
To evaluate television and simultaneous electronic devices use in adolescents with musculoskeletal pain and musculoskeletal pain syndromes.
MethodsA cross-sectional study was performed in 299 healthy adolescents of a private school. All students completed a self-administered questionnaire, including: demographic data, physical activities, musculoskeletal pain symptoms, and use of simultaneous television/electronic devices (computer, internet, electronic games, and cell phones). Seven musculoskeletal pain syndromes were also evaluated: juvenile fibromyalgia, benign joint hypermobility syndrome, myofascial syndrome, tendinitis, bursitis, epicondylitis, and complex regional pain syndrome.
ResultsInter-rater agreement between pretest and retest was 0.83. Musculoskeletal pain and musculoskeletal pain syndrome were found in 183/299 (61%) and 60/183 (33%), respectively. The median age (15 [10–18] vs. 14 [10–18] years, p=0.032) and years of education (10 [5–12] vs. 9 [5–12] years, p=0.011) were significantly higher in adolescents with musculoskeletal pain when compared with those without this condition. The frequencies of female gender (59% vs. 47%, p=0.019), cell phone use (93% vs. 81%, p=0.003), and simultaneous use of at least two electronic devices (80% vs. 67%, p=0.011) were significantly higher in the former group. Further comparisons between adolescents with and without musculoskeletal pain syndromes revealed that the frequency of female gender was significantly higher in the former group (75% vs. 25%, p=0.002), and with a significantly reduced median of weekends/holidays electronic games use (1.5 [0–10] vs. 3 [0–17]h/day, p=0.006).
ConclusionsA high prevalence of musculoskeletal pain/syndromes was observed in female adolescents. Musculoskeletal pain was mostly reported at a median age of 15 years, and students used at least two electronic devices. Reduced use of electronic games was associated with musculoskeletal pain syndromes.
Avaliar o uso de televisão e dispositivos eletrônicos em adolescentes com dor e síndromes musculoesqueléticas.
MétodosFoi feito um estudo transversal com 299 adolescentes saudáveis de uma escola particular. Todos os alunos responderam a um questionário autoaplicável, que incluiu perguntas sobre: dados demográficos, prática de atividade física, sintomas de dor musculoesquelética e o uso de televisão/ dispositivos eletrônicos (computador, internet, jogos eletrônicos e celular). Sete síndromes musculoesqueléticas foram avaliadas: fibromialgia juvenil, síndrome de hipermobilidade articular benigna, síndrome miofascial, tendinite, bursite, epicondilite e síndrome de dor regional complexa.
ResultadosA concordância entre o pré-teste e reteste foi de 0,83. Dor musculoesquelética e síndromes musculoesqueléticas foram encontradas em 183/299 (61%) e 60/183 (33%), respectivamente. As medianas de idade [15 (10-18) versus 14 (10-18) anos, p=0,032] e de anos de escolaridade [10 (5-12) vs. 9 (5-12) anos, p=0,010] foram significantemente maiores em adolescentes com dor musculoesquelética em comparação com aqueles sem essa condição. As frequências do sexo feminino (59% versus 47% p=0,019), uso do telefone celular (93% contra 81%, p=0,003) e do uso simultâneo de pelo menos dois dispositivos eletrônicos (80% vs. 67%, p=0,011) foram significantemente maiores no grupo de adolescentes com dor musculoesquelética. Comparações adicionais entre os adolescentes com e sem síndromes musculoesqueléticas revelaram que a frequência do sexo feminino foi significantemente maior no primeiro grupo de (75% versus 25%, p=0,002), e com mediana significantemente reduzida de horas de jogos eletrônicos aos finais de semana e feriados [1,5 (0-10) vs. 3 (0-17) horas/dia, p=0,006].
ConclusõesUma alta prevalência de dor/síndromes musculoesqueléticas foi observada em adolescentes do sexo feminino. A dor musculoesquelética foi predominantemente relatada entre alunos com mediana de idade de 15 anos e que usavam pelo menos dois dispositivos eletrônicos simultaneamente. O uso reduzido de jogos eletrônicos foi associado à presença de síndromes musculoesqueléticas.
