

this study aimed to evaluate the usefulness of current radiographic measurements, which were originally conceived to evaluate adenoid hypertrophy, as potential referral parameters.
Methodschildren aged from 4 to 14 years, of both genders, who presented nasal obstruction complaints, were subjected to cavum radiography. Radiographic examinations (n = 120) were evaluated according to categorical and quantitative parameters, and data were compared to gold-standard videonasopharyngoscopic examination, regarding accuracy (sensitivity, negative predictive value, specificity, and positive predictive value).
Resultsradiographic grading systems presented low sensitivity for the identification of patients with two-thirds choanal space obstruction. However, some of these parameters presented relatively high specificity rates when three-quarters adenoid obstruction was the threshold of interest. Amongst the quantitative variables, a mathematical model was found to be more suitable for identifying patients with more than two-thirds obstruction.
Conclusionthis model was shown to be potentially useful as a screening tool to include patients with, at least, two-thirds adenoid obstruction. Moreover, one of the categorical parameters was demonstrated to be relatively more useful, as well as a potentially safer assessment tool to exclude patients with less than three-quarters obstruction, to be indicated for adenoidectomy.
o objetivo deste estudo foi de investigar a utilidade de medidas radiográficas destinadas à avaliação da tonsila faríngea a serem utilizadas como potenciais parâmetros de encaminhamento.
Métodoscrianças de quatro a 14 anos, de ambos os gêneros, que apresentavam queixas referentes à obstrução nasal foram submetidas à radiografia do cavum. Os registros radiográficos (n=120) foram avaliados de acordo com parâmetros categóricos e quantitativos, e dados resultantes foram comparados ao exame padrão-ouro de videonasofaringoscopia, em relação às suas taxas de acurácia (sensibilidade, valor preditivo negativo, especificidade e valor preditivo positivo).
Resultadosos parâmetros radiográficos categóricos apresentaram baixa sensibilidade para a identificação de pacientes portadores de ⅔ de obstrução do espaço coanal. No entanto, alguns destes parâmetros apresentaram especificidades relativamente altas quando ¾ de obstrução coanal era o ponto de corte de interesse. Dentre as variáveis quantitativas, um modelo matemático se mostrou mais adequado para identificar pacientes com mais de ⅔ de obstrução coanal.
Conclusãoeste modelo demonstrou, assim, ser potencialmente útil como método de rastreamento para identificação de pacientes com pelo menos ⅔ de obstrução adenoidiana. Além disso, um dos parâmetros categóricos analisados demonstrou ser relativamente mais útil e potencialmente seguro para eliminar pacientes queixosos com menos de ¾ de obstrução a serem indicados à adenoidectomia.
Mouth breathing is highly prevalent among children of all ages,1–3 and it is frequently caused by obstructive hypertrophied adenoids.3–5 Even though pediatricians are responsible for most of the child referrals to otolaryngologic secondary care, diagnosis agreement between both levels of care is extremely low in cases of adenoid enlargement.6 Since pediatricians rarely perform videonasopharyngoscopic examination (VNP), but cavum X-ray is the most frequently required otolaryngologic complementary exam in the public health system,7 it is justifiable to investigate the usefulness of cavum X-ray on adenoid assessment.
Although this topic has been extensively debated over the years,4,8–12 the usefulness of lateral cavum X-ray is still unclear. This uncertainty might be related to the absence of comprehensive studies that simultaneously investigate a considerable number of radiographic parameters.13,14
Therefore, the aim of this study was to evaluate current radiographic adenoid assessment methods in comparison to gold standard VNP examination, and to present potentially useful radiographic referral methods.
MethodsThis was a cross-sectional methodological study, and was approved by the institutional ethics review board (protocol 0181/08).
In order to compose the study sample, 170 children from a public pediatric otolaryngologic referral center, ages ranging from 4 to 14 years, were invited to participate. Of these, 43 refused to participate. An informed consent was obtained from all the participants, after detailed description of the procedures and proper explanation of the study objective, risks, discomforts, and benefits.
In order to meet the inclusion criteria, patients must have presented complaints of nasal obstruction or oral breathing suspected to be caused by adenoid hypertrophy. Children with congenital syndromes or head and neck malformations were excluded. Subjects with acute infection of the respiratory tract or with history of previous adenoidectomy were also excluded.
