

To identify the prevalence and factors associated with anemia in children attending Municipal Early Childhood Education Day Care Center (Centros Municipais de Educação Infantil [CMEI]) nurseries in Colombo-PR.
MethodsAnalytical, cross-sectional study with a representative sample of 334 children obtained by stratified cluster sampling, with random selection of 26 nurseries. Data collection was conducted through interviews with parents, assessment of iron intake by direct food weighing, and hemoglobin measurement using the finger-stick test. Bivariate association tests were performed followed by multiple logistic regression adjustment.
ResultsThe prevalence of anemia was 34.7%. Factors associated with anemia were: maternal age younger than 28 years old (p=0.03), male children (p=0.02), children younger than 24 months (p=0.01), and children who did not consume iron food sources (meat+beans+dark green leafy vegetables) (p=0.02). There was no association between anemia and iron food intake in CMEI. However, iron intake was well below the recommended levels according to the National Education Development Fund resolution, higher prevalence of anemia was observed in children whose intake of iron, heme iron, and nonheme iron was below the median.
ConclusionsIn terms of public health, the prevalence of anemia is characterized as a moderate problem in the studied population and demonstrates the need for coordination of interdisciplinary actions for its reduction in CMEI nurseries.
Identificar a prevalência e os fatores associados à anemia em crianças que frequentam berçários de Centros Municipais de Educação Infantil (CMEI) de Colombo-PR.
MétodosEstudo analítico, de caráter transversal, com amostra representativa de 334 crianças obtida por amostragem estratificada por conglomerados, com seleção aleatória de 26 berçários. A coleta de dados foi realizada por meio de entrevista com os pais, avaliação da ingestão de ferro por pesagem direta de alimentos e dosagem de hemoglobina por punção digital. Foram realizados testes de associação bivariados seguido pelo ajuste de uma regressão logística múltipla.
ResultadosA prevalência de anemia foi de 34,7%. Os fatores associados à anemia foram: idade materna inferior a 28 anos (p = 0,03), crianças do sexo masculino (p = 0,02), com idade inferior a 24 meses (p = 0,01) e que não consumiam fontes alimentares de ferro (carne+feijão+verduras verdes escuras) (p = 0,02). Não houve associação entre anemia e ingestão de ferro no CMEI. Porém, a ingestão de ferro foi bem abaixo do que recomenda a resolução do Fundo Nacional de Desenvolvimento da Educação, sendo possível observar maior prevalência de anemia nas crianças cuja ingestão de ferro, ferro heme e ferro não-heme apresentava-se abaixo da mediana.
ConclusãoEm termos de saúde pública, a prevalência de anemia encontrada se caracteriza como um problema moderado na população estudada e demonstra a necessidade de articulação de ações interdisciplinares para a sua diminuição nos CMEIs.
Anemia is a global public health problem, with important consequences for human health and the social and economic development of each nation.1 It results from single or multiple causes that act simultaneously, influencing children's health,2 their cognitive and physical development, and immunity, increasing the risk of infections and infant mortality.3
A global analysis of the prevalence of anemia worldwide has shown that preschool-age children are the most affected age range, with a prevalence rate of 47.4%.1
Due to its complex and difficult-to-control characteristics, several studies have sought to identify the reasons for its high prevalence and potential associated factors.4,5,6 The identification of these factors contributes to implementation of actions aimed at the prevention and minimization of the problem.
The period between conception and 2 years of age is a critical stage of development, making children vulnerable to anemia. At this age, they start attending Early Childhood Education Day Care Center nurseries, which are responsible for their full-time health and nutrition care.
The municipality of Colombo and the metropolitan region of Curitiba lack studies on the prevalence of anemia in children attending Municipal Early Childhood Education Day Care Centers (Centros Municipais de Educação Infantil [CMEI]). Thus, such studies are justified due to the greater vulnerability of these children and the identification of amounts of iron supplied in the meals at these institutions. Obtaining a profile of anemia status may contribute to the implementation and consolidation of actions that will contribute to its prevention and reduction in this population.
The objective of the study was to estimate the prevalence of anemia and to identify associated factors in children attending CMEI nurseries in the municipality of Colombo, state of Parana, Brazil.