Idiopathic musculoskeletal pain is the most important cause of non-inflammatory pain in adolescents, ranging from 30% to 65%.1–6 In addition, adolescents may present musculoskeletal pain syndromes that are generally under-diagnosed conditions and could influence daily life activities, such as decreased recreational levels.7,8
The pathophysiology of musculoskeletal pain is multifactorial. The use of electronic devices (computer, internet, electronic games, and cell phones) has been reported as a risk factor associated with musculoskeletal pain6–9; however, studies rarely have evaluated specific musculoskeletal pain syndromes.10
In addition, to the best of the authors’ knowledge, none of them assessed concomitantly the use of television, digital media, musculoskeletal pain, and seven musculoskeletal pain syndromes (juvenile fibromyalgia, benign joint hypermobility syndrome, myofascial syndrome, tendinitis, bursitis, epicondylitis, and complex regional pain syndrome) in adolescents.
Therefore, the objective of the present study was to assess musculoskeletal pain and musculoskeletal pain syndromes in adolescents, and to compare demographic data, physical activities, and characteristics of television and simultaneous media use in adolescents with and without musculoskeletal pain, as well as in adolescents with and without musculoskeletal pain syndromes.
MethodsA cross-sectional study was performed in a private school of the city of São Paulo, Brazil. A total school population of 331 healthy adolescents (10–19 years old) was invited to participate from October to December 2014. None of them had musculoskeletal pain secondary to infectious, rheumatic, oncologic, genetics, diabetes mellitus, or thyroid diseases, nor had reported recent trauma. The Ethics Committee of Faculdade de Medicina, Universidade de São Paulo, Brazil approved this study (identification number 24668013.5.0000.0065). Informed consent was obtained from the adolescents and their legal guardians.
Thirty-two of the 331 healthy adolescents were excluded due to adolescent/parental refusal (n=30) and errors of omission (n=2). Thus, a total of 299 healthy adolescents were included in the study.
All students completed a self-administered questionnaire (Supplementary File) in the classroom. The median duration of questionnaire answer was 20min (range: 15–30min). This survey was confidential and covered the following aspects: demographic data (age, gender, socioeconomic classes,11 years of education), physical activities, musculoskeletal pain symptoms, and use of television and digital media (computer, internet, electronic games, and cell phones). Electronic games evaluated in this study were mobile handheld devices (keypad phones, touchscreen smartphones, tablet, computers, Playstation portable [PSP]) (Sony Corporation of America, NY, USA), Nintendo DS (Nintendo®, Kyoto, Japan), and Game Boy (Nintendo®, Kyoto, Japan), Wii (Nintendo®, Kyoto, Japan), Playstation (Sony Corporation of America, NY, USA), and Xbox (Sony Corporation of America, NY, USA). The questionnaire also included pictures of different body areas placed next to the questions to help the adolescents identify the body area of the musculoskeletal pain symptoms, and was modified as previously published by this group.1,2,10 These features were evaluated at any time during the three months preceding the study.
Pretest and retest of the questionnaire were performed in 25 adolescents in December 2014. The pretest was conducted to adapt the questionnaire, to ensure students’ understanding, coordinate the scheduling of a physical examination, and to assess the applicability and functionality of the database. A few words were changed in the questionnaire (e.g., the words “Playstation portable” were added as one of the portable electronic games and the word “average” was included when rephrasing some questions). These students were randomly selected and a mean interval of 30 days between pretest and retest of the questionnaire was observed.
Four trained physicians carried out a physical examination of musculoskeletal system immediately after the self-administered questionnaire. Students who answered “yes” on question number 46 (“Did you have any pain on muscles, bones, or joints in the past three months?”) were systematically evaluated. The physical examination was performed in a clinical examination room at the school in those adolescents who reported musculoskeletal pain during the last three months. The median duration of the musculoskeletal system exam was 10min (range: 5–15min).
