
To collect the most up-to-date information regarding pediatric osteoarticular infections, including the epidemiological and microbiological profiles, diagnosis, and treatment.
Source of dataA non-systematic review was performed on the search engines PubMed, SciELO, LILACS, and Google Scholar, using the keywords “bone and joint infection”, “children”, “pediatric”, “osteomyelitis”, “septic arthritis” and “spondylodiscitis” over the last ten years. The most relevant articles were selected by the authors to constitute the database.
Synthesis of dataOsteoarticular infections are still a major cause of morbidity in pediatrics. Their main etiology is Staphylococcus aureus, but there has been an increase in the detection of Kingella kingae, especially through molecular methods. Microbiological identification allows treatment direction, while evidence of inflammatory activity assists in treatment follow-up. Imaging tests are especially useful in the initial diagnosis of infections. Empirical treatment should include coverage for the main microorganisms according to the age and clinical conditions of the patient, while considering the local resistance profile. Surgical procedures can be indicated for diagnosis, focus control, and function preservation. Acute complications include sepsis, deep venous thrombosis, and pulmonary embolism. Deaths are rare. Late complications are uncommon but may lead to deformities that compromise motor development.
ConclusionA correct and early diagnosis, prompt implementation of adequate antimicrobial therapy, and focus control, when indicated, are critical to a better prognosis.
Compilar as informações mais atuais referentes às infecções ostoarticulares em pediatria, inclusive perfil epidemiológico e microbiológico, diagnóstico e tratamento.
Fonte dos dadosFeita revisão não sistemática nos mecanismos de busca Pubmed, Scielo, Lilacs e Google Scholar, com as palavras-chave bone and joint infection, children, pediatric, osteomyelitis, septic arthritis e espondylodiscitis nos últimos 10 anos. Os artigos mais relevantes foram selecionados pelos autores para compor a base de dados.
Síntese dos dadosAs infecções osteoarticulares ainda são causa importante de morbidade na pediatria. A sua principal etiologia é o Staphylococcus aureus, porém há um aumento na detecção de Kingella kingae, especialmente através de métodos moleculares. A identificação microbiológica possibilita direcionamento de tratamento, enquanto que as provas de atividade inflamatória auxiliam no acompanhamento do tratamento. Exames de imagem são especialmente úteis no diagnóstico inicial das infecções. O tratamento empírico deve incluir cobertura para os principais microrganismos, de acordo com a faixa etária e as condições clínicas do paciente, considerando o perfil de resistência local. Procedimentos cirúrgicos podem ser indicados para diagnóstico, controle do foco e preservação da função. As complicações agudas incluem sepse, trombose venosa profunda e embolia pulmonar. Óbitos são raros. As complicações tardias são incomuns, mas podem levar a deformidades que comprometem o desenvolvimento motor.
ConclusãoO diagnóstico correto e precoce, com pronta instituição de terapia antimicrobiana adequada e controle do foco, quando indicado, é fundamental para um melhor prognóstico.
Osteoarticular infections (OAI) in children and adolescents remain an important cause of morbidity and may cause deformities that compromise motor development.1 For this reason, and considering the difficulty of early and adequate diagnosis, it is an extremely important issue in pediatric clinical practice.
The focus of this article is acute OAI of bacterial etiology and, for this reason, the following infections will be included in the review:
- "02"
Septic arthritis: an intra-articular infectious process;
- "02"
Osteomyelitis: a bone infectious process;
- "02"
Spondylodiscitis: encompasses the infectious processes of intervertebral discs.
It is noteworthy that osteomyelitis can spread contiguously and reach adjacent joints, leading to a picture of associated osteomyelitis and septic arthritis.2
A specific type of OAI that will not be addressed in this article is vertebral osteomyelitis, as it has distinct epidemiological and microbiological characteristics from other infections. Its most common etiology is Mycobacterium tuberculosis and its treatment is directed at this agent.2
EpidemiologyOsteoarticular infections are more common in children under 5 years of age and in males.2–4 Overall, they affect previously healthy patients, but some conditions may predispose to its occurrence, such as immunosuppression, prematurity, and sickle-cell anemia.5
Approximately 20% of patients have some history of nonspecific local trauma in the two weeks prior to diagnosis, such as falls, bruises, and abrasions; however, as trauma is very common in this age group, it is possible that reports by parents and/or guardians are underestimated.6
In developed countries, it is estimated that the incidence of osteomyelitis ranges from two to 13 cases per 100,000 inhabitants. In developing countries, the incidence tends to be higher, reaching 200 cases per 100,000 inhabitants.7
Septic arthritis is less common, with an incidence ranging from one to five cases per 100,000 inhabitants in developed countries8–10 to 20 cases per 100,000 inhabitants in developing countries.11
There are no specific data from Brazil on the incidence of osteoarticular infections.
