
To identify the associated factors to loneliness among Brazilian adolescents, considering this is a knowledge gap and given its severity. The United Nations estimates that mental health problems affect approximately 20% of adolescents worldwide.
MethodsThis is a cross-sectional study with data from the National Adolescent School-based Health Survey 2015, conducted with students aged 13-17 in Brazil. The statistical analysis was performed with the calculation of the prevalence of feeling loneliness reported. Poisson regression with the adjusted Prevalence Ratio was used to evaluate the association between sociodemographic characteristics, family context, mental health and lifestyles, and feelings of loneliness.
Results15,5% of Brazilian students reported loneliness in the last 12 months. Female gender, higher maternal education, insomnia and be bullying victims rarely or sometimes and most of the time or always had a higher prevalence rate of loneliness. Having friends, having a meal with parents or guardians 5 days or more a week and having understanding parents showed a lower prevalence ratio for loneliness.
ConclusionLoneliness feeling is frequent among adolescents and is associated with female gender, less social and family support, intra-family violence and risk behaviors such as alcohol consumption and bullying. Policies to promote physical and mental well-being in this age group, stimulating friendship and family participation in the lives of adolescents should be made .
In recent decades, there has been an increase in the physical and mental illness of children and adolescents, while mental health problems afflict approximately 20% of the world's adolescents.1
Adolescence is characterized by a phase of intense transformations, thus there is great emotional instability, questioning, conflict and a greater need for the attention of public health policies directed to this age group.2
Therefore, mental health is an integral part of the health and well-being of young people and can be affected by biological, economic and cultural factors. Consequently, mental health in this age group requires greater investigation into the identification of risk factors and protection.3,4 Although, loneliness is experienced at all ages and from a variety of reasons and perspectives, while influenced by factors that reveal the human need to establish social relationships.5 Authors report an increase in the number of cases of depression, anxiety and eating disorders among young people, reaching about 20% of adolescents in the world.2,6
Data from the cohort study of 14-year-olds in the United Kingdom, the Millennium Cohort Study (n = 11,872), with a nationally representative sample survey, identified the prevalence of one-third (34.1%) loneliness among this age group, during the past 2 weeks in 2015. The study found that Loneliness was associated with negative social experiences, including bullying from peers and siblings and arguments with parents. It was also identified there was a constellation of adversities, including victimization and family conflict, that contributed to loneliness.7
In Brazil, an epidemiological survey found that 14.3% of school adolescents in a municipality in Rio de Janeiro have already thought about ending their own lives.6 Another study among about 4,207 adolescents aged 14 to 19 years in Pernambuco, found a feeling of loneliness in 15.8% of adolescents, suicidal thinking in 11.2%.4 However, there is a lack of studies and national surveys that address this issue.
Considering this to be a knowledge gap which no national Brazil survey was identified,4 being absent from academic and public discourse with a shortage of large-scale population data.7 In addition, given its severity and the need for investment in mental health studies, an investigation of mental health indicators among the adolescent population was carried out.4
This study aims to identify the factors associated with feelings of loneliness experienced by Brazilian adolescents, thereby contributing to the formulation of policies that promote an improvement in their mental health.
MethodThe analysis of demographic, family and social factors associated with loneliness was performed according to secondary data from the PeNSE 2015. PeNSE is a national cross-sectional survey in partnership with the Ministry of Health that provides information with updated data on the distribution of risk factors and health protection of Brazilian adolescents.8
The study investigated 10,926 Brazilian students enrolled and attending grades 6 to 9 of elementary school and grades 1 to 3, in 371 schools and 653 classes in the country's five geographic regions and the overall total for Brazil. This is a sample of schoolchildren aged 13 to 17 years, denominated Sample II.8
All the students in the selected classes present on the data collection day were invited to participate in the research. The sample analyzed comprised 50.3% male and 49.7% female students. Considering the students enrolled and non-respondents, the sample loss was approximately 2.4%. More details of the sample can be found in another publication.8
PeNSE data were collected between April and September 2015. The students, using smartphone devices, answered the structured self-administered questionnaire, contemplating information about the socio-economic situation, family context, experimentation and use of cigarettes, alcohol and other drugs, violence, safety, accidents, and other conditions concerning the life of these adolescents attending school.8 The elaboration of the questionnaire followed a methodology recommended by the Global School-based Student Health Survey (GSHS), developed by the World Health Organization (WHO).8
The outcome of feeling lonely was investigated by the question “In the last 12 months, how often have you felt lonely?”, categorized as: No (never, rarely or sometimes) and Yes (always and most of the time). The variables that characterize behavioral aspects of loneliness among the adolescents were categorized into four groups according to concept affinity, namely:
- a)
Sociodemographic characteristics: age (13 to 15 years and 16 to 17 years); gender; skin color (white, black, yellow, mulatto and indigenous); maternal schooling (none or incomplete elementary, complete elementary school or incomplete secondary school, complete or incomplete higher and complete higher); administrative dependency of the school (public or private);
- b)
Mental health: having friends, insomnia, suffering from bullying (never, rarely or sometimes and most of the time, always);
- c)
Behavior and life habits: tobacco use, alcohol consumption;
- d)
Family context: having a family meal on 5 days or more per week, having understanding parents, family supervision or frequency that parents or guardians really know what the child was doing in their free time; intrafamilial violence, or frequency that adolescents suffered physically aggression by an adult family member (never, once, and more than once).