Initially, all children were submitted to a radiographic exam of the cavum, which was performed by a single radiology specialist. Focus-film distance was 140cm, and X-ray exposure settings were 70kV, 12mA, for 0.40 to 0.64seconds. During radiographic examination, patients were standing, and instructed to breathe exclusively through the nose and to keep their lips gently sealed. Central X-ray beam was directed toward the nasopharyngeal anatomic area. Radiographic exams showing elevation of the soft palate or significant rotation of the head were discarded.
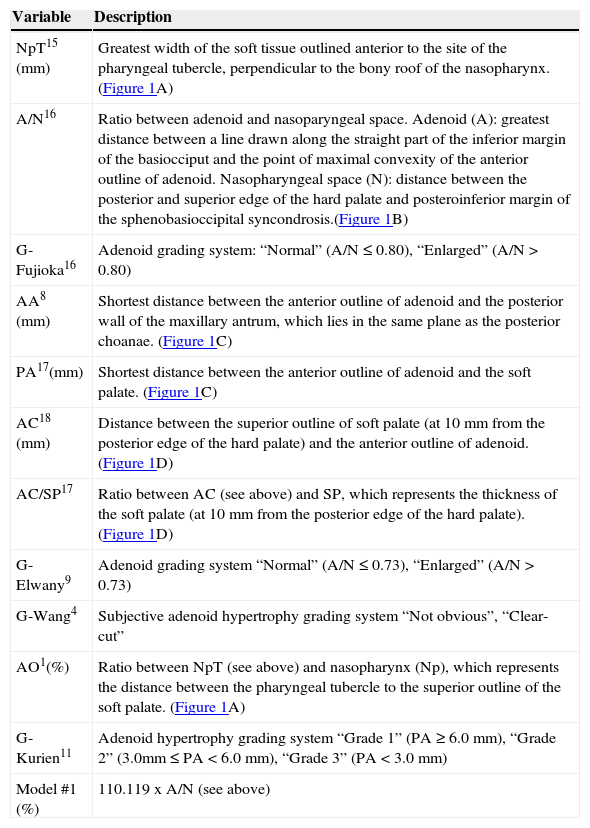
Lateral radiographies were number-coded and hand-traced by one of the researchers, who was unaware of the subjects’ identities as well as their clinical conditions and complaints. The examiner performed several radiographic categorical and quantitative measurements (Table 1,15–18Figure 1), which were already proven to be satisfactorily reproducible.19 Tracings were performed with a negatoscope upon acetate films. Linear measurements were determined with a digital caliper (Starret™ 799A-8/200).
Radiographic assessment measurements.
| Variable | Description |
|---|---|
| NpT15 (mm) | Greatest width of the soft tissue outlined anterior to the site of the pharyngeal tubercle, perpendicular to the bony roof of the nasopharynx. (Figure 1A) |
| A/N16 | Ratio between adenoid and nasoparyngeal space. Adenoid (A): greatest distance between a line drawn along the straight part of the inferior margin of the basiocciput and the point of maximal convexity of the anterior outline of adenoid. Nasopharyngeal space (N): distance between the posterior and superior edge of the hard palate and posteroinferior margin of the sphenobasioccipital syncondrosis.(Figure 1B) |
| G-Fujioka16 | Adenoid grading system: “Normal” (A/N ≤ 0.80), “Enlarged” (A/N > 0.80) |
| AA8 (mm) | Shortest distance between the anterior outline of adenoid and the posterior wall of the maxillary antrum, which lies in the same plane as the posterior choanae. (Figure 1C) |
| PA17(mm) | Shortest distance between the anterior outline of adenoid and the soft palate. (Figure 1C) |
| AC18 (mm) | Distance between the superior outline of soft palate (at 10mm from the posterior edge of the hard palate) and the anterior outline of adenoid. (Figure 1D) |
| AC/SP17 | Ratio between AC (see above) and SP, which represents the thickness of the soft palate (at 10mm from the posterior edge of the hard palate). (Figure 1D) |
| G-Elwany9 | Adenoid grading system “Normal” (A/N ≤ 0.73), “Enlarged” (A/N > 0.73) |
| G-Wang4 | Subjective adenoid hypertrophy grading system “Not obvious”, “Clear-cut” |
| AO1(%) | Ratio between NpT (see above) and nasopharynx (Np), which represents the distance between the pharyngeal tubercle to the superior outline of the soft palate. (Figure 1A) |
| G-Kurien11 | Adenoid hypertrophy grading system “Grade 1” (PA ≥ 6.0mm), “Grade 2” (3.0mm ≤ PA < 6.0mm), “Grade 3” (PA < 3.0mm) |
| Model #1 (%) | 110.119 x A/N (see above) |
AA, antroadenoid diameter; AC, air column; AC/SP, air column/soft palate ratio; A/N, adenoid/nasopharyngeal ratio; AO, airway occlusion; G-Elwany, Elwany grading system; G-Fujioka, Fujioka grading system; G-Kurien, Kurien grading system; G-Wang, Wang grading system; NpT, nasopharyngeal tonsil; PA, palatal airway.