EtiologyMost of these infections occur due to hematogenous spread during episodes of transient bacteremia in patients who may have been asymptomatic until then.2 In case of osteomyelitis, the infection usually begins in the highly vascularized metaphyseal region and may spread to other regions, including adjacent joints.2
A lower percentage of infections may occur by contiguity or direct inoculation, in post-trauma situations, or even after surgical procedures.5
The main etiological agent of osteoarticular infections is Staphylococcus aureus, a Gram-positive coccus that usually colonizes the airways and skin.2,5 The increased prevalence of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) is currently the subject of important discussions, leading to the need to re-evaluate several protocols for the treatment of infections caused by this agent.12,13 In Latin America, some countries have already shown a higher incidence rate of OAI caused by CA-MRSA, such as Uruguay, Argentina, and Chile.14–16 However, a study carried out in French Guiana between 2010 and 2015did not find CA-MRSA in the assessed population.17 In Brazil, two studies conducted in the state of São Paulo showed methicillin-resistance rates of 20%–45% in pediatric OAI.18,19 Additionally, the detection of toxin-producing strains, such as those that produce Panton–Valentine leukocidin, which can lead to more severe cases with sepsis, shock, and even death, are also a matter of concern. For this reason, knowledge of the local resistance profile of this microorganism is extremely important for determining the best empirical antibiotic therapy regimen for OAI.2,5
Another microorganism that has been increasingly identified, especially in the age group under 36 months in developed countries, is Kingella kingae, a Gram-negative coccobacillus that is difficult to grow in standard culture media.2 It is identified especially through molecular diagnostic methods and it is estimated that this microorganism may be responsible for most cases of OAI with negative cultures.2 A study performed between 2004 and 2005 in France showed that Kingella kingae was responsible for 45% of cases of OAI in children, being more frequent than Staphylococcus aureus, responsible for only 29% of cases.20 Infections caused by Kingella kingae have shown to be milder, with fewer laboratory alterations and less systemic involvement.21,22 In Brazil, there are no studies on the role of this microorganism in OAI in children. It is a rarely identified agent, since molecular tests are not common in routine clinical practice.
Other agents that can cause pediatric osteoarticular infections include the following:2,5
- •
Group A Streptococcus;
- •
Streptococcus pneumoniae;
- •
Group B Streptococcus, which is more common in neonates;
- •
Enterobacteria, such as E. coli, also more common in neonates, and Salmonella spp.is more common in patients with sickle-cell anemia;
- •
Pseudomonas aeruginosa, especially in cases of osteomyelitis post-plantar perforating injury;
- •
Neisseria gonorrhoeae, in cases of septic arthritis in the sexually active population.
It is important to remember that up to 60% of cases may remain without microbiological identification when evaluated exclusively by culture.3,16,20
Clinical pictureSeptic arthritisThe most common presentation of septic arthritis includes local pain, present in approximately 80% of the cases, which may be accompanied by edema, reduced mobility of the affected joint, and/or fever.1,7
In neonates and young infants, the main symptoms may be nonspecific, such as irritability and inappetence, whether or not associated with fever and/or refusal to move the affected joint.2
In general, the symptoms are acute, starting between two and four days, and the most commonly affected joints are the knee and the hip, followed by the ankle, elbow, and shoulder. The clinical diagnosis of hip arthritis is especially challenging. The typical condition includes anterior hip and thigh pain that sometimes radiates to the knee, claudication, and decreased hip mobility, which assumes a preferred position of external rotation, flexion, and abduction.2,4,23,24
OsteomyelitisOsteomyelitis can be divided, based on the time of evolution, into acute (less than two weeks), subacute (between two weeks and three months), and chronic (more than three months).5
Its initial presentation includes local alterations such as pain, edema, and other phlogistic signs, as well as difficulty in moving the affected limb. A history of fever may be present in 60%–80% of the cases.1,2
Symptoms may be nonspecific in newborns and young infants, as in cases of septic arthritis.