Seven musculoskeletal pain syndromes were evaluated: juvenile fibromyalgia, benign joint hypermobility syndrome, myofascial syndrome, tendinitis, bursitis, epicondylitis, and complex regional pain syndrome. Juvenile fibromyalgia was diagnosed in cases with history of widespread pain for at least three months and the presence of 11 of 18 tender points examined bilaterally, according to the American College of Rheumatology criteria.12 Benign joint hypermobility syndrome was diagnosed using the Beighton criteria,13 and was defined as the presence of musculoskeletal pain without systemic diseases14 and ≥five out of nine points of hypermobility13–15: 1) touch thumbs to volar forearms (one point each for right side and left side), 2) extend fifth metacarpophalangeal joint to 90° (one point each for right side and left side), 3) >10° hyperextension of elbow (one point each for right side and left side), 4) >10° hyperextension of knee (one point each for right side and left side), and 5) touch palms to floor with knees straight (one point). Myofascial syndrome was diagnosed in the presence of active trigger points assessed bilaterally in specific muscles or muscular groups (trapezius, subscapular, posterior cervical muscles, biceps, triceps, brachioradial, extensor, and flexor musculature of the hand, wrist and fingers, and intrinsic muscles of the hand), and soft tissues stress injuries (tendinitis, bursitis, and epicondylitis), as previously reported.1,2,10 The clinical diagnosis of tendinitis was based on localized pain or tenderness to palpation on tendons of shoulders, elbows, wrists, knees, and heels.2 Complex regional pain syndrome was diagnosed according to the Budapest criteria.16,17
Statistical analysisThe sample size provided power of 80% to find differences from 6.5% to 17% in the frequency of use of different digital devices among the groups with and without musculoskeletal pain (Graphpad StatMate 1.01, GraphPad Software, Inc., CA, USA). The Kappa index was used to assess the questionnaire reliability between pretest and retest. The results for continuous variables were presented as median (minimum and maximum value) or mean±standard deviation (SD); for categorical variables, as frequency (percentage). The scores that had normal distribution were compared using Student's t-test. The scores that had abnormal distribution were evaluated by Mann–Whitney's test. For the categorical variables, the differences were calculated by Fisher's exact test or the chi-squared test, accordingly. p-values ≤0.05 were considered to be statistically significant.
ResultsThe Kappa index between pretest and retest was 0.83, demonstrating an excellent reliability in the adolescent's responses.18 Musculoskeletal pain was reported by 183 (61%) of the 299 adolescents. The main locations of reported musculoskeletal pain were: 121 (66%) back, 90 (49%) neck, 76 (41%) lower limbs, 58 (31%) shoulders/arms, and 35 (19%) wrist/hands. Temporary agency work was reported in nine (5%) of 183 adolescents with musculoskeletal pain, and only one of them worked 5h/day as a video editor.
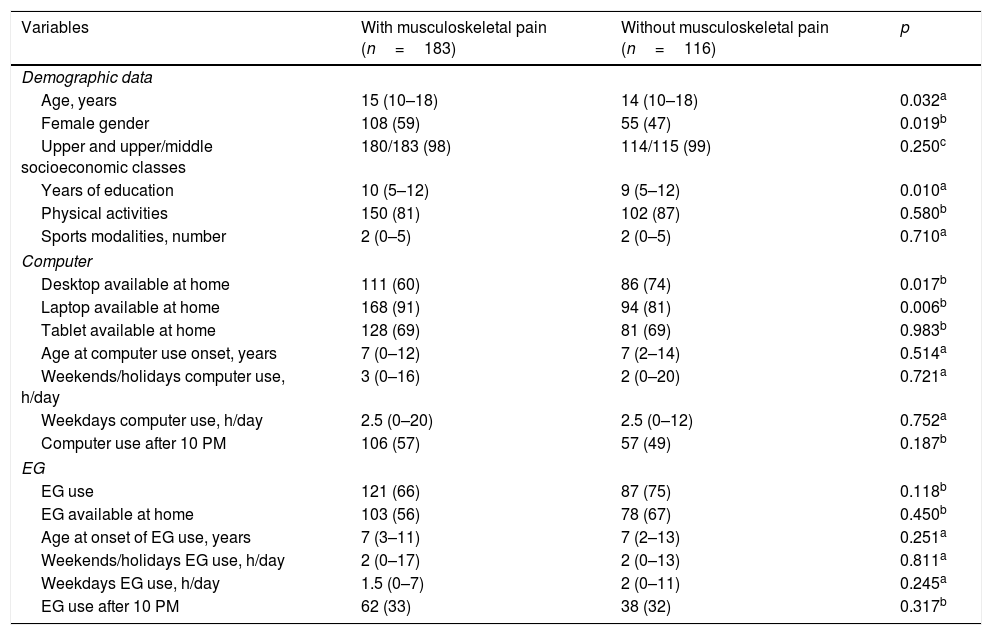
Table 1 presents the demographic data, physical activities, and characteristics of computer and electronic game use in adolescents with musculoskeletal pain compared to those without musculoskeletal pain. The median age (15 [10–18] vs. 14 [10–18] years, p=0.032) and years of education (10 [5–12] vs. 9 [5–12] years, p=0.011) were significantly higher in adolescents with musculoskeletal pain when compared with those without this condition. The frequencies of female gender (59% vs. 47%, p=0.019) were significantly higher in the former group. The frequency of laptop available at home was significantly higher in the former group (91% vs. 81%, p=0.006), whereas the frequency of desktop available at home was significantly lower (60% vs. 74%, p=0.017). No differences were observed in physical activities and electronic games use in both groups (Table 1).
