
To identify associations between maternal restrictive feeding practices for child weight control and sociodemographic, behavioral, dietetic, and anthropometric characteristics.
MethodsCross-sectional study with mothers of children aged 2–8 years. Maternal feeding practices were measured by the Comprehensive Feeding Practices Questionnaire, in private schools in Brazil. Bivariate and multivariate associations were performed, using nonparametric analyses to estimate odds ratios and significance levels.
ResultsMaternal restrictive feeding practices for weight control were independently associated with the mother's perception of her child being a little overweight/overweight/obese (OR=4.61, p=0.001), greater concern about the child's overweight (OR=2.61, p<0.001), child's overweight/obesity/severe obesity (OR= 2.18, p<0.001), and the child's greater intake of ultra-processed foods (OR=1.40, p=0.026).
ConclusionIn this study, the risk variables identified for the use of the maternal restrictive feeding practices to control the child's weight can be used to provide education and guidance interventions in health and education networks directed to groups with similar characteristics to those of the studied population.
Identificar associações da prática alimentar materna de restrição para controle de peso do filho com características sociodemográficas, comportamentais, dietéticas e antropométricas.
MétodosEstudo transversal com mães de crianças de dois a oito anos. Práticas maternas foram mensuradas por meio do instrumento Comprehensive Feeding Practices Questionnaire, em escolas privadas no Brasil. Para testar associações univariadas e múltiplas, foram feitos testes não paramétricos para cálculo de razões de chance (OR) e níveis de significância (valor de p).
ResultadosA restrição materna para controle do peso da criança foi independentemente associada com a percepção de que seu filho está um pouco gordo/gordo/muito gordo (OR = 4,61, p = 0,001), a preocupação quanto ao excesso de peso infantil (OR = 2,61, p<0,001), e em relação às características da criança, com o sobrepeso/obesidade/obesidade grave (OR = 2,18, p < 0,001) e o consumo de alimentos ultraprocessados (OR = 1,40, p = 0,026).
ConclusãoNeste estudo as variáveis de risco identificadas para o uso da prática materna de restrição para controle de peso do filho podem ser usadas para direcionar ações de educação e orientação nas redes de saúde e ensino, dirigidas a grupo com características similares as da população estudada.
Discussions regarding obesity have been widely reported in the world literature. The great investment in studies is related to the fact that obesity is considered an epidemic that affects all age groups of the population, as well as a challenge faced by researchers, as the disease has multifactorial causes.1
A specific research area focuses on the implication of the parents’ role in the development of childhood obesity2 and provides ample evidence on the importance of parental eating strategies for the child's food intake.
Regarding parental control practices, food restriction is the most often addressed in the literature.2 The restriction involves a type of limit imposed by parents on children related to the availability and amount of generally palatable and unhealthy foods.3 Considering the motivation for the use of this practice, parents are driven mainly by their desire to improve their child's health or modify their weight.4
The parental choice for the use of restrictive practices may be influenced by factors such as their perception of the child's weight,5,6 response to childhood excess weight,7 and concern with their child's weight.8,9
However, the parental use of restriction to control the child's eating habits can have counterproductive effects, as it interferes with internal signs of hunger and satiety and the child's self-regulation of appetite.10 In this scenario, some studies have verified that restrictive parental practices were associated with children's behavior of “eating in the absence of hunger”11 and, when exposed to options including what is restricted to them, they are more likely to choose these foods and eat them in excess.10,12 Finally, many of the studies on this subject have found that parental restriction is associated with excess weight in childhood.7,8,12,13
Considering the negative implications related to these restrictive practices, developing studies that enable understanding the factors associated with such parental attitudes may be a path that will allow identification of situations of risk for the child's nutritional and emotional health, as well as preventing the treatment of problems arising from such practices.
Therefore, the present study aimed to discuss the use of maternal food restriction aimed at the child's weight control, measured through the Comprehensive Feeding Practices Questionnaire (CFPQ), based on the investigation of possible associations and significant influences related to the practice. The hypothesis of the present study was that the practice of restriction would be associated mainly with maternal concern with excess weight, the perception of the child's nutritional status, and the parents’ nutritional status.