A descriptive analysis was carried out with an assessment of prevalence and respective 95% confidence intervals (95% CI) for the outcome of feeling loneliness among adolescents, according to sociodemographic characteristics, family context, lifestyles, and mental health. Next, the Poisson regression was used with the calculation of the crude Prevalence Ratio (PRc).
The variables that were associated at level p < 0.02 were included in the multivariate Poisson regression model individually, obeying the increasing order of their p-value, or stepwise. Thus, all variables were mutually adjusted and the adjusted PR (PRa) for loneliness among adolescents was calculated. Only the variables that were statistically associated with loneliness among adolescents were retained in the final model (p < 0.05). Sampling structure and weights after stratification were considered for all analyses. The data were analyzed using Stata Statistical Software Release 13.
The students were informed about the research, their free participation and that they could withdraw if they did not feel comfortable about answering the questions. PeNSE is in compliance with the Guidelines and Norms Regulating Research Involving Human Beings and was approved by the National Commission of Ethics in Research of the Ministry of Health (CONEP/MS) under Certificate of Presentation for Ethical Appreciation (CAAE).8
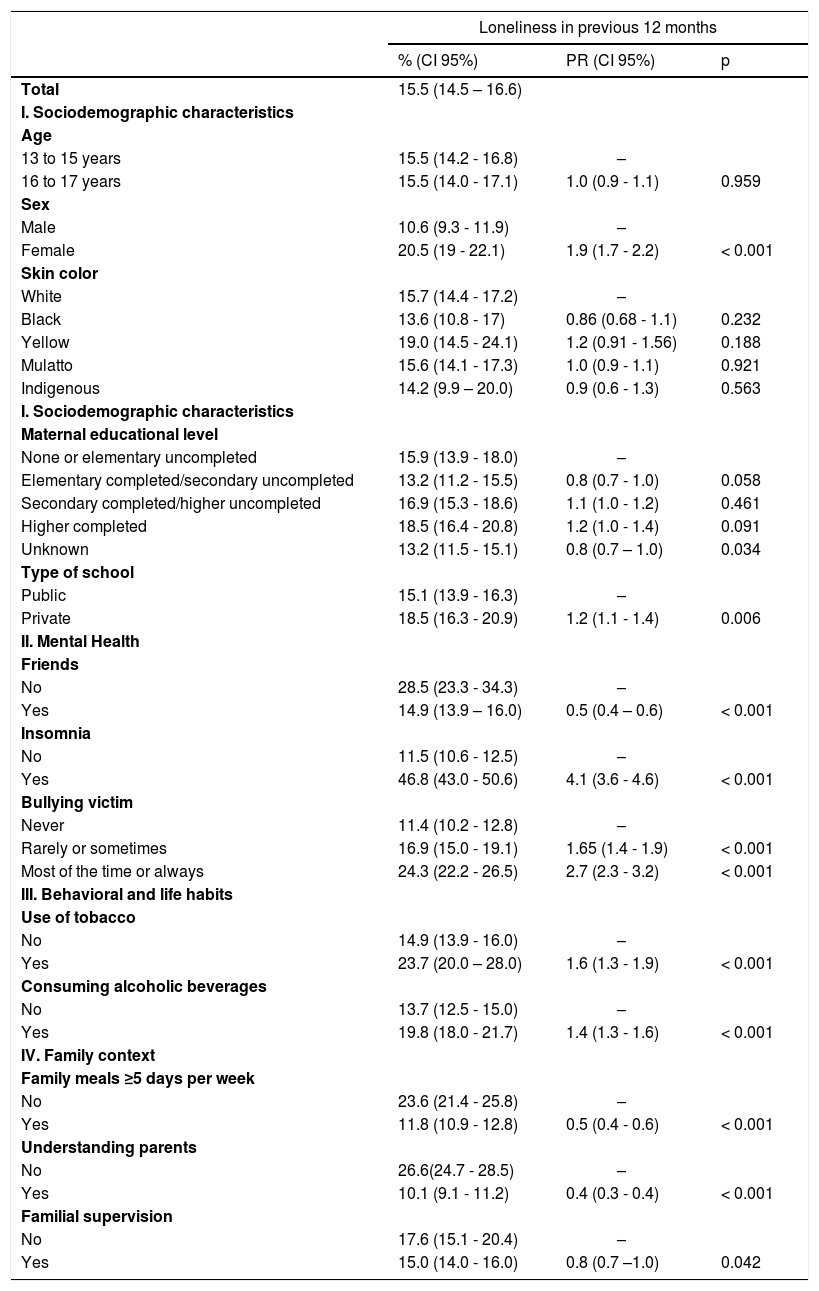
ResultsTable 1 shows that 15.5% (95% CI: 14.5–16.6) of Brazilian students reported feeling lonely in the last 12 months, with a higher frequency in females (20.5%, 95% CI: 19–22.1) and in private school students (18.5%, 95% CI: 16.3–20.9). There was a higher frequency of loneliness among adolescents who reported having insomnia (46.8%; 95% CI: 43–50.6) and who suffered bullying most of the time or always (24.3%; 95% CI: 22.2–26.5). Less prevalent were those who reported having friends 14.9% CI (13.9–16.0).