The most frequently affected bones, in decreasing order, are the femur, tibia, and humerus.2,4 Involvement of the foot, hand, fibula, radius, and clavicle is less frequent.2,4
SpondylodiscitisSpondylodiscitis presentation is usually more insidious and nonspecific. Its main symptoms include low back pain, and refusal to bend the back, sit, stand, or walk.2,25 There may also be an association with abdominal pain and constipation.2,25 Fever may be absent and systemic symptoms are less common.2,25
The mean time between symptom onset and the final diagnosis is around 27 days, being more than four weeks in up to 70% of cases.25
Most cases show concomitant disc and vertebral involvement, with exclusive disc involvement being rare.25 The most affected region is the lumbar region (75% of cases), with the L4/L5 space being the most affected.25
DiagnosisThe diagnosis is based on clinical suspicion, considering the patient's history and physical examination, and with the help of laboratory and imaging tests.
Laboratory testsThe main recommended laboratory tests that can help in both the diagnosis and follow-up of cases are as follows: complete blood count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Tests for microbiological identification are also fundamental, such as blood culture and culture of other relevant sites (such as synovial fluid or deep tissue sample).2
Complete blood countThe complete blood count can show leukocytosis, but this alteration is not mandatory, being less common in neonates and young infants.1,2
Inflammatory activity testsThe inflammatory activity tests, ESR and CRP, are useful both in the diagnosis and in the evaluation of treatment response.1,2 Both are usually elevated at the onset, and CRP tends to normalize more quickly with appropriate treatment, indicating a good outcome.1,2 Another marker that may bring benefits in the diagnosis and follow-up of cases in the future is procalcitonin, but it is a test that is not routinely available in clinical practice, and it has not been shown to be considerably superior to joint analysis by ESR and CRP in these cases.2 It is important to emphasize, however, that these tests may show normal values and thus do not rule out the diagnosis of OAI.1,2
CulturesBlood culture should be collected whenever OAI is suspected, preferably before the onset of empirical antibiotic therapy, but without significantly delaying it.1,2,26
Microbiological tests (culture or molecular tests) from normally sterile sites, such as bone tissue or synovial fluid, can confirm the diagnosis of OAI, as well as provide important information regarding the resistance profile of the isolated microorganism.1,2,26 Inoculation of at least one material sample in a blood culture flask is recommended to increase the chances of identifying Kingella kingae.1,2 In case of bone material analysis, it is recommended to collect at least three samples, aiming to increase the chance of positivity.26
For patients with osteomyelitis secondary to implants or post-osteosynthesis, sonication of the collected material is recommended to increase positivity rates.26
It is important to emphasize that, in case of samples obtained surgically, the administration of prophylactic antibiotic therapy at the anesthetic induction is recommended, with the aim of avoiding bacteremia and sepsis secondary to surgical manipulation, and that there is no evidence of positivity rate reduction due to this prophylaxis.26
Although they are not routinely performed in clinical practice, molecular tests can be especially useful in identifying microorganisms that do not usually grow easily in standard culture media, such as Kingella kingae.18
Imaging testsPlain X-rayA plain X-ray is recommended for all cases of suspected OAI, especially to rule out other diagnostic hypotheses such as neoplasms or fractures, since its sensitivity for the definitive diagnosis of these infections is low.2
The alterations observed in osteomyelitis include bone thinning and periosteum elevation; they may take ten to 21 days to appear.2 In spondylodiscitis, a reduction in intervertebral space and erosion of the adjacent vertebra can be observed, but this type of alteration may take two to three weeks to appear.2 In case of septic arthritis, the main alterations observed include increased joint space and soft tissue edema.2
UltrasonographyUltrasonography is an easy-to-perform, non-invasive test, commonly available in pediatric clinical practice. It is indicated for the diagnosis of septic arthritis, with high sensitivity for the identification of joint effusion.2 In some cases, when performed by experienced operators, it may also allow the visualization of bone abscesses and periosteal alterations, but it is not the most indicated test for osteomyelitis diagnosis.27
Computed tomographyComputed tomography has lower sensitivity than magnetic resonance imaging, but it is more often available in clinical practice and easier to perform in the pediatric age group. For these reasons, it is often preferentially performed. In addition to assisting in the diagnosis of infections, it can also be useful in planning surgical procedures and guiding aspiration or drainage procedures.2
Magnetic resonance imagingMagnetic resonance imaging is the most appropriate test for the diagnosis of OAI, especially in cases of osteomyelitis and spondylodiscitis, due to its high sensitivity, and because it is able to detect alterations early, after only three to five days of evolution.2,26 However, it is difficult to perform, often requiring sedation in pediatric clinical practice, and is seldom available, which makes it difficult to routinely perform.