MethodsStudy designThe study used data from the Food Practices Study, a cross-sectional study aimed at adapting and validating the CFPQ in a sample of parents of preschoolers and school-aged children enrolled in private schools in the cities of São Paulo and Campinas, in the state of Sao Paulo, Brazil.14,15
ParticipantsMothers of children aged 2–8 years enrolled in the selected schools were included in the study. Questionnaires completed by anyone but the child's mother were excluded, as well as those whose children had pathologies that could influence feeding and maternal practices, foreign mothers, and questionnaires of children belonging to the same family (in those cases, only the younger sibling was kept in the sample).
To estimate of sample size, an alpha error probability of ≤0.05 and beta error of ≤0.20 were adopted. Having maternal schooling as the main independent variable for sample calculation, the proportion of mothers with a high level of schooling who would attain a high score on the CFPQ scale was estimated at 35%, while among those with low educational level, 45% would do so. The estimated sample size for each group of high and low maternal level of schooling resulted in 375 subjects, resulting in a minimum of 750 individuals. With the addition of 10% to compensate for eventual losses or unwillingness to participate, initially 825 mothers were considered.
ProceduresParticipants were recruited from private schools in the cities of São Paulo and Campinas, SP, Brazil. Fourteen of the 46 schools contacted accepted the invitation to participate in the study. More details on the procedures have been described elsewhere.14,15
MeasuresSociodemographic, behavioral, dietary, and anthropometric characteristics were reported by the mother. Ultraprocessed food intake was evaluated through a Food Frequency Questionnaire (FFQ), specially developed for the initial design and previously tested in a pilot study. The questionnaire included foods based on their association with obesity and their high frequency of intake among the Brazilian population.16 The ultraprocessed foods (artificial juice, breakfast cereals, chocolate, cookies with and without filling, processed dairy desserts, fast food, ice cream, instant noodles, lunch meats, soft drinks, candy and snacks) were added and then the means were calculated, and variable dichotomization was performed according to their distribution.
Risk mothers were considered as those whose children consumed ultraprocessed foods at least once a week, and absence of risk as those who reported not using such foods. The nutritional status of the child was calculated using the body mass index (BMI) z-score for age, and its classification was based on the growth curves of the World Health Organization (WHO).17,18 The cutoff points were based on the categories considering the weight and height self-reported by the mothers (for children aged <5 years: “very low weight” was defined as z-score <−3; “low weight”, z-score ≥−3 and <−2; “normal weight”, as z-score ≥−2 and <+1; “risk for overweight”, z-score ≥+1 and <+2; “overweight”, z-score ≥+2 and <+3; and “obesity”, as z-score ≥+3. For children aged ≥5 years: “very low weight” was defined as z-score <−3; “low weight,” z-score ≥−3 and <−2; “normal weight,” as z-score ≥−2 and <+1; “overweight,” z-score ≥+1 and <+2; “obesity,” as z-score ≥+2 and <+3; and “severe obesity,” as z-score ≥+3).
The questions related to maternal responsibility for the child's feeding and concerns regarding the child's excess weight were obtained from the Child Feeding Questionnaire.19 The maternal “weight control restriction” practice was measured using the Portuguese version of the CFPQ, through seven questions. The process of cross-cultural adaptation and validation of the questionnaire has been described in previous studies.14,15
Statistical analysisFirst, descriptive analyses were performed to determine the distribution of the variables and to identify the appropriate cutoff for dichotomization. For the analysis of the “restriction for weight control” feeding practice, considered the dependent variable, the scores were transformed into a scale from zero to 100. The score dichotomization considered the median value; scores >P50 were considered “at risk.” Univariate analyses were conducted between “restriction for weight control” and the independent variables (sociodemographic, behavioral, dietetic, and anthropometric factors). The value of p≤0.20 was considered in the univariate analyses for the inclusion of the independent variables in the multiple logistic regression model. The statistical significance in the final model was defined as p≤0.05. The model was adjusted for the mother's BMI and the child's age, as continuous variables, and for the child's gender. All statistical analyses were performed using the Stata statistical package (Stata Statistical Software: Release 14., College Station, TX, USA).