Material and methodsThis is a cross-sectional analytical study of 334 children aged 6–36 months, attending CMEI nurseries the city of Colombo – PR, in the metropolitan region of Curitiba. Colombo has 38 CMEIs, attended by 6852 children regularly enrolled in 2012, with 816 in the nurseries.
The selected sample was representative of children from CMEI nurseries and was defined by stratified cluster sampling with a single step, with random selection of 26 of the 38 CMEIs in Colombo. These were separated by city health district according to their location, while respecting the proportion of students enrolled in each health district. As a reference to calculate the sample, a prevalence of anemia of 29.7% was adopted from a study carried out in CMEI nurseries of Cascavel, state of Parana, with a representative sample of children between 6 and 24 months,7 as the children are of the same age and also attend CMEIs. A confidence level of 95% was used, with a margin of error of 0.04 and an estimated proportion used as reference of 0.3. Because stratified cluster sampling was used, a 1.4 effect factor of sample design was included to guarantee the desired accuracy, resulting in a minimum sample of 320 children.
The questionnaire included questions about the socioeconomic, environmental, biological, maternal and birth characteristics, feeding practices, and iron supplementation. The questionnaires were previously tested in a pilot study in a CMEI that was not part of the sample. Interviews were conducted with parents and guardians from June to December 2013.
Hemoglobin levels were measured in a blood sample obtained by digital puncture, collected in a microcuvette, and reading was performed in portable hemoglobin meter. A hemoglobin concentration below 11g/dL was considered anemia and classified as mild (10.0–10.9g/dL), moderate (7.0–9.9g/dL), or severe (<7.0g/dL), according to the World Health Organization (WHO) criteria.8
The anthropometric assessment was performed with weight and height measurement. Weight was measured using a digital pediatric scale with 5g accuracy and 15kg capacity. Children were weighed naked using a clean disposable diaper, after the scale was previously calibrated and installed on a flat, smooth, firm surface. Children weighing more than 15kg were weighed on a portable digital scale with capacity of 150kg and 100g accuracy.9
The length was measured using a portable wooden anthropometer, with amplitude of 100cm and 0.5cm subdivisions. Children younger than 2 years were measured in the supine position on the anthropometer. Children older than 2 years were measured in the standing position with a wooden anthropometer.
The nutritional status was classified using the World Health Organization (WHO) Anthro program, version 3.2.2 (WHO, GE, Switzerland) for weight/age (W/A), height/age (H/A), and body mass index/age (BMI/A).10
Iron intake was obtained by individual direct weighing of the food provided at the CMEI, carried out on two nonconsecutive days. The nutritional composition of the food was obtained using the AVANUTRI® program (AVANUTRI®, RJ, Brazil). Iron intake was expressed as dietary intake of total iron, heme iron, and nonheme iron. Heme iron was considered as 40% of the iron contained in meat, and non-heme iron as the remaining 60%, added to the total iron found in other foods. The densities of total iron, heme iron, and nonheme iron were obtained by dividing the total of each of these nutrient by the total calories ingested by the child on the day, expressed in mg of iron per 1000kcal of the diet.11
The independent variables were distributed as follows: (1) biological factors: gender and age of the child; (2) feeding practice: duration of maternal breastfeeding, exclusive breastfeeding until six months, consumption of fruit juice, fruit, milk, beans, meat, liver, legumes, dark green leafy vegetables, iron-rich foods (meat+beans+dark green leafy vegetables); total iron, heme iron, and non-heme iron intake at CMEI; density of total iron, heme iron, and non-heme iron; (3) morbidities: fever and diarrhea in the last 15 days, history of anemia; (4) nutritional status: low birth weight, underweight, overweight, short stature, overweight according to BMI for age; (5) health care: prenatal care, number of prenatal consultations, iron supplementation during pregnancy, type of delivery, prematurity; (6) maternal factors: age, ethnicity, number of children; (7) socioeconomic factors: maternal level of education and employment, per capita income, welfare program beneficiaries and Children's Milk Program; home ownership, number of residents in the household, number of rooms, clean water, sewage treatment and garbage collection services.