ScintigraphyScintigraphy is most useful in suspected multifocal involvement, or in cases where it is not possible to determine the exact site of infection through the anamnesis or clinical examination.2 It has high sensitivity, but low specificity, and both are lower in newborns and young infants.2 The main problem with this type of test is the high radiation doses required for its performance.2
TreatmentThe basis of OAI treatment includes antimicrobial therapy and control of infectious foci.2 Generally, hospitalization is recommended for the start of parenteral antibiotic therapy and close monitoring of the case evolution.
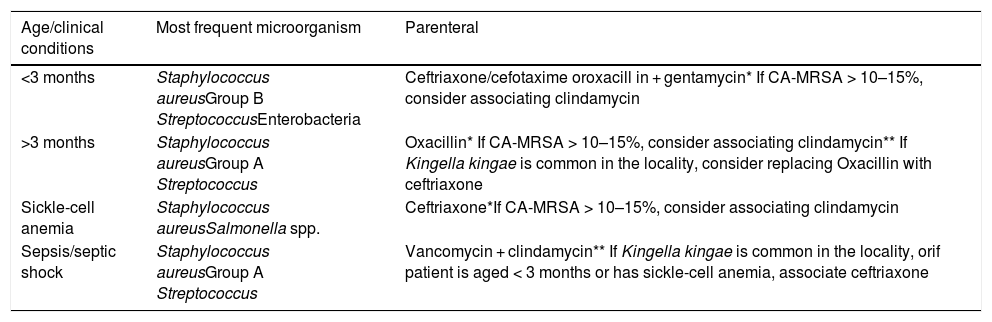
Antimicrobial therapyEmpirical antimicrobial therapy should provide coverage for the main etiological agent according to the type of injury, clinical conditions, and patient age range (Table 1).27,28
Suggested empirical treatment regimen based on patient age and clinical conditions.
| Age/clinical conditions | Most frequent microorganism | Parenteral |
|---|---|---|
| <3 months | Staphylococcus aureusGroup B StreptococcusEnterobacteria | Ceftriaxone/cefotaxime oroxacill in + gentamycin* If CA-MRSA > 10–15%, consider associating clindamycin |
| >3 months | Staphylococcus aureusGroup A Streptococcus | Oxacillin* If CA-MRSA > 10–15%, consider associating clindamycin** If Kingella kingae is common in the locality, consider replacing Oxacillin with ceftriaxone |
| Sickle-cell anemia | Staphylococcus aureusSalmonella spp. | Ceftriaxone*If CA-MRSA > 10–15%, consider associating clindamycin |
| Sepsis/septic shock | Staphylococcus aureusGroup A Streptococcus | Vancomycin + clindamycin** If Kingella kingae is common in the locality, orif patient is aged < 3 months or has sickle-cell anemia, associate ceftriaxone |
CA-MRSA, community-acquired methicillin-resistant Staphylococcus aureus.
It must necessarily include coverage for Staphylococcus aureus and, where there is a prevalence higher than 10–15% of CA-MRSA, this resistance profile should also be taken into consideration when choosing the preferred regimen.2
The regimen should always be selected once the microorganism is identified in culture or through molecular methods, based on the results of the resistance and sensitivity profile. In case of OAI with negative culture, the transition to oral antibiotic therapy should follow the coverage profile of the initial parenteral regimen.