Ethical aspectsThis study was approved by the Research Ethics Committee of Universidade Federal de São Paulo. All participants of the original project signed the Informed Consent.
ResultsA total of 1178 questionnaires were answered, of which 251 were considered as losses due to lack of response in the items referring to the “weight control restriction” domain in the CFPQ and those that lacked much information. More details on exclusions and losses are described elsewhere.14,15
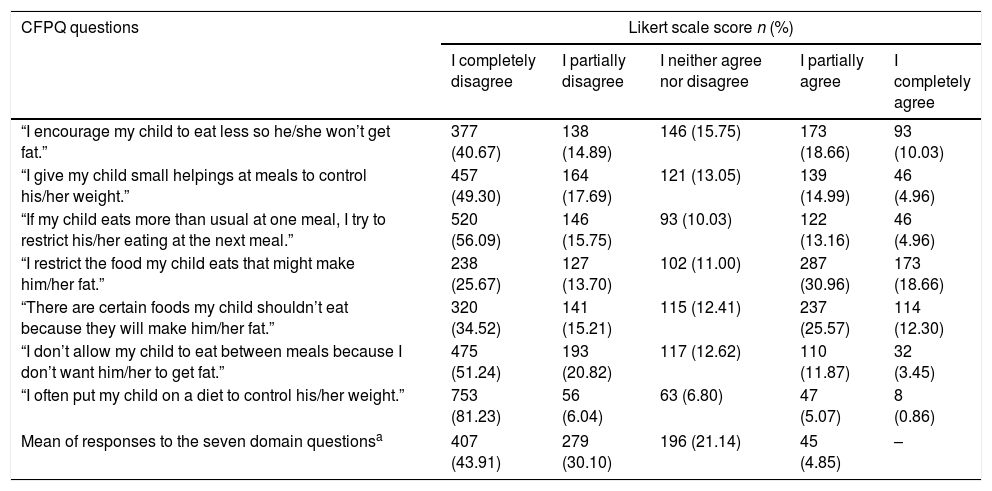
The data in Table 1 show the distribution of the CFPQ responses regarding the practice of “weight control restriction” in the total study sample. There are seven items that comprise the domain, and according to the average responses, 74% of the mothers reported disagreeing at some level with the statements about the restrictive practice, and none reported completely agreeing with all domain statements.
Distribution of the Comprehensive Feeding Practices Questionnaire responses related to the “restriction for weight control” domain in a sample of mothers of preschoolers and school-aged children enrolled in private schools of São Paulo and Campinas, SP, Brazil (n=927).
| CFPQ questions | Likert scale score n (%) | ||||
|---|---|---|---|---|---|
| I completely disagree | I partially disagree | I neither agree nor disagree | I partially agree | I completely agree | |
| “I encourage my child to eat less so he/she won’t get fat.” | 377 (40.67) | 138 (14.89) | 146 (15.75) | 173 (18.66) | 93 (10.03) |
| “I give my child small helpings at meals to control his/her weight.” | 457 (49.30) | 164 (17.69) | 121 (13.05) | 139 (14.99) | 46 (4.96) |
| “If my child eats more than usual at one meal, I try to restrict his/her eating at the next meal.” | 520 (56.09) | 146 (15.75) | 93 (10.03) | 122 (13.16) | 46 (4.96) |