The variables were categorized according to studies investigating anemia in children.2,4,11,12 Iron intake was categorized in relation to the observed mean values.
Data were entered in duplicate into a Google Drive® online form and after verification, they were exported to SPSS software, version 19.0 (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, NY: USA).
A descriptive analysis of the variables was performed. The association with anemia was verified using Fisher's exact test and the chi-squared test. The variables with p<0.20 were selected to compose the multiple logistic regression model. The multivariate analysis was performed by constructing the conceptual model based on and adapted from Osório et al.13
Seven hierarchical levels were defined according to the following order: maternal characteristics (age); nutritional status (short stature), morbidity (presence of fever and/or diarrhea in the previous 15 days, history of anemia); maternal breastfeeding (breastfeeding duration), feeding practices at home (consumption of dark green leafy vegetables, meats, liver and iron-rich foods (meat+beans+dark green leafy vegetables); iron intake at CMEI (non-heme iron and total iron); biological characteristics of the child (gender and age). The variables were entered into the model one by one, and those that did not show statistical significance of p<0.05 were removed. Crude and adjusted odds ratios (OR) were estimated.
This work is part of the Research Project on Food and Nutrition Security in the School Environment, approved by the Ethics Committee for Research in Human Beings (CAAE 11312612.5.0000.0102).
ResultsThe estimated prevalence of anemia is 34.7%. Of the anemic children, 56.9% had mild, 42.2% moderate, and 0.9% severe anemia. The mean hemoglobin level was 11.3g/dL (±1.34).
The mean age of the children was 21.2 (±5.7) months and 50.3% were males. The median duration of breastfeeding was 180 days and of exclusive breastfeeding, 90 days. This study found 5% short stature, 0.6% underweight, 3.4% overweight, and 8.4% overweight according to BMI. Family income per capita was less than one minimum wage in 76.7% of households.
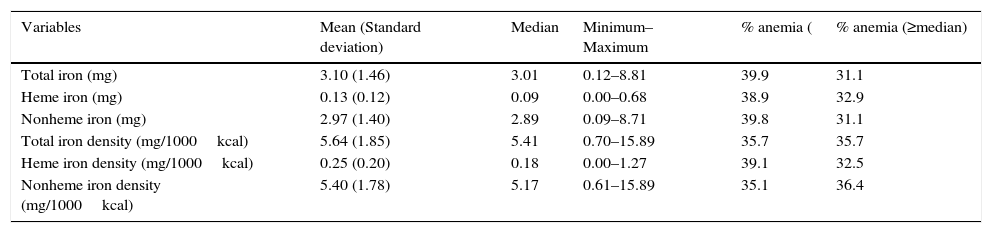
The median intake of total iron at the CMEI was 3.01mg, with a larger contribution of non-heme iron. The median iron density was 5.64mg/1000kcal. The prevalence of anemia was higher in children that had total iron, heme iron, nonheme iron intake, and heme iron density below the median levels (Table 1).
Total iron, heme iron, and nonheme iron intake, in addition to total iron, heme iron, and nonheme iron density in the diet of children attending Municipal Early Childhood Education Centers, Colombo, 2013.