 NpT, nasopharyngeal tonsil; Np, nasopharynx. (B) A, adenoid; N, nasopharyngeal space. (C) AA, antroadenoid; PA, palatal airway. (D) AC, air column; SP, soft palate.")
On the same day, the selected sample was submitted to VNP, which was performed by experienced otolaryngologists. The examination was performed with a flexible fiberoptic nasopharyngoscope (Olympus™ ENFP4, 3.4mm), with a 250-watt halogen light. All exams were performed after topical anesthesia (lidocaine 2%) in both nostrils. At any sign of discomfort, the exam was interrupted.
All exams were recorded and then edited to preserve the identification of the patient. The edited VNP clips were number-coded, and then handed to another examiner, an experienced otolaryngologist not involved with the subjects’ enrollment, VNP performance, or the recording and editing of exams. The examiner was also unaware of the radiographic examination outcomes and the subjects’ respiratory symptoms and complaints.
In order to evaluate the VNP clips, the measured choanal obstruction (MCO), a reproducible assessment method designed to quantify the degree of obstruction caused by the adenoid tissue, was used.19 The examiner was instructed to choose the frame that would provide the best view of the adenoid in relation to the choana, obtained from the most distal portion of the inferior turbinate. In these frames, the patient should be inspiring exclusively through the nose, with no evidence of soft palate elevation. The selected frame was then converted into a digital file (JPEG format), and the MCO was finally calculated as the percentage of the choanal area occupied by the adenoid tissue, using the image processing software Image J.20, If images from both nostrils were available, the average between the right and left sides evaluations was calculated in order to minimize occasional variations, as previously recommended.19
Data analysisInitially, the sample was described according to the demographic data, respiratory complaints and the research variables. Optimal cut-off points were chosen for each of the quantitative variables (nasopharyngeal tonsil [NpT], adenoid/nasopharyngeal ratio [A/N], antroadenoid diameter [AA], palatal airway [PA], air column [AC], air column/soft palate ratio [AC/SP], airway occlusion [AO], and Model #1), according to receiver operating characteristic (ROC) curve analysis.21 Subsequently, sensitivity, specificity, and positive and negative predictive values were calculated for each of the quantitative and categorical radiographic parameters (G-Fujioka, G-Elwany, G-Wang, and G-Kurien).
Specific gold-standard MCO cut-off points were used for these calculations (66.67%, 75.00%). Such thresholds represent cut-off points used to identify patients with pathological hypertrophic adenoid22 and candidates for adenoidectomy,23 respectively. Sensitivity, as well as negative predictive value, was calculated considering a VNP threshold of 66.67%; specificity and positive predictive value were calculated for a VNP threshold of 75.00%.
All calculations and analysis were performed using the Statistical Package for Social Sciences (SPSS), version 13.0.
ResultsFrom the initial 127 patients, seven patients were excluded due to the poor quality of the cavum X-ray or VNP. VNP bilateral examination was not performed on 32/120 subjects (26.66%), who had MCO values derived from a single nostril evaluation.
The final sample was composed of 120 subjects (females: 59, 49.16%; males: 61, 50.83%), and the mean age was 9.45 years (standard deviation: 2.45; range: 4.08-14.33). Nasal breathing was reported by seven subjects (5.83%), while exclusive oral breathing was reported by 56 subjects (46.66%); 57 subjects (47.50%) reported mixed (oral/nasal) breathing. The majority of the sample (99, 82.50%) was composed of patients with nasal obstruction complaints; most of whom described the obstruction as bilateral (63/99), and irregular (69/99). According to the reports, 107 (89.16%) children experienced frequent snoring, and 61 children (50.83%) experienced airway interruptions during sleep.