| “I restrict the food my child eats that might make him/her fat.” | 238 (25.67) | 127 (13.70) | 102 (11.00) | 287 (30.96) | 173 (18.66) |
| “There are certain foods my child shouldn’t eat because they will make him/her fat.” | 320 (34.52) | 141 (15.21) | 115 (12.41) | 237 (25.57) | 114 (12.30) |
| “I don’t allow my child to eat between meals because I don’t want him/her to get fat.” | 475 (51.24) | 193 (20.82) | 117 (12.62) | 110 (11.87) | 32 (3.45) |
| “I often put my child on a diet to control his/her weight.” | 753 (81.23) | 56 (6.04) | 63 (6.80) | 47 (5.07) | 8 (0.86) |
| Mean of responses to the seven domain questionsa | 407 (43.91) | 279 (30.10) | 196 (21.14) | 45 (4.85) | – |
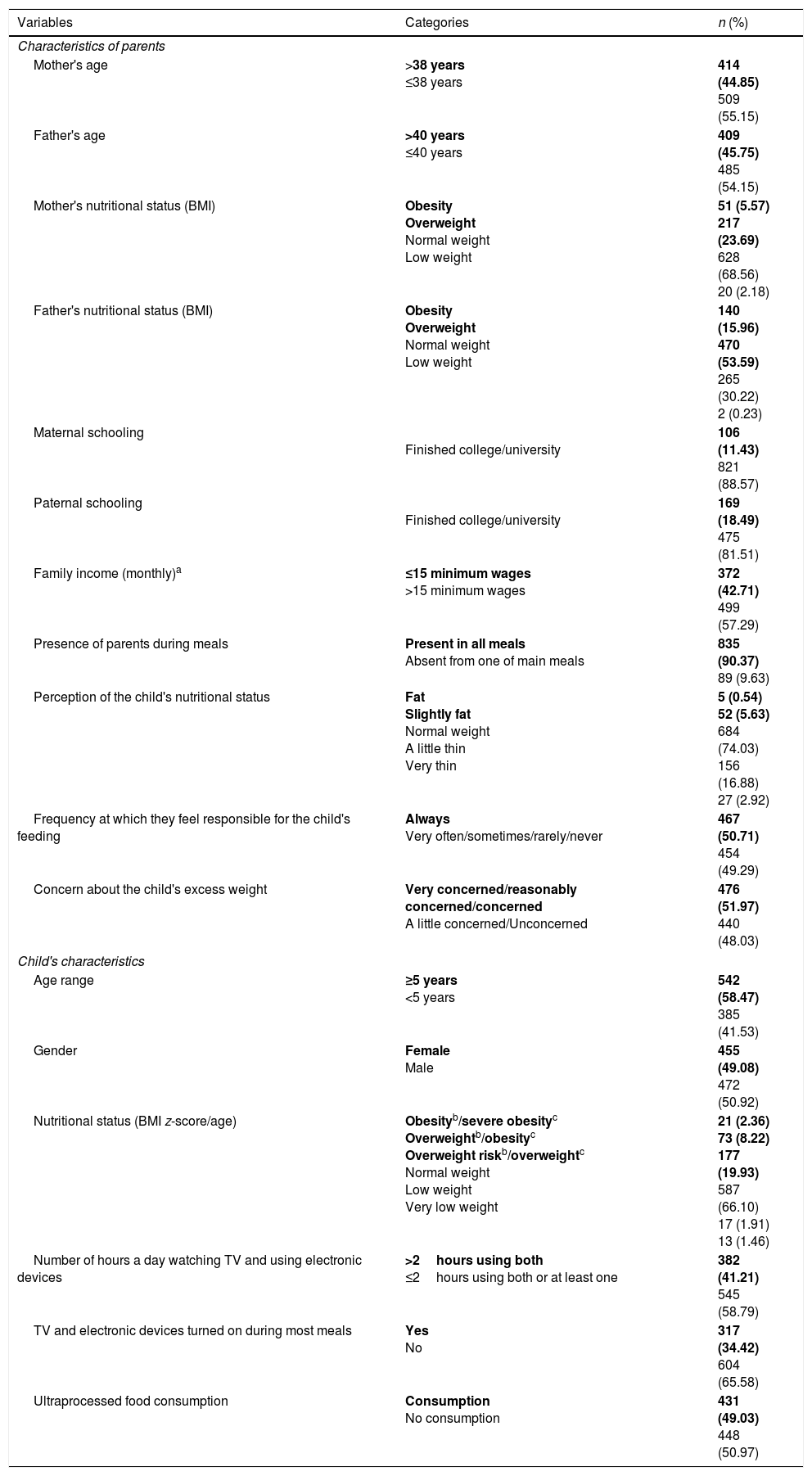
The analysis of maternal characteristics disclosed a high level of schooling among the studied population, with less than a quarter of the mothers reporting having not finished college/university (11.43%) and more than half (57.29%) reported a monthly income >15 minimum wages. According to the BMI, about one-third of the mothers had excess weight (29.26%), differently from the fathers, for which this item represented three quarters of the sample (69.56%). Predominantly, nine out of ten participants reported that at least one of the parents was present at all the child's meals (90.37%). Considering child's characteristics, the sample was well distributed according to gender (49.08% girls) and almost half of the children (49.03%) reported ultraprocessed food consumption during the seven days prior to the survey. Finally, although 30% of the children were classified as having excess weight, only 6% of the mothers perceived them as being slightly fat (Table 2).