| Variables | Mean (Standard deviation) | Median | Minimum–Maximum | % anemia ( | % anemia (≥median) |
|---|---|---|---|---|---|
| Total iron (mg) | 3.10 (1.46) | 3.01 | 0.12–8.81 | 39.9 | 31.1 |
| Heme iron (mg) | 0.13 (0.12) | 0.09 | 0.00–0.68 | 38.9 | 32.9 |
| Nonheme iron (mg) | 2.97 (1.40) | 2.89 | 0.09–8.71 | 39.8 | 31.1 |
| Total iron density (mg/1000kcal) | 5.64 (1.85) | 5.41 | 0.70–15.89 | 35.7 | 35.7 |
| Heme iron density (mg/1000kcal) | 0.25 (0.20) | 0.18 | 0.00–1.27 | 39.1 | 32.5 |
| Nonheme iron density (mg/1000kcal) | 5.40 (1.78) | 5.17 | 0.61–15.89 | 35.1 | 36.4 |
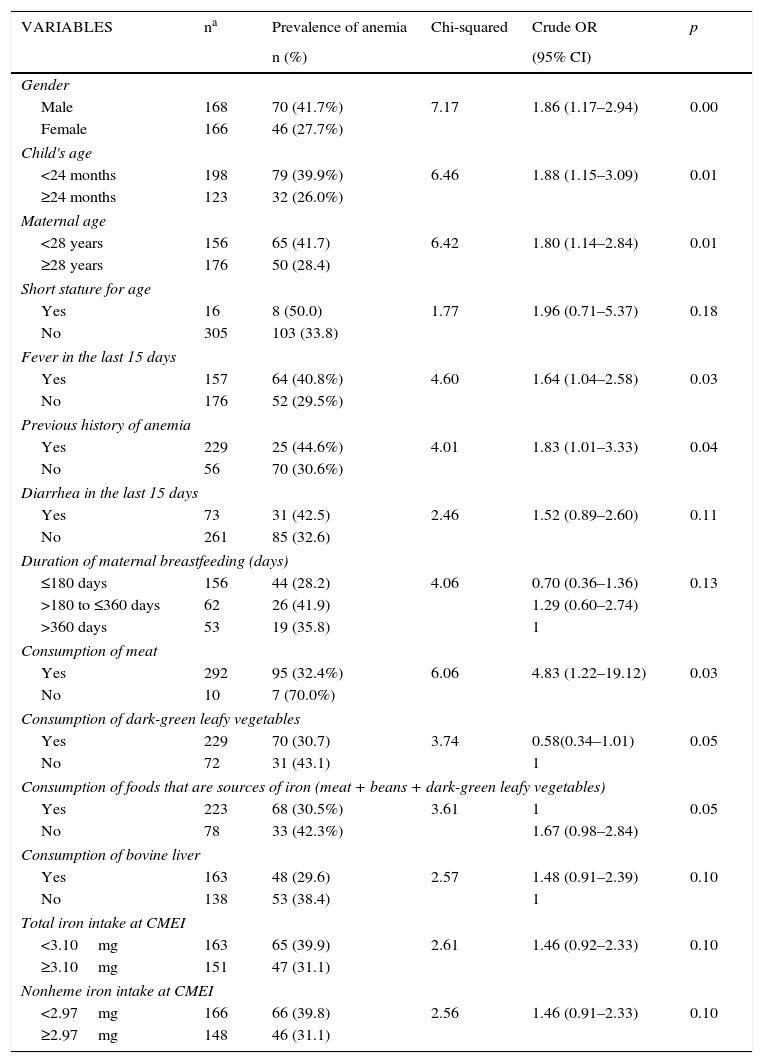
In the bivariate analysis (Table 2), anemia showed a statistical association with male gender (OR: 1.86; 95% CI: 1.17–2.94); age younger than 24 months (OR: 1.88; 95% CI: 1.15–3.09); maternal age younger than 28 years (OR: 1.80; 95% CI: 1.14–2.84) and non-consumption of iron food sources (OR: 1.67; 95% CI: 0.98–2.84). Other significant factors in this first stage of the analysis were: presence of fever in the previous 15 days (OR: 1.64; 95% CI: 1.04–2.58), previous history of anemia (OR: 1.83; 95% CI: 1.01–3.33), meat consumption (OR: 4.83; 95% CI: 1.22–19.12) and consumption of dark green leafy vegetables (OR: 0.58; 95% CI: 0.34–1.01). Fourteen factors showed p<0.20 in the bivariate analysis and were considered for inclusion in the multiple logistic regression model (Table 2).
Distribution of anemia in children from Municipal Early Childhood Education Centers, Colombo, 2013.