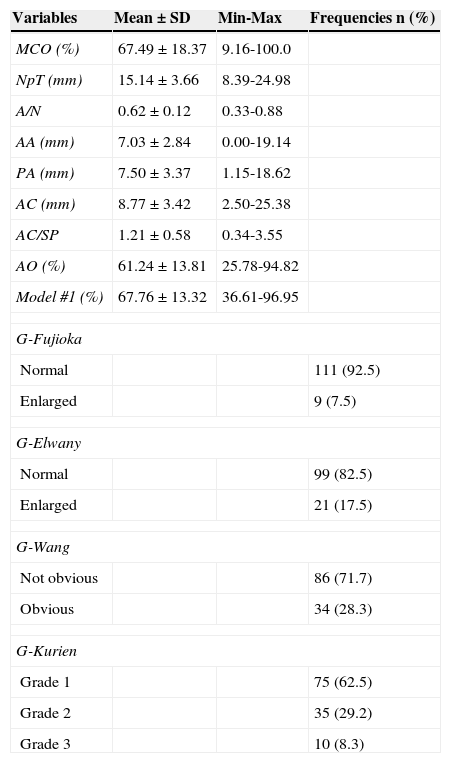
Table 2 presents the MCO description, as well as the descriptive analysis of the quantitative and categorical radiographic parameters.
Descriptive analysis of the MCO, and quantitative and categorical radiographic parameters.
| Variables | Mean±SD | Min-Max | Frequencies n (%) |
|---|---|---|---|
| MCO (%) | 67.49±18.37 | 9.16-100.0 | |
| NpT (mm) | 15.14±3.66 | 8.39-24.98 | |
| A/N | 0.62±0.12 | 0.33-0.88 | |
| AA (mm) | 7.03±2.84 | 0.00-19.14 | |
| PA (mm) | 7.50±3.37 | 1.15-18.62 | |
| AC (mm) | 8.77±3.42 | 2.50-25.38 | |
| AC/SP | 1.21±0.58 | 0.34-3.55 | |
| AO (%) | 61.24±13.81 | 25.78-94.82 | |
| Model #1 (%) | 67.76±13.32 | 36.61-96.95 | |
| G-Fujioka | |||
| Normal | 111 (92.5) | ||
| Enlarged | 9 (7.5) | ||
| G-Elwany | |||
| Normal | 99 (82.5) | ||
| Enlarged | 21 (17.5) | ||
| G-Wang | |||
| Not obvious | 86 (71.7) | ||
| Obvious | 34 (28.3) | ||
| G-Kurien | |||
| Grade 1 | 75 (62.5) | ||
| Grade 2 | 35 (29.2) | ||
| Grade 3 | 10 (8.3) | ||
AA, antroadenoid diameter; AC, air column; AC/SP, air column/soft palate ratio; A/N, adenoid/nasopharyngeal ratio; AO, airway occlusion; G-Elwany, Elwany grading system; G-Fujioka, Fujioka grading system; G-Kurien, Kurien grading system; G-Wang, Wang grading system; MCO, measured choanal obstruction; Min-Max, minimal to maximum; NpT, nasopharyngeal tonsil; PA, palatal airway; SD, standard deviation.
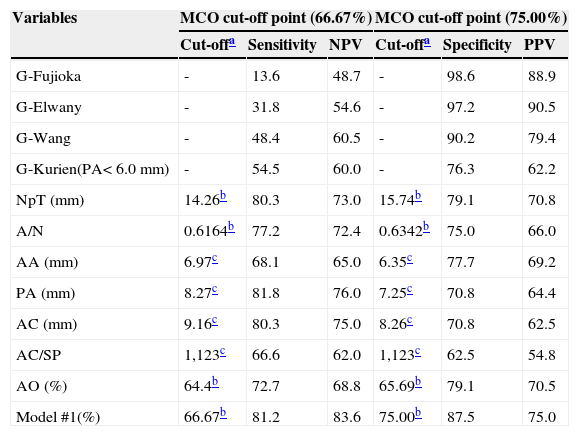
The categorical parameters G-Fujioka, G-Elwany, G-Wang, and G-Kurien produced poor sensitivity and negative predictive value for the MCO cut-off point of 66.67%. However, excellent specificity and positive predictive values were presented by most of the categorical parameters for the MCO cut-off point of 75.00% (Table 3).