Demographic data, physical activities, and characteristics of computer and electronic game (EG) use in adolescents with vs. without musculoskeletal pain.
| Variables | With musculoskeletal pain (n=183) | Without musculoskeletal pain (n=116) | p |
|---|---|---|---|
| Demographic data | |||
| Age, years | 15 (10–18) | 14 (10–18) | 0.032a |
| Female gender | 108 (59) | 55 (47) | 0.019b |
| Upper and upper/middle socioeconomic classes | 180/183 (98) | 114/115 (99) | 0.250c |
| Years of education | 10 (5–12) | 9 (5–12) | 0.010a |
| Physical activities | 150 (81) | 102 (87) | 0.580b |
| Sports modalities, number | 2 (0–5) | 2 (0–5) | 0.710a |
| Computer | |||
| Desktop available at home | 111 (60) | 86 (74) | 0.017b |
| Laptop available at home | 168 (91) | 94 (81) | 0.006b |
| Tablet available at home | 128 (69) | 81 (69) | 0.983b |
| Age at computer use onset, years | 7 (0–12) | 7 (2–14) | 0.514a |
| Weekends/holidays computer use, h/day | 3 (0–16) | 2 (0–20) | 0.721a |
| Weekdays computer use, h/day | 2.5 (0–20) | 2.5 (0–12) | 0.752a |
| Computer use after 10 PM | 106 (57) | 57 (49) | 0.187b |
| EG | |||
| EG use | 121 (66) | 87 (75) | 0.118b |
| EG available at home | 103 (56) | 78 (67) | 0.450b |
| Age at onset of EG use, years | 7 (3–11) | 7 (2–13) | 0.251a |
| Weekends/holidays EG use, h/day | 2 (0–17) | 2 (0–13) | 0.811a |
| Weekdays EG use, h/day | 1.5 (0–7) | 2 (0–11) | 0.245a |
| EG use after 10 PM | 62 (33) | 38 (32) | 0.317b |
Results are presented in number (%) and median (minimum and maximum values).
EG, electronic games.
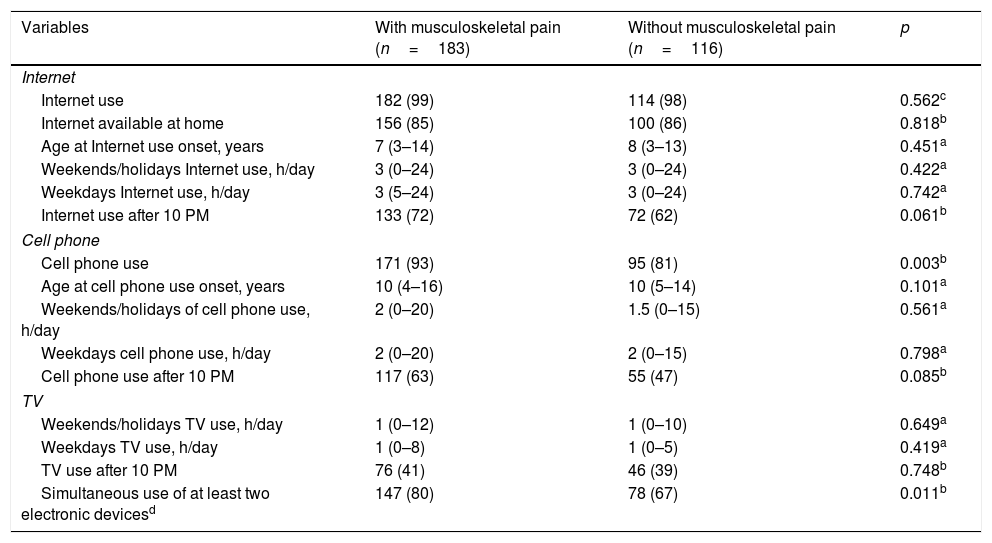
Table 2 presents the characteristics of Internet, cell phone, television, and simultaneous media use in adolescents with versus without musculoskeletal pain. The frequencies of cell phone use (93% vs. 81%, p=0.003) and simultaneous use of at least two electronic media (computer, electronic game, Internet, cell phone and/or television; 80% vs. 67%, p=0.011) were significantly higher in adolescents with musculoskeletal pain when compared with those without musculoskeletal pain. No differences were evidenced in Internet and television use in both groups (Table 2).