| VARIABLES | na | Prevalence of anemia | Chi-squared | Crude OR | p |
|---|---|---|---|---|---|
| n (%) | (95% CI) | ||||
| Gender | |||||
| Male | 168 | 70 (41.7%) | 7.17 | 1.86 (1.17–2.94) | 0.00 |
| Female | 166 | 46 (27.7%) | |||
| Child's age | |||||
| <24 months | 198 | 79 (39.9%) | 6.46 | 1.88 (1.15–3.09) | 0.01 |
| ≥24 months | 123 | 32 (26.0%) | |||
| Maternal age | |||||
| <28 years | 156 | 65 (41.7) | 6.42 | 1.80 (1.14–2.84) | 0.01 |
| ≥28 years | 176 | 50 (28.4) | |||
| Short stature for age | |||||
| Yes | 16 | 8 (50.0) | 1.77 | 1.96 (0.71–5.37) | 0.18 |
| No | 305 | 103 (33.8) | |||
| Fever in the last 15 days | |||||
| Yes | 157 | 64 (40.8%) | 4.60 | 1.64 (1.04–2.58) | 0.03 |
| No | 176 | 52 (29.5%) | |||
| Previous history of anemia | |||||
| Yes | 229 | 25 (44.6%) | 4.01 | 1.83 (1.01–3.33) | 0.04 |
| No | 56 | 70 (30.6%) | |||
| Diarrhea in the last 15 days | |||||
| Yes | 73 | 31 (42.5) | 2.46 | 1.52 (0.89–2.60) | 0.11 |
| No | 261 | 85 (32.6) | |||
| Duration of maternal breastfeeding (days) | |||||
| ≤180 days | 156 | 44 (28.2) | 4.06 | 0.70 (0.36–1.36) | 0.13 |
| >180 to ≤360 days | 62 | 26 (41.9) | 1.29 (0.60–2.74) | ||
| >360 days | 53 | 19 (35.8) | 1 | ||
| Consumption of meat | |||||
| Yes | 292 | 95 (32.4%) | 6.06 | 4.83 (1.22–19.12) | 0.03 |
| No | 10 | 7 (70.0%) | |||
| Consumption of dark-green leafy vegetables | |||||
| Yes | 229 | 70 (30.7) | 3.74 | 0.58(0.34–1.01) | 0.05 |
| No | 72 | 31 (43.1) | 1 | ||
| Consumption of foods that are sources of iron (meat + beans + dark-green leafy vegetables) | |||||
| Yes | 223 | 68 (30.5%) | 3.61 | 1 | 0.05 |
| No | 78 | 33 (42.3%) | 1.67 (0.98–2.84) | ||
| Consumption of bovine liver | |||||
| Yes | 163 | 48 (29.6) | 2.57 | 1.48 (0.91–2.39) | 0.10 |
| No | 138 | 53 (38.4) | 1 | ||
| Total iron intake at CMEI | |||||
| <3.10mg | 163 | 65 (39.9) | 2.61 | 1.46 (0.92–2.33) | 0.10 |
| ≥3.10mg | 151 | 47 (31.1) | |||
| Nonheme iron intake at CMEI | |||||
| <2.97mg | 166 | 66 (39.8) | 2.56 | 1.46 (0.91–2.33) | 0.10 |
| ≥2.97mg | 148 | 46 (31.1) | |||
The entry order of the variables into the multiple logistic regression model is shown in Fig. 1.

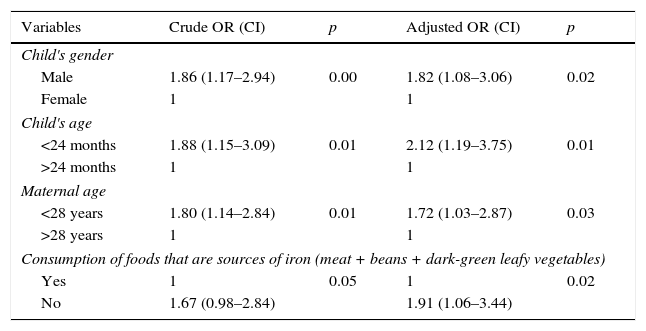
Table 3 shows the result of the multiple logistic regression model adjustment. After running the selection algorithm, the following variables remained in the model: child's gender, estimating an 82% higher chance of anemia in male children (OR: 1.82; 95% CI: 1.08–3.06); child's age younger than 24 months (OR: 2.12; 95% CI: 1.19–3.75); maternal age younger than 28 years (OR: 1.72; 95% CI: 1.03–2.87), and non-consumption of iron food sources (OR: 1.91; 95% CI: 1.06–3.44).