Valuation of the cut-off points, sensitivity, and specificity of the radiographic parameters in relation to MCO cut-off points.
| Variables | MCO cut-off point (66.67%) | MCO cut-off point (75.00%) | ||||
|---|---|---|---|---|---|---|
| Cut-offa | Sensitivity | NPV | Cut-offa | Specificity | PPV | |
| G-Fujioka | - | 13.6 | 48.7 | - | 98.6 | 88.9 |
| G-Elwany | - | 31.8 | 54.6 | - | 97.2 | 90.5 |
| G-Wang | - | 48.4 | 60.5 | - | 90.2 | 79.4 |
| G-Kurien(PA<6.0mm) | - | 54.5 | 60.0 | - | 76.3 | 62.2 |
| NpT (mm) | 14.26b | 80.3 | 73.0 | 15.74b | 79.1 | 70.8 |
| A/N | 0.6164b | 77.2 | 72.4 | 0.6342b | 75.0 | 66.0 |
| AA (mm) | 6.97c | 68.1 | 65.0 | 6.35c | 77.7 | 69.2 |
| PA (mm) | 8.27c | 81.8 | 76.0 | 7.25c | 70.8 | 64.4 |
| AC (mm) | 9.16c | 80.3 | 75.0 | 8.26c | 70.8 | 62.5 |
| AC/SP | 1,123c | 66.6 | 62.0 | 1,123c | 62.5 | 54.8 |
| AO (%) | 64.4b | 72.7 | 68.8 | 65.69b | 79.1 | 70.5 |
| Model #1(%) | 66.67b | 81.2 | 83.6 | 75.00b | 87.5 | 75.0 |
AA, antroadenoid diameter; AC, air column; AC/SP, air column/soft palate ratio; A/N, adenoid/nasopharyngeal ratio; AO, airway occlusion; G-Elwany, Elwany grading system; G-Fujioka, Fujioka grading system; G-Kurien, Kurien grading system; G-Wang, Wang grading system; MCO, measured choanal obstruction; NpT, nasopharyngeal tonsil; NPV, negative predictive value; PA, palatal airway; PPV, positive predictive value.
Original and “ideal” cut-off points are presented for all of the quantitative radiographic parameters (Table 3). The following analysis demonstrated diverse sensitivity, specificity, and positive and negative predictive values; however, relatively higher rates were demonstrated when the threshold of 66.67% was considered (Table 3).
DiscussionAfter many attempts,4,8–12 this research has finally performed a comprehensive evaluation of the current radiographic parameters4,8–11,15,16 intended to evaluate adenoid hypertrophy. In order to do so, this investigation has selected the VNP as the gold standard to be compared to the cavum X-ray exam, as recommended by the relevant literature.10,24–26 Besides, the inclusion criteria adopted by this study have necessarily created a characteristic sample which accurately represents the population from whom complementary exams, such as the cavum X-ray, are usually required, i.e. subjects suspected to have adenoid hypertrophy. Moreover, this research has satisfied other essential27–29 methodological requirements, such as examiners blinded to the subjects’ symptoms and complaints, as well as to the other examination outcomes; comprehensive description of the exams; and the moment in time they were performed. Such features have assured good scientific reliability for the evidence provided by this study.
The choice of calculating sensitivity rates for 66.67% of choanal obstruction was motivated by the selection of an assessment tool for screening purposes, i.e. to identify, as much as possible, individuals suffering from pathological22 adenoid enlargement. However, if a given test tends to present higher sensitivity rates, more positive test results are obtained; as a consequence, several healthy patients might be erroneously categorized as ill.30 Yet, high sensitivity is still desirable for screening purposes, since the consequence of a false-negative test result (lack of referral to secondary care), may be mostly avoided.
Particularly, G-Fujioka and G-Elwany, two grading systems based on A/N, could not reasonably recognize patients with ⅔ (MCO cut-off point: 66.67%), since sensitivity values were low for both parameters. Wormald and Prescott12 have also observed low sensitivity for G-Fujioka (41.0%) when this system was used to identify individuals with MCO higher than 60.00%.
