| Variables | PE, n (%) | BMI, n (%) |
|---|---|---|
| Parents gender | ||
| Male | 0 | 1 (100%) |
| Female | 6 (42.9%) | 8 (57.1%) |
| Parents marital status | ||
| Single | 3 (60%) | 2 (40%) |
| Widower | 0 (0%) | 1 (100%) |
| Divorced | 1 (50%) | 1 (50%) |
| Married | 2 (28.6%) | 5 (71.4%) |
| Parents occupation | ||
| Unemployed | 0 (0%) | 2 (100%) |
| Employed | 6 (66.7%) | 3 (33.3%) |
| Housewife | 0 (0%) | 2 (100%) |
| Retired | 0 (0%) | 1 (100%) |
| Student | 0 (0%) | 1 (100%) |
| Parents age | 42.83±6.4 | 43.44±11.7 |
| Adolescent gender | ||
| Male | 5 (41.7%) | 7 (58.3%) |
| Female | 1 (33.3%) | 2 (66.7%) |
| Adolescent drug use | ||
| Yes | 2 (40%) | 3 (60%) |
| No | 4 (40%) | 6 (60%) |
| Adolescent behavioral problems | ||
| Yes | 2 (33.3%) | 4 (66.7%) |
| No | 4 (44.4%) | 5 (55.6%) |
| Adolescent age | 14.50±1.7 | 13.11±2.9 |
PE, psychoeducation; BMI, brief motivational intervention.
Note: The data were presented as a percentage n, and mean age and standard deviation.
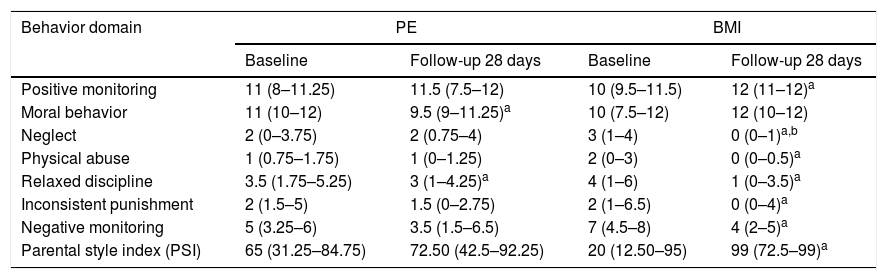
As seen in Table 3, the parental style index of the BMI group improved significantly more than the PSI of the control group, when comparison of pre- and post-interventions were analyzed, although a statistically significant difference between the groups was not observed due to the great variability of PSI scores in both groups. The comparison between pre- (day 1) and post-intervention (day 28) showed a statistically significant difference in the large majority of parental practices in the BMI group, besides the parental style index. There was a reduction in risk practices such as neglect, physical abuse, relaxed discipline, inconsistent punishment, and negative monitoring. There was also an increase in the protective practice of positive monitoring. In the PE group, a statistically significant difference was found for the parental practice of relaxed discipline, which declined from pre- to post-intervention. Also in the PE group, the protective practice of moral behavior exhibited a reduction (Table 3). In terms of motivational stages, 80% of the parents were at the preparation or action stage when they first called, and the same percentage was identified at the final call (28 days of follow-up).
Comparison of parental practices between BMI and PE (n=15).
| Behavior domain | PE | BMI | ||
|---|---|---|---|---|
| Baseline | Follow-up 28 days | Baseline | Follow-up 28 days | |
| Positive monitoring | 11 (8–11.25) | 11.5 (7.5–12) | 10 (9.5–11.5) | 12 (11–12)a |
| Moral behavior | 11 (10–12) | 9.5 (9–11.25)a | 10 (7.5–12) | 12 (10–12) |
| Neglect | 2 (0–3.75) | 2 (0.75–4) | 3 (1–4) | 0 (0–1)a,b |
| Physical abuse | 1 (0.75–1.75) | 1 (0–1.25) | 2 (0–3) | 0 (0–0.5)a |
| Relaxed discipline | 3.5 (1.75–5.25) | 3 (1–4.25)a | 4 (1–6) | 1 (0–3.5)a |
| Inconsistent punishment | 2 (1.5–5) | 1.5 (0–2.75) | 2 (1–6.5) | 0 (0–4)a |
| Negative monitoring | 5 (3.25–6) | 3.5 (1.5–6.5) | 7 (4.5–8) | 4 (2–5)a |
| Parental style index (PSI) | 65 (31.25–84.75) | 72.50 (42.5–92.25) | 20 (12.50–95) | 99 (72.5–99)a |
PE, psychoeducation; BMI, brief motivational intervention.