Characteristics of the study population (n=927).
| Variables | Categories | n (%) |
|---|---|---|
| Characteristics of parents | ||
| Mother's age | >38 years ≤38 years | 414 (44.85) 509 (55.15) |
| Father's age | >40 years ≤40 years | 409 (45.75) 485 (54.15) |
| Mother's nutritional status (BMI) | Obesity Overweight Normal weight Low weight | 51 (5.57) 217 (23.69) 628 (68.56) 20 (2.18) |
| Father's nutritional status (BMI) | Obesity Overweight Normal weight Low weight | 140 (15.96) 470 (53.59) 265 (30.22) 2 (0.23) |
| Maternal schooling | Finished college/university | 106 (11.43) 821 (88.57) |
| Paternal schooling | Finished college/university | 169 (18.49) 475 (81.51) |
| Family income (monthly)a | ≤15 minimum wages >15 minimum wages | 372 (42.71) 499 (57.29) |
| Presence of parents during meals | Present in all meals Absent from one of main meals | 835 (90.37) 89 (9.63) |
| Perception of the child's nutritional status | Fat Slightly fat Normal weight A little thin Very thin | 5 (0.54) 52 (5.63) 684 (74.03) 156 (16.88) 27 (2.92) |
| Frequency at which they feel responsible for the child's feeding | Always Very often/sometimes/rarely/never | 467 (50.71) 454 (49.29) |
| Concern about the child's excess weight | Very concerned/reasonably concerned/concerned A little concerned/Unconcerned | 476 (51.97) 440 (48.03) |
| Child's characteristics | ||
| Age range | ≥5 years <5 years | 542 (58.47) 385 (41.53) |
| Gender | Female Male | 455 (49.08) 472 (50.92) |
| Nutritional status (BMI z-score/age) | Obesityb/severe obesityc Overweightb/obesityc Overweight riskb/overweightc Normal weight Low weight Very low weight | 21 (2.36) 73 (8.22) 177 (19.93) 587 (66.10) 17 (1.91) 13 (1.46) |
| Number of hours a day watching TV and using electronic devices | >2hours using both ≤2hours using both or at least one | 382 (41.21) 545 (58.79) |
| TV and electronic devices turned on during most meals | Yes No | 317 (34.42) 604 (65.58) |
| Ultraprocessed food consumption | Consumption No consumption | 431 (49.03) 448 (50.97) |
The results in bold represent the category at risk for each variable.
BMI, body mass index.
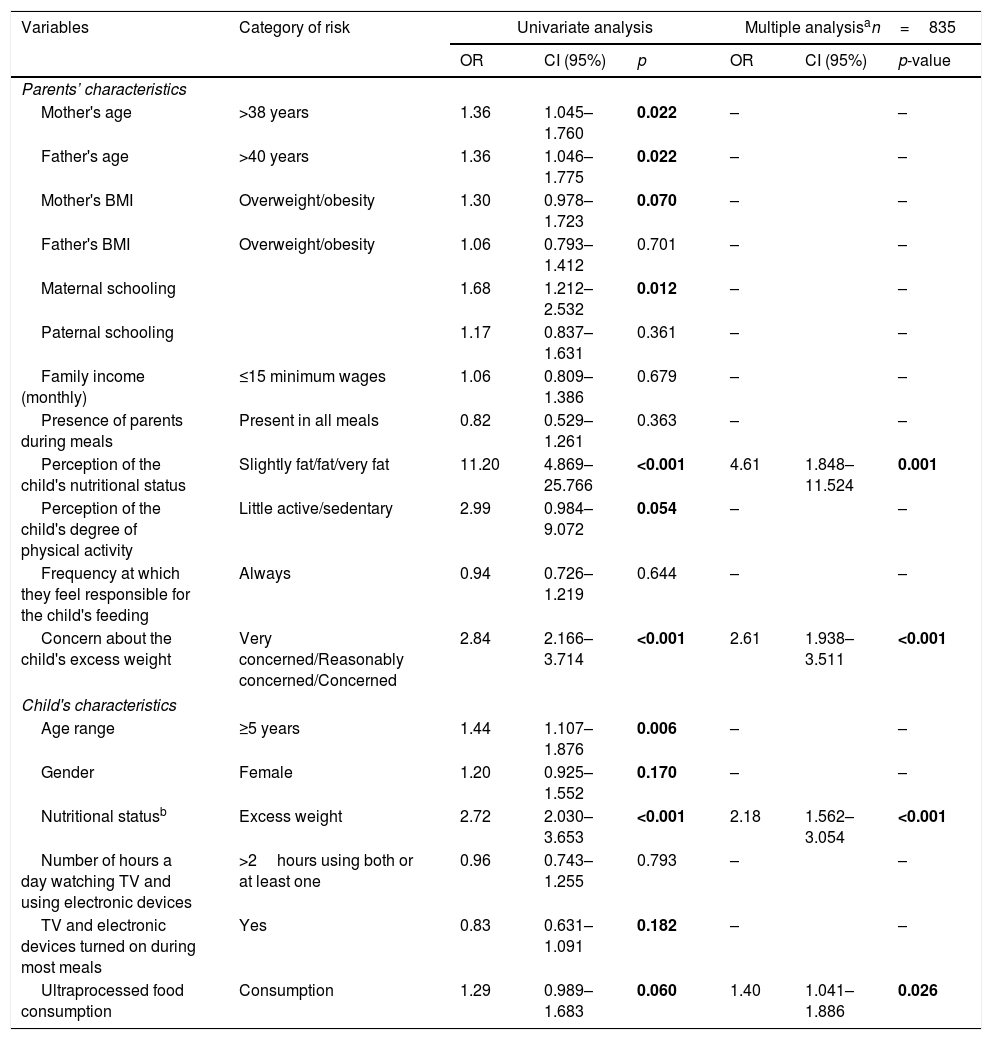
Table 3 shows the data related to the univariate analysis and the multiple logistic regression between the “restriction for weight control” and other paternal and child characteristics. Several eligible variables (p≤0.20) in the univariate analysis were inserted into the multiple regression model and, after controlling for the child's gender and age and the mother's BMI, the maternal restriction was independently associated with the perception that the child is slightly fat/fat/very fat (OR=4.61, p=0.001), higher concern about the child's excess weight (OR=2.61, p<0.001), with the child's overweight/obesity/severe obesity (OR=2.18, p<0.001) and the child's consumption of ultraprocessed foods (OR=1.40, p=0.026).