Prevalence and Gross Prevalence Ratio of loneliness among Brazilian adolescents aged 13 to 17 according to sociodemographic variables, family context, lifestyles and mental health, National School Health Survey (PeNSE), total for Brazil, 2015.
Notes: result weighted according to the complex sampling plan.
%, proportions and respective 95% confidence intervals (95% CI); PR, prevalence and respective 95% confidence intervals (95% CI); P, associated at level.
For the behavioral and life habits, there was a higher frequency of loneliness among adolescents who smoked cigarettes (23.7%; 95% CI: 20–28) and consumed alcoholic beverages (19.8%; 95% CI: 18–21.7) (Table 1). Regarding the family context, less loneliness was reported by those who had a family meal more than five days a week (11.8% CI 10.9–12.8)) and who had understanding parents (10.1% CI 9.1–11.2) (Table 1).
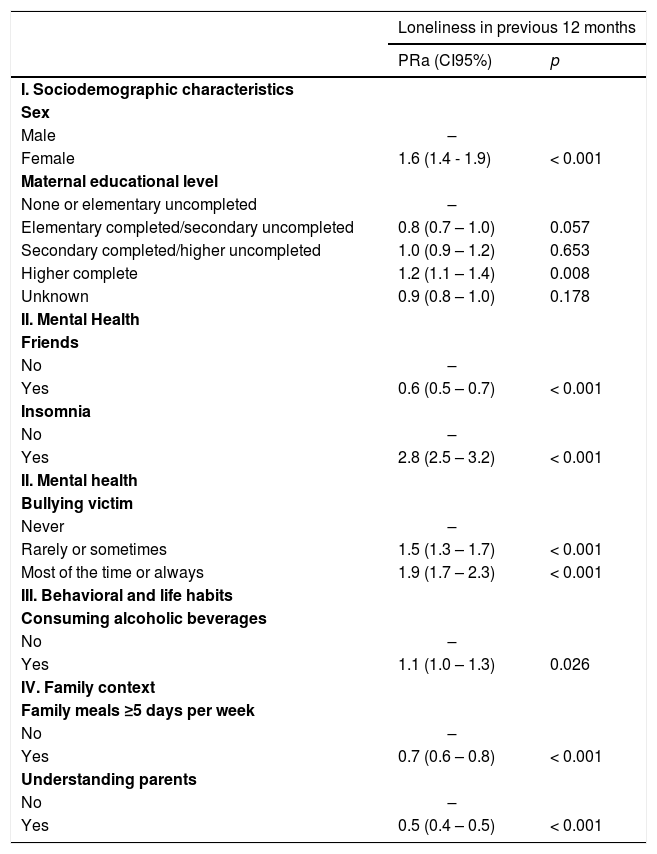
The sociodemographic variables that remained associated with feeling loneliness after adjustment in the Poisson multiple regression model (Table 2) were: female sex (PRa = 1.6, 95% CI: 1.4–1.9) and a higher completed maternal education level (PRa = 1.2, 95% CI: 1.1–1.4), who presented the greatest prevalence rate of feeling lonely in the 12 months prior to the survey. For the mental health characteristics investigated (Table 2), a higher prevalence of feeling loneliness was presented by those adolescents who reported insomnia (PRa = 2.8, 95% CI 2.5–3.2) and were victims of bullying rarely or sometimes (PRa = 1.5, 95% CI: 1.3–1.7) and most of the time or always (PRa = 1.9, 95% CI: 1.7–2.3).