Another grading system (G-Wang), based upon subjective criteria, presented similar results as the objective parameters mentioned above (G-Fujioka and G-Elwany). The inability of this system to identify patients who require otolaryngologic attention, in addition to its dependency on the examiners’ subjective judgment, makes it clinically unsuitable. Although Wang et al.4 have found a significant association between G-Wang and adenoid dimension, an “eyeball” radiographic evaluation, even less time-consuming, might not be preferred.
The G-Kurien system, though originally conceived to categorize patients among three classes,11 was also tested for its accuracy. Individuals with PA higher than 6.0mm (“Grade 3” hypertrophy) were considered to be radiographic positives. According to the results, low rates of sensitivity were obtained. In addition, Kurienet al.11 had already reported low agreement between G-Kurien and similar VNP categorization.
Due to the disadvantages of the current categorization methods (G-Fujioka, G-Elwany, G-Wang, and G-Kurien), and their unsuitability as screening tools, this study directed efforts to the creation of alternative screening methods of adenoid radiographic evaluation.
In order to do so, optimal cut-off points were originated for the remaining radiographic parameters, and accuracy rates were then calculated. With the exception of AA, AC/SP, and AO, the other quantitative parameters presented similar sensitivity rates; thus, it was not possible to isolate a single parameter with significant superiority over the others. However, Model #1 presented relatively higher negative predictive value, which means that the proportion of individuals with a negative test result who actually have less than 66.67% adenoid obstruction is relatively higher when such tool is used. Such feature (high negative predictive value) is also desirable for screening purposes, since clinicians and pediatricians must avoid neglecting, as much as possible, ill patients who would rather be referred to secondary care.
Alternatively, the choice of calculating specificity rates for 75.00% choanal obstruction was motivated by the desire to select a safe parameter intended to suggest patients to be benefited from adenoidectomy, i.e. to identify, with as much certainty as possible, individuals to be surgically23 treated. However, if a test tends to present higher specificity rates, more negative test results are obtained; and, as a consequence, several adenoidectomy candidates might be erroneously categorized as healthy.30 Yet, high specificity is still desirable when it comes to the indication of radical therapies, since the consequence of a false-positive test result (unnecessary adenoidectomy), may be mostly avoided rather than the consequences of false-negative test result.
The categorical assessment tools G-Fujioka and G-Elwany presented relatively higher specificity rates when compared to the remaining radiographic parameters. In addition, both parameters presented similar and relatively higher positive predictive values, which means that the proportion of individuals with a positive test result who actually have at least 75.00% adenoid obstruction is relatively higher when such tools are used. High positive predictive value is also desirable when selecting adenoidectomy candidates, since clinicians and pediatricians must avoid suggesting, as much as possible, adenoidectomy to healthy patients who would rather be clinically treated or not treated at all.
Wormald and Prescott12 have already reported high specificity and positive predictive value for G-Fujioka, considering 60.00% choanal obstruction. Amongst G-Fujioka and G-Elwany, however, the authors recommend the latter, since more individuals may be labeled as positive (21/120) by G-Elwany than by G-Fujioka (9/120). Therefore, even though both tools are satisfactorily specific, and present similarly high negative predictive values, G-Elwany might be considered even more useful than G-Fujioka, because more patients would have the opportunity to be properly (surgically)23 treated when assessed with G-Elwany.
However, the results and inferences here suggested must be cautiously analyzed. The thresholds that were assumed to represent ill children (MCO ≥ 66.67%), or patients who would benefit from adenoidectomy (MCO ≥ 75.00%) are merely theoretical.22,23 Hence, longitudinal studies are still required to confirm the efficiency of the methods suggested here for each of their respective purposes; whether for identification of pathologically obstructive patients (Model #1), or candidates to adenoidectomy (G-Elwany), either as a single or associated with other exams or clinical signs.
According to the analysis provided by this research, the authors conclude that Model #1 is potentially useful as a screening tool to identify patients with 66.67% adenoid obstruction. Also, G-Elwany was demonstrated to be a potentially safe assessment tool to rule out complaining patients with less than 75.00% obstruction.
FundingThis research was financially supported by the São Paulo Research Foundation (Fundação de Amparo à Pesquisa do Estado de São Paulo - FAPESP), under the process number 08/53538-0.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Feres MF, Hermann JS, Sallum AC, Pignatari SS. Radiographic adenoid evaluation – suggestion of referral parameters. J Pediatr (Rio J). 2014;90:279–85.