Univariate analysis and multiple logistic regression between maternal restrictive feeding practices measured by the Comprehensive Feeding Practices Questionnaire and parents’ and child's characteristics.
| Variables | Category of risk | Univariate analysis | Multiple analysisan=835 | ||||
|---|---|---|---|---|---|---|---|
| OR | CI (95%) | p | OR | CI (95%) | p-value | ||
| Parents’ characteristics | |||||||
| Mother's age | >38 years | 1.36 | 1.045–1.760 | 0.022 | – | – | |
| Father's age | >40 years | 1.36 | 1.046–1.775 | 0.022 | – | – | |
| Mother's BMI | Overweight/obesity | 1.30 | 0.978–1.723 | 0.070 | – | – | |
| Father's BMI | Overweight/obesity | 1.06 | 0.793–1.412 | 0.701 | – | – | |
| Maternal schooling | 1.68 | 1.212–2.532 | 0.012 | – | – | ||
| Paternal schooling | 1.17 | 0.837–1.631 | 0.361 | – | – | ||
| Family income (monthly) | ≤15 minimum wages | 1.06 | 0.809–1.386 | 0.679 | – | – | |
| Presence of parents during meals | Present in all meals | 0.82 | 0.529–1.261 | 0.363 | – | – | |
| Perception of the child's nutritional status | Slightly fat/fat/very fat | 11.20 | 4.869–25.766 | <0.001 | 4.61 | 1.848–11.524 | 0.001 |
| Perception of the child's degree of physical activity | Little active/sedentary | 2.99 | 0.984–9.072 | 0.054 | – | – | |
| Frequency at which they feel responsible for the child's feeding | Always | 0.94 | 0.726–1.219 | 0.644 | – | – | |
| Concern about the child's excess weight | Very concerned/Reasonably concerned/Concerned | 2.84 | 2.166–3.714 | <0.001 | 2.61 | 1.938–3.511 | <0.001 |
| Child's characteristics | |||||||
| Age range | ≥5 years | 1.44 | 1.107–1.876 | 0.006 | – | – | |
| Gender | Female | 1.20 | 0.925–1.552 | 0.170 | – | – | |
| Nutritional statusb | Excess weight | 2.72 | 2.030–3.653 | <0.001 | 2.18 | 1.562–3.054 | <0.001 |
| Number of hours a day watching TV and using electronic devices | >2hours using both or at least one | 0.96 | 0.743–1.255 | 0.793 | – | – | |
| TV and electronic devices turned on during most meals | Yes | 0.83 | 0.631–1.091 | 0.182 | – | – | |
| Ultraprocessed food consumption | Consumption | 1.29 | 0.989–1.683 | 0.060 | 1.40 | 1.041–1.886 | 0.026 |
OR, odds ratio; 95% CI, 95% confidence interval; minimum wage in 2014, R$ 724.00; BMI, body mass index.
Results in bold are significant (in the univariate analysis p≤0.20, and in the multiple analysis, p≤0.05).
The aim of this study was to identify associations between maternal practices of “restriction for weight control” with sociodemographic, behavioral, dietary and anthropometric characteristics of parents and children.