Adjusted prevalence rate of loneliness among 13 to 17-year-old Brazilian adolescents according to sociodemographic variables, family context, lifestyles and mental health, National School Health Survey (PeNSE), Brazil, 2015.
Notes: result weighted according to the complex sampling plan.
PRa, adjusted prevalence ratio and respective 95% confidence intervals (95% CI); P, associated at level.
Among the behavioral and life habits investigated, alcohol consumption showed a higher prevalence rate among students who felt loneliness (PRa = 1.1, 95% CI 1.0–1.3). For the family context, behaviors such as having a meal with parents or guardians 5 days or more in the week (PRa = 0.7, 95% CI: 0.6–0.8) and having understanding parents (PRa = 0.5, CI 95%: 0.4–0.5) presented a lower aPR for loneliness among adolescents, as well as among those who reported having friends (PRa = 0.6, 95% CI 0.5–0.7) (Table 2).
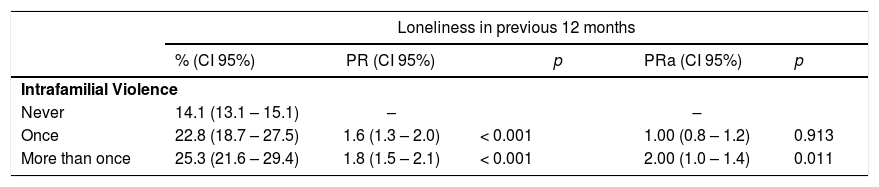
Table 3 shows that 22.8% (CI 95%: 18.7–27.5) of adolescents who reported intrafamilial violence once in the last 30 days felt loneliness in the 12 months prior to the survey, while 25.3% % (CI 95%: 21.6–29.4) of adolescents that suffered intrafamilial violence more than once felt loneliness. After Poisson multiple regression analysis and adjustment for variables related to sociodemographic characteristics, family context, lifestyles, and mental health, feelings of loneliness were higher among those adolescents who suffered more than one familial violence event (PRa = 2.0, 95% CI: 1.0–1.4), revealing a statistical relationship between intrafamilial violence and loneliness among adolescents (p < 0.05).
Gross and adjusted prevalence rate (PR and PRa) of loneliness among 13 to 17-year-old Brazilian adolescents according to episodes of intrafamilial violence, National School Health Survey (PeNSE), Brazil 2015.
Notes: result weighted according to complex sampling plan.
%, proportions and respective 95% confidence intervals (95% CI); PR, prevalence and respective 95% confidence intervals (95% CI); P, Associated at level; PRa, Adjusted prevalence ratio and respective 95% confidence intervals (95% CI).
The analyzes of data from the PeNSE 2015, shows that loneliness affects approximately one-seventh of the population of Brazilian schoolchildren, and this was associated with sociodemographic characteristics such as female sex, higher maternal education, insomnia, being a victim of bullying, use of cigarettes, and alcohol.