The treatment should be administered parenterally until clinical and laboratory improvement is attained.2 Previously, treatment with at least two weeks of intravenous therapy was recommended, but recent studies have shown that shorter cycles with early transition to an oral antimicrobial regimen are equally effective.28–31 The transition can be performed early in uncomplicated cases, when the patient has been afebrile for at least 24–48 hours, and with falling CRP levels (30%–50% of its highest value).2
The duration of the antimicrobial regimen varies from two to three weeks in cases of septic arthritis, two to four weeks in cases of spondylodiscitis (this time is quite variable due to case heterogeneity), and from four to six weeks in cases of osteomyelitis.2,32 Complicated cases may require prolonged treatment.2
Surgical proceduresThe main indications for undergoing the surgical procedure include microbiological diagnosis (through aspiration of synovial fluid or bone biopsy), control of the infectious foci, and maximum preservation of the affected limb function.4
Septic arthritisJoint drainage and irrigation is recommended as soon as possible whenever an infectious process is suspected, and can be performed by arthrotomy, arthroscopy, or arthrocentesis, depending on the experience of the care team and the patient's clinical condition.2,4 This procedure is indicated for both the microbiological diagnosis and control of the infectious focus, and the collection of material for culture is always indicated.2,4,5
Although arthroscopy is associated with a shorter hospital length of stay, arthrotomy is still recommended in cases of hip and shoulder joint involvement in young infants aged <6 months, in case of infection by more virulent microorganisms such as Panton-Valentine leukocidin-producing Staphylococcus aureus, and in patients whose treatment had a late start (after five to seven days of evolution).2
OsteomyelitisStudies show that up to 90% of patients respond well to conservative treatment without the need for surgery, especially if the diagnosis is made early.2 For this reason, routine surgical procedures are not indicated in these cases.2,5 These procedures are reserved for cases where there is no adequate response to antimicrobial therapy within 72−96 hours, those with persistence of fever and elevated levels on inflammatory activity tests, and for aspiration or drainage of purulent collections and debridement of necrotic areas.2,4
Whenever a surgical procedure is performed, culture material should be collected, regardless of the antibiotic therapy duration.
ComplicationsPatients with osteoarticular infections may have initial complications secondary to bacteremia and late complications related to bone alterations due to infection. Complications are associated with cases of infection by more virulent microorganisms such as CA-MRSA, Panton–Valentine leukocidin-producing S. aureus, or Salmonella spp.2
Early complications include persistent bacteremia, usually secondary to an uncontrolled focus of infection, such as undrained abscesses; sepsis or septic shock; deep vein thrombosis (DVT), especially associated with infections caused by CA-MRSA and, consequently, pulmonary embolism.33 Studies have shown a rate of 6%–40% of DVT in patients with osteoarticular infection caused by CA-MRSA. For this reason, some authors recommend performing ultrasonography for DVT screening in these patients and, at the slightest evidence of respiratory distress, an urgent assessment for possible pulmonary embolism should be performed.33 However, there is no indication for routine DVT prophylaxis.2 In cases with this complication, prolonged antimicrobial treatment is recommended, and at least six weeks of intravenous therapy is suggested, followed by oral therapy until the thrombosis resolves.2 The initial treatment of DVT should be performed with low-molecular-weight heparin.2 Deaths secondary to osteoarticular infections are currently very rare.2
Nonetheless, late complications may include impairment of the growth plate of the affected bone, with subsequent difference in limb size; avascular necrosis of the femoral head; pathological fractures; loss of function; recurrent infections and chronic osteomyelitis.5 These complications, however, are rare.3,4
ConclusionOAIs are an important cause of morbidity in the pediatric age group and it is important to consider their diagnosis when appropriate. Their main etiological agent is Staphylococcus aureus, but they may also be caused by other microorganisms, which vary with the patient's age, location, and clinical conditions. An early diagnosis and start of antimicrobial treatment are crucial for good patient outcome, as well as the control of the infectious focus.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Alvares PA, Mimica MJ. Osteoarticular infections in pediatrics. J Pediatr (Rio J). 2020;96:58–64.