The use of the restriction was associated with mother's perception of the child's excessive weight, with a magnitude of effect of almost 5 (OR=4.61, p=0.001). In agreement with these results, Francis et al.5 verified that the perception about the child's nutritional state contributed significantly to the greater use of restrictive feeding practices. These data may reflect a process in which the mother wants her child to be leaner,20 stimulated by the perception of the child's nutritional status, which may or may not correspond to the actual BMI.6
Several studies that assessed the perception of the child's nutritional state aimed at investigating the underestimation or overestimation of the children's weight by the mothers.21–24 These researchers found that most mothers cannot accurately perceive the weight of overweight children. When considering that perception is a subjective fact, regarding the maternal feeding practice, the child's actual weight may possibly matter less than the way the mother perceives it.23
A common assumption regarding the subject of childhood obesity is that the maternal perception that her child is overweight is crucial for the intervention and efforts to control food and nutritional deviations.21,25 It is therefore recommended that mothers be informed about the nutritional status of their children and made aware of the risks associated with health. However, it is important to recognize that this information alone can have a negative impact on maternal actions, such as the restrictive feeding practices.
According to the hypothesis, in this sample, the practice of “restriction for weight control” was reported by mothers concerned about their child's excess weight, with an increased risk of approximately 2.6-fold (OR=2.61, p<0.001), as found in previous studies.8,26 Mothers may be primarily concerned with the future consequences regarding health and social stigma if the child is overweight, and this occurs regardless of the child's actual nutritional status.26
Francis et al.5 verified that parental concern is an additional and important influence on restrictive dietary practices, also present in overweight mothers, which may be partly due to their own excess weight and the fear that the child will face a similar problem. In this sample, although a higher frequency of restriction practices in overweight and obese mothers was observed in the univariate analysis (OR=1.3, p=0.070), this association did not show enough statistical significance to be included as an independent risk factor in the multiple logistic model.