Note: The data were presented by median and n percentile.
The feasibility of the research protocol was assessed based on the 26 parents enrolled in the study and on the 15 parents who completed the follow-up assessment at 28 days. Considering the great number of losses during the follow up, analysis of the results was performed per protocol. In fact, the telehealth prevention protocol to change parental behaviors is feasible, short, and may reach parents in a wide area, if they have access to a phone. It is of utmost importance to increase the motivation of more parents to understand their role in the child behaviors, and to seek for help and advice in order to prevent the teenagers from the precocious use of legal and illegal drugs.
DiscussionThis exploratory pilot study is the first that the authors are aware of to examine if BMI, when compared to psychoeducation, helps to reduce the parental risk practices and increase the parental protective practices involved in the prevention of adolescent drug use. Compared with those from the control group, the parents in the BMI group improved their parental style index when contrasted with the baseline, which did not occur in the control group. Although less effective than BMI, psychoeducation can also act to diminish parental risk practices and increase protective parenting. Therefore, the differences between the groups were not significant. A larger sample is needed to verify if the BMI is in fact more effective. Prior studies have observed that motivational intervention has promising results with respect to changes in behavior in general: helping young people to avoid involvement with drugs8; motivating drug users to stop or reduce consumption,9 and assisting the families of drug addicts to modify their permissive behavior.23
In terms of the parental practice of neglect, the BMI was found to be more effective at reducing this practice than PE, with a statistically significant difference between the two. This result is of great importance, as the negligent behavior of parents has been demonstrably associated with increased vulnerability to drug use in several studies.6 Therefore, it may be expected that a program that helps parents to reduce neglect toward their children may play an important role in the prevention of drug use.
The parental style index and the large majority of parental practices are changed by BMI, showing that this intervention is effective at modifying parental practices in order to favor styles thought to help in preventing drug use by youngsters. According to a previous study, parental monitoring is strongly associated with the reduced use of drugs, especially when associated with affection and interest in the activities of adolescents.4 Negative parental practices are more associated with parents of children that demonstrate behavioral problems, such as aggressiveness, impulsivity, and drug abuse.6 Therefore, the findings of this pilot study indicate that BMI has a greater potential for reducing the risk factors and increasing the protective factors of drug use involved in the educational attitudes of parents.
The present study had some limitations, notably considering the feasibility of such a program. Feasibility was assessed based on the number of families contacted to enroll in the study and the number who completed the prevention intervention. The initially proposed sample size was not achieved, mainly due to problems in the recruitment and in the retention of parents on the follow-up dates. Other authors have described the same difficulties in their studies, as the rates of families recruited for family-focused prevention are typically low.27 To avoid bias, it is necessary to think about new recruitment strategies, such as partnership with institutions the subjects are familiar with, and building on cross-institutional support. The most important issue regarding this subject is that families need to feel confident about participating in the program.28 Furthermore, telephone contact represents a simple resource, as it does not tend to generate a sense of obligation in the participants to continue participating in the intervention.10 According to a systematic review with telemedicine services, up to 70% losses are expected during the program.29 This small sample size does not allow the generalization of the results, and even though some differences are already apparent with the small group of parents, increasing the enrollment of more parents, both mothers and fathers, with a more homogeneous sociodemographic distribution and complete participation are the objective of a full randomized trial. Since the study had less than one month of follow-up, it was not possible to assess whether the intervention had an impact on the drug use of the adolescents. However, studies have shown that an increase in parental behavioral protection factors may be directly responsible for a decrease in the use of drugs by teenagers of 5–10%.30
In conclusion, the present study provides some evidence for using BMI to decrease risk practices and increase protective practices in parents seeking to prevent the use of drugs by their children. It is suggested that further studies are carried out focusing on the problems of recruitment and retention, so that larger samples can be analyzed.
FundingFunding for this study was provided by Secretaria Nacional de Políticas Sobre Drogas—SENAD. SENAD had no role in the study design, collection, analysis, or interpretation of the data, writing of the manuscript, or the decision to submit the paper for publication.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Valente JY, Moreira TC, Ferigolo M, Barros HM. Randomized clinical trial to change parental practices for drug use in a telehealth prevention program: a pilot study. J Pediatr (Rio J). 2019;95:334–41.