Logistic regression model for factors associated with anemia in children from Municipal Early Childhood Education Centers, Colombo, 2013.
| Variables | Crude OR (CI) | p | Adjusted OR (CI) | p |
|---|---|---|---|---|
| Child's gender | ||||
| Male | 1.86 (1.17–2.94) | 0.00 | 1.82 (1.08–3.06) | 0.02 |
| Female | 1 | 1 | ||
| Child's age | ||||
| <24 months | 1.88 (1.15–3.09) | 0.01 | 2.12 (1.19–3.75) | 0.01 |
| >24 months | 1 | 1 | ||
| Maternal age | ||||
| <28 years | 1.80 (1.14–2.84) | 0.01 | 1.72 (1.03–2.87) | 0.03 |
| >28 years | 1 | 1 | ||
| Consumption of foods that are sources of iron (meat + beans + dark-green leafy vegetables) | ||||
| Yes | 1 | 0.05 | 1 | 0.02 |
| No | 1.67 (0.98–2.84) | 1.91 (1.06–3.44) | ||
A 34.7% prevalence of anemia was identified, as well as a positive association with younger maternal age, male gender, child's age younger than 24 months, and non-consumption of iron-rich foods (beans, meat, and dark green leafy vegetables) at home.
In public health, the prevalence of anemia of 34.7% is considered a moderate problem in the studied population.3 This prevalence is higher to that found in a study carried out in Cascavel – PR,7 which investigated children younger than 24 months that attended daycare (29.7%). The Woman and Child National Demographic and Health Survey (Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher [PNDS]) of 2006 assessed the prevalence of anemia in children at the national level, for the first time and found a prevalence rate of 20.9% in children younger than 59 months, and 35.8% in children younger than 24 months, close to what was found in this study.14
This result is consistent with that of Leal et al.12 (32.8%) in children aged 0–59 months from the state of Pernambuco and Castro et al.15 (29.2%) in preschoolers, and lower than that identified in Vitória (ES) (15.7%) in children aged 1–5 years.16 Two other studies investigating anemia in day care center nurseries found higher prevalence rates, 51.9% and 46.6%.2,17 A meta-analysis performed by Vieira & Ferreira found a higher weighted mean prevalence than that found in the present study: 52% anemia in day care centers, 60.2% in health services, and 66.5% in disadvantaged populations.18
Although most children have mild anemia, moderate anemia was found in 42.2% of the anemic children; such rate deserves attention, as anemia negatively affects cognitive development, physical capacity, production of thyroid hormones, body temperature regulation, and immune status, increasing the risk of infection and causing effects that last for a lifetime.14 Konstantyner et al.4 found 9.9% moderate anemia in children younger than 24 months from all regions of Brazil.
The association between anemia and age younger than 24 months has been verified in studies conducted in day care centers.15,19,20 This vulnerability is related to an increased growth velocity, wherein the weight triples and body surface area doubles. This fact generates increased nutritional needs, which coincides with major changes in feeding, introduction of complementary feeding, weaning, and exposure to the family feeding practices.
Early cessation of breastfeeding associated to a poor complementary diet with low iron content adds a multiplier effect to the anemia risk increase. This risk is aggravated by the greater exposure to contagion from infectious and parasitic diseases, due to increased contact with the outside environment.11,15,20 Only 13.2% of children were breastfed exclusively for 6 months, 33% had meat introduced at 6 months of age, and the iron intake, especially heme iron, was well below the intake observed in older children and corresponded to 35.2% of what is recommended by the National School Feeding Program.
Brain growth is higher in the first two years of life, when the central nervous system membranes are more permeable to iron, representing the most critical time for its use. Iron deficiency has consequences such as the loss of physical and cognitive development, which impairs learning ability and decreases work capacity. Promoting better nutrition in the first 1000 days of life has been one of the strategies to improve the health status in adulthood, as well as human development, and reinforces the importance of prevention of nutritional deficiencies, such as iron deficiency anemia in first two years of life.21
The higher prevalence of anemia in males is related to the higher growth rate in boys, resulting in greater need for iron by the body, not supplied by the diet.15,22,23
Maternal age and non-consumption of iron-rich foods remained in the final model and are related to family questions associated to the home. This situation demonstrates the homogeneity in relation to the other assessed variables and emphasizes the importance of this study to identify subgroups that are the most vulnerable to the development of anemia, within a relatively homogeneous population.