One should consider that the maternal perception and concern about the child's excess weight are necessary for studies on the treatment of obesity, but this finding also suggests a paradox. Some level of concern is required for parents to reflect on and change their behaviors regarding child feeding practices; however, excessive concern can lead to harmful practices such as restriction.6 Excessive parental control can disrupt the child's capacity to exercise appetite self-regulation and reinforce inappropriate eating behaviors.26
There is some evidence that high levels of maternal control are associated with excess weight in childhood and increased intake of palatable foods.10,27 As expected, the results of this study also indicate that the children's nutritional status (overweight/obesity/severe obesity) may influence the mothers’ restriction practices (OR=2.18, p≤0.001), which is consistent with other analyses on food intake regulation in preschool children, showing that higher levels of restrictive practices were associated with higher levels of child adiposity.12
When describing a model of obesity propensity in children, Costanzo and Woody26 suggested that parents end up exercising greater control over foods when they observe that the child is at risk for developing nutritional disorders. However, as in previous cross-sectional studies, it is not possible to infer the direction of the observed association, i.e., whether restrictive feeding practices result in lower or greater weight gain, and whether it is a reaction to the child's nutritional status or if there are other factors involved.28
In the present study's results, the use of “restriction for weight control” was also associated with ultraprocessed food consumption (OR=1.40, p=0.026). Several studies have indicated that restriction may increase the children's preferences for restricted foods,5,21,27 impair self-regulation,10,26 and increase children's food intake,12 especially of palatable foods, such as those with high fat and sugar contents, which may lead to excessive weight gain.
The practice may also draw the children's attention to these foods, increasing their desire to consume them, which shows that the use of the restriction is not an adequate alternative to promote moderation in consumption, and may even have the opposite effect, by stimulating the intake of foods that should be avoided.10,27
The present study has some limitations. First, it was demonstrated that the sample was quite homogeneous, with the level of schooling and family income being relatively high, which limits the generalization of the findings to the entire Brazilian population. Therefore, comparisons with other populations with lower incomes and levels of schooling should be made with caution. The self-reported nature of the anthropometric, dietary, and behavioral measures is a limitation present in most school-based surveys on maternal behavior. That occurs because they can be answered in a way that corresponds to what is perceived as socially desirable, or are even subject to the biases of maternal perceptions and recollections. It is worth mentioning, however, that the investigation of perceptions is indispensable to study subjective processes that lead to maternal feeding practices.29
The FFQ used in the study has not been previously validated, which makes it difficult to compare with other studies. However, its development was necessary, since a brief and specific tool was not available for the studied age group.
The use of a validated questionnaire to evaluate restrictive feeding practices in a significantly large sample is one of the strengths of this study, as well as the originality of the approach to this topic in the Brazilian population. Although there are few studies on parental feeding practices in Brazil, they are extremely relevant, as it represents a country where rates of childhood obesity have been growing alarmingly.16
To conclude, in this study, the mother's perception that her child is slightly fat/fat/very fat, concern about excess weight, the child's excess weight, and ultraprocessed food consumption were predictors of the use of maternal restriction practices to control the child's weight.
Restriction can be an alternative adopted by mothers as a simple method to promote healthy eating habits and control the child's weight. However, it can harm the child's physical and emotional health and should not be encouraged by professionals who seek to treat obesity.
It is important to consider that food restriction is a control and imposition strategy on the child's feeding, based on maternal goals and desires that do not consider the needs of the child. When exposed to this type of strategy, the child may interpret the mother's attitude in a contradictory manner. On one hand, attributing a negative and harmful connotation to the prohibited items, while on the other hand, understanding that such highly palatable foods, although prohibited, are extremely desirable. Consequently, when exposed to these foods, there is a greater risk of consuming them in large quantities even in the absence of hunger. It is therefore recommended that children learn in their family environment to consume all types of food in moderation, developing the critical knowledge that will enable them to make decisions about the adequate frequency and quantity for their consumption.
Supported by these data, intervention programs should be designed to help raise parents’ awareness of their children's nutritional status, while always being careful not to lead to harmful actions, but rather seeking to include advice that can result in a flexible environment in which children are encouraged to participate and make decisions about their own nutrition.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the participating schools, parents, and children for their contribution. They also would like to thank CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) for the grants to FRF, SW, LAM, and JFI, as well as CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) for the productivity grant to JAACT.
Please cite this article as: Freitas FR, Moraes DE, Warkentin S, Mais LA, Ivers JF, Taddei JA. Maternal restrictive feeding practices for child weight control and associated characteristics. J Pediatr (Rio J). 2019;95:201–8.
Study carried out at Universidade Federal de São Paulo (UNIFESP), Departamento de Pediatria, Disciplina de Nutrologia, São Paulo, SP, Brazil.