Characteristics of Internet, cell phone, television (TV), and simultaneous media use in adolescents with vs. without musculoskeletal pain.
| Variables | With musculoskeletal pain (n=183) | Without musculoskeletal pain (n=116) | p |
|---|---|---|---|
| Internet | |||
| Internet use | 182 (99) | 114 (98) | 0.562c |
| Internet available at home | 156 (85) | 100 (86) | 0.818b |
| Age at Internet use onset, years | 7 (3–14) | 8 (3–13) | 0.451a |
| Weekends/holidays Internet use, h/day | 3 (0–24) | 3 (0–24) | 0.422a |
| Weekdays Internet use, h/day | 3 (5–24) | 3 (0–24) | 0.742a |
| Internet use after 10 PM | 133 (72) | 72 (62) | 0.061b |
| Cell phone | |||
| Cell phone use | 171 (93) | 95 (81) | 0.003b |
| Age at cell phone use onset, years | 10 (4–16) | 10 (5–14) | 0.101a |
| Weekends/holidays of cell phone use, h/day | 2 (0–20) | 1.5 (0–15) | 0.561a |
| Weekdays cell phone use, h/day | 2 (0–20) | 2 (0–15) | 0.798a |
| Cell phone use after 10 PM | 117 (63) | 55 (47) | 0.085b |
| TV | |||
| Weekends/holidays TV use, h/day | 1 (0–12) | 1 (0–10) | 0.649a |
| Weekdays TV use, h/day | 1 (0–8) | 1 (0–5) | 0.419a |
| TV use after 10 PM | 76 (41) | 46 (39) | 0.748b |
| Simultaneous use of at least two electronic devicesd | 147 (80) | 78 (67) | 0.011b |
Results are presented in number (%) and median (minimum and maximum values).
Electronic games use was reported by 208/299 (70%) adolescents: Wii, Playstation or Xbox in 65/208 (31%) adolescents; 53/208 (25%) mobile handheld devices (cell phones, touchscreen smartphones, tablet, PSP, Nintendo DS, and Game Boy); and 38/208 (18%) laptop and desktop. Fifty-two of 208 (25%) adolescents used more than one gaming platform.
At least one musculoskeletal pain syndrome was observed in 60/183 (33%) adolescents. Seven of these 60 adolescents had more than one musculoskeletal pain syndromes. Myofascial syndrome was observed in 36/183 (19%), and the main muscle involved was the trapezium (n=25). Tendinitis was diagnosed in 24/183 (13%), mainly localized in the carpal flexors and thumbs (n=18). Juvenile fibromyalgia occurred in four (2%) out of 183 adolescents, and benign joint hypermobility syndrome, in four (2%) out of 183. No cases of bursitis, epicondylitis, or complex regional pain syndrome were observed. The main locations of examined musculoskeletal pain were: 47/60 (78%), back; four, (6%) neck; 11 (18%) upper limbs; 16 (27%), wrist/hands; and eight (13%), lower limbs.
Further comparisons between adolescents with and without musculoskeletal pain syndromes revealed that the frequency of female gender was significantly higher in the former group (75% vs. 25%, p=0.002). The median of weekends/holidays electronic games use was significantly reduced in adolescents with musculoskeletal pain syndromes when compared with those without these conditions (1.5 [0–10] vs. 3 [0–17]h/day, p=0.006). Age, socioeconomic class, years of education, physical activities, and characteristics of television, computer, Internet, and cell phone use were similar in both groups (p>0.05).
DiscussionThe present study indicated a high frequency of musculoskeletal pain and musculoskeletal pain syndromes in healthy adolescents. These symptoms were more commonly reported at median age of 15 years (vs. 14 years) in adolescents using at least two electronic devices. Female gender and a reduced use of electronic games were associated with musculoskeletal pain syndromes.