Older mothers are better able to meet the health care demands of their children. The risk of anemia in children of younger mothers suggests that these are less prepared to meet the nutritional needs of their children and to perform the duties of motherhood. This may reflect the lack of financial resources, lack of knowledge about anemia and child care, and lack of adequate guidance.11,12,20,24
The non-consumption of iron food sources remain associated with anemia and emphasizes the importance of adequate nutrition in the family context, containing beans, dark green leafy vegetables, and especially meat and viscera, as they are sources of heme iron, with better bioavailability. Children whose parents reported consumption of these foods at home were more protected against anemia.
The iron intake at the CMEI showed no association with anemia. However, there is a higher prevalence of anemia in children that showed intake of total iron, heme iron, nonheme iron, and heme iron density below the median. This association probably does not occur because at the CMEI, as all children basically receive the same diet.
The National School Feeding Program (Programa Nacional de Alimentação Escolar, PNAE) recommends that the food served at school should include 7.7mg/day of iron for children aged 7–11 months and 4.9mg/day for children aged 1–3 years.25 The median intake of iron found in the CMEI (3.10mg) is well below this recommendation. A study of children aged 6–59 months in the state of Pernambuco found a significant linear trend with a reduction in anemia prevalence with the increase in the density of total iron, heme iron, and nonheme iron in the children's diet.11 The low amount of iron consumed in the CMEI, together with the low supply of iron food sources, reflects the difficulty of implementing the PNAE recommendations and shows that school feeding has not been sufficient to contribute to the prevention of anemia in the children attending these schools.
No variable related to socioeconomic and environmental conditions showed an association with anemia, probably due to sample homogeneity. This is evident when considering that almost 80% of the population lives on less than one minimum wage per capita, 84.8% of households have basic sanitation facilities, 98.7% have access to clean water, and 100% have public garbage collection services. Other studies conducted in daycare centers found no correlation with family income.26–28
This study attempted to assess all conditions that might be related to anemia described in the scientific literature, but the scope of this study was to investigate iron intake variables, which are seldom investigated in most studies due to the difficulty in obtaining such data.
As limitations of the study, the fact that it is cross-sectional should be mentioned, which makes it impossible to understand the cause and effect association of anemia. Moreover, iron intake at home was not quantified. However, considering that the children spent the whole day at the CMEI and had most of their meals there allows for the assumption that the participation of the food received at school is predominant in these children's lives. The authors interviewed the mothers to investigate the children's feeding practices regarding the consumption of iron-rich foods at home.
Anemia, a result of food insecurity present in the children's lives, reflects the violation of the right to regular and permanent access to quality food in sufficient quantity. The CMEI must promote food and nutrition security, with strategies that permeate health care and adequate food intake, because anemia affected more than 1/3 of the children, who showed low food contribution of iron.
The CMEI are potential sites for the carrying out of interventions, considering the children remain there full-time. Interdisciplinary actions – the roles of health and education professionals together with families – can be the foundation that will support better health for the children. The planning of strategies and training of involved professionals for better food iron supply in CMEI are encouraged.
Factors associated with anemia are also a result of the influence of social, economic, and behavioral conditions of the population that reflect on the health and nutrition of these individuals. Every action that benefits the children's health also depends on economic, political, and social restructuring of the country, which can stimulate advances that will affect education, employment, income, and access to health care. The strengthening and investing in such strategies and programs to promote the families’ household food security will indirectly prevent anemia.
FundingThe research is part of the PROCAD/Casadinho UFPR-UFPE project of Conselho Nacional de Desenvolvimento Cientifico e Tecnológico (CNPq), process No. 552448/2011-7. Capes Fellow.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Zuffo CR, Osório MM, Taconeli CA, Schmidt ST, da Silva BH, Almeida CC. Prevalence and risk factors of anemia in children. J Pediatr (Rio J). 2016;92:353–60.
The article is part of the first author's Master's Degree dissertation in Postgraduate Program in Food and Nutrition Security, Department of Health Sciences, Universidade Federal do Paraná, Curitiba, PR, Brazil.