The assessment of self-report and standardized questionnaire was important, and this tool included pictures of different body areas to indicate the location of musculoskeletal pain.1,2,10 The use of a questionnaire with excellent test–retest reliability was also relevant for this population,18 reducing the effect of memory bias, as also has been shown in other studies of this group.1,2,10 Another strength of this study was the systematic musculoskeletal physical examination of adolescents who complained of musculoskeletal pain, using established criteria for musculoskeletal pain syndromes.1,2,10,12,16,17
In adolescents, musculoskeletal pain is multifactorial. There are several risk factors for musculoskeletal pain, such as gender, age, and use of electronic devices.4,9,19 Other risk factors may be associated to these symptoms during the growth process, such as sport with strength training, posture, and recreational activities.7 In this study, musculoskeletal pain was observed in approximately two-thirds of subjects and predominantly in older adolescents, as reported in other studies in Brazil, Finland, and Italy.5,8,20 The increased reports of pain with age in the present study may be related to a high perception and memory of pain in adolescents, and further studies will be necessary to clarify this point.
Regarding device availability, adolescents with musculoskeletal pain reported frequent use of a laptop at home, whereas desktop availability at home was reduced. These findings may be related to electronic devices use, probably because desktops are more ergonomic than laptops.21–23
Interestingly, cell phone use was commonly observed in adolescents with musculoskeletal pain in the present study, while television use was reduced. The most frequent sites of these complaints were the back, neck, and shoulders, and cell phone use may be responsible for musculoskeletal pain. Since the launch of the first generation iPhone (Apple®, CA, USA), the smartphone technology has altered adolescents’ daily habits of electronic devices use.9 Indeed, a recent systematic review found that high frequency of phone calls, texting, and gaming were associated with musculoskeletal disorders, especially those related to neck flexion posture.9
Additionally, simultaneous use of at least two electronic devices was associated with musculoskeletal pain in the present adolescents. The possible use of several muscles, tendons, fascias, ligaments, and enthesis by adolescents using at least two electronic devices at the same time may have contributed to an additional musculoskeletal stress.
Musculoskeletal syndromes were observed in one third of adolescents with musculoskeletal pain, especially in females. This finding is yet unclear, and possible related to the fact that women are more likely to complain than men, especially amplified musculoskeletal pain syndromes.2 Adolescents with those conditions spent fewer hours gaming during the weekends and holidays, probably inducing limitation of such recreational activities. However, a longitudinal assessment will be necessary to confirm this result.
Importantly, myofascial syndrome and tendinitis were the most prevalent syndromes observed in the present study. These musculoskeletal injuries have been rarely studied in adolescent populations,10,24 and may be related to inadequate posture and repetitive movements using electronic devices. Since 1990, when the so-called “Nintendinitis” was first described,25 several injuries associated with video games and new technologies have been increasingly observed among children and adolescents.3,9,24,26
This study has limitations. The selected population of a private school including adolescents of upper and upper/middle socio-economic classes with a low frequency of work activities was a two-edged sword, since musculoskeletal pain may be related to repeated movements.16 In turn, it is possible that work activities may prevent musculoskeletal pain caused by electronic devices, by increasing the ability to tolerate low-load demands from their use. Other issues related to musculoskeletal pain and musculoskeletal pain syndromes, such as emotional disorders and other risk behavior, were not studied herein. Moreover, self-report of electronic device use is likely to include an amount of error when summarizing the previous three months. Further studies will be necessary to evaluate ergonomics,27–29 such as body posture and home/workplace set-up in this population using multiple electronic devices.
In conclusion, a high prevalence of musculoskeletal pain and musculoskeletal pain syndromes was observed in female adolescents. Musculoskeletal pain was more commonly reported at a median age of 15 years (vs. 14 years) in adolescents using at least two electronic devices. Cell phone use was associated with musculoskeletal pain, and the most frequent sites of these complaints were the back, neck, and shoulders. Reduced electronic games use was associated with musculoskeletal pain syndromes.
FundingThis study was supported by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq 303422/2015-7 to CAS), Federico Foundation, Switzerland (to CAS) and by Núcleo de Apoio à Pesquisa “Saúde da Criança e do Adolescente” da USP (NAP-CriAd) to CAS.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank to Ulysses Doria-Filho for the statistical analysis and Marta Leal for contribution in the questionnaire. They would also like to thank all students, parents, and teachers of a private school in Sao Paulo, Brazil.
Please cite this article as: Queiroz LB, Lourenço B, Silva LE, Lourenço DM, Silva CA. Musculoskeletal pain and musculoskeletal syndromes in adolescents are related to electronic devices. J Pediatr (Rio J). 2018;94:673–9.
Study conducted at Universidade de São Paulo (USP), Faculdade de Medicina, Hospital das Clínicas, Instituto da Criança, São Paulo, SP, Brazil.