Countries such as Russia and the United States, when compared to Brazil, presented a lower prevalence of loneliness among adolescents. In Russia and the United States, one in ten adolescents reported feelings of loneliness, while in the Czech Republic this figure. is one in thirteen.9 It is a little researched topic that, due to its influence on the aggravation of mental health in adolescents, has been gaining magnitude in the incidence of disease or mental disorders among this population.6,9
Regarding the sociodemographic characteristics investigated in this study, gender showed a relation with loneliness, with a higher prevalence in females. Studies confirm that there is greater fragility in mental health and loneliness among women,4,5 presenting a higher prevalence of negative relationships between family and friends.10 Females are also more likely to contain their feelings and are more susceptible to suffering from problems such as depression and loneliness,11 self-inflicted injuries or suicide12 and find greater ease in recognizing themselves to be lonely and sad.4 Male adolescents, on the other hand, project their emotions more, becoming prone to suffer from the externalization of feelings, such as hyperactivity, conduct disorder and violence.11
There was also a significant association between loneliness and maternal schooling. Adolescent children of mothers with higher education revealed a higher prevalence of feeling alone, which can be explained by the influence of income in that, according to some authors, higher levels of schooling are associated with higher levels of loneliness among adults, after being adjusted for the covariables of income and sex.5 However, research conducted on adolescents from the Czech Republic, the United States and Russia revealed that parents with higher levels of schooling offer a better behavior model for their children, influencing less the feeling of loneliness among adolescents,9 this finding was contrary to the results of the current study. Furthermore, another study attributes the relationship between higher levels of loneliness and higher schooling to an improvement in the concepts of social relation and greater restrictions and requirements in establishing and maintaining personal relationships, thereby contributing to the distance between people.5 Thus, in order to better evaluate the effect of maternal schooling on loneliness among adolescents, further studies are needed that consider the income variable in the investigative model.
Insomnia was also related to loneliness among adolescents, in that those who reported greater difficulty sleeping had a higher prevalence of loneliness. A study conducted with Norwegian students indicates that feelings of loneliness were associated with reports of difficulty in initiating and maintaining sleep among the young, thereby impairing the quality of life and well-being of the population.13 In accordance with the results found in the present study, other authors showed a higher risk of insomnia among adolescents who suffered violence and loneliness.13,14 In the United States, insomnia symptoms reported by adolescents are associated with mental problems and suicidal tendencies, involvement with risk factors such as tobacco use, substance abuse, obesity, and a worse perception of their mental health.15 Thus, sleep disorders can be a triggering factor or a consequence of loneliness among adolescents, since it can impair their emotional state rendering them unable to cope with stressful situations, and reflects troubling experiences in the adolescent's daily life.13
The presence of friends continued to show a lower prevalence ratio among adolescents who reported loneliness. Such findings are consistent with the evidence of other studies in which authors affirm that in the younger age group, having friends maintains the social relation between adolescents, and it is also a form of support while faced with the changes experienced in this age group, thereby reducing feelings of loneliness.7,9,16 Thus, relations of friendship characterized by mutual support are reported to be a protective factor and offer social support against situations of anxiety and loneliness among adolescents, consequently improving well-being and reducing the levels of suffering caused by stress.10 Likewise, other studies confirm the protective role of friendships in health risk factors for adolescents, such as smoking tobacco and its derivatives and the use of illicit drugs17,18 while reducing the prevalence of bullying among school children.14,19
Peer violence or bullying has also been associated with intrafamilial violence and loneliness among adolescents. Authors affirm that bullying predisposes teenagers to conditions of vulnerability, such as: insomnia, low self-esteem, sadness, depressive symptoms, and high levels of suicidal ideation, as determined by personal, family, school, social and cultural factors.14 Adolescents who are victims of bullying present impaired interpersonal skills, and feel more lonely and greater shyness, thus demonstrating the relationship between bullying and loneliness in this age group.14,19-20
In the present study, a positive correlation was identified between alcohol consumption by adolescents and reports of loneliness. Psychoactive substances, because they are close to the school environment, can interfere with the daily life and social relations of adolescents, with alcoholic beverages and cigarettes being the main psychoactive substances used by schoolchildren.21
Research conducted with adolescents from Russia and the United States revealed that lonely adolescents present a higher consumption of psychoactive substances because they use alcoholic beverages as a means to alleviate negative feelings of loneliness and also to obtain approval from friends and favor social relationships.9 In Brazil, a study reveals the positive association between loneliness and increased consumption of substances such as alcohol and illicit drugs, in which those who had no friends made more use of alcoholic beverages.17,22 However, according to the WHO, drug use is an ineffective method to alleviate situations of loneliness and violence experienced by adolescents, contributing negatively to their physical and mental well-being.
In relation to cigarette smoking, authors have identified that living with parents in the same home environment reduces the chance of using this substance.21,23 On the other hand, conflicting relationships between fathers, mothers and children undermine the concept that the adolescent constructs about certain habits that are detrimental to health, thereby favoring risk behaviors such as smoking among adolescents.24
Parents with a harsh authoritarian style also contribute to increased levels of loneliness among adolescents,24 a finding that corroborates the results of this study in which more participatory parenting reduces the risk of feeling loneliness in this age group. Thus, parents who understand their children's problems and know what they do in their free time are contrary to the idea of authoritarian parents, who abuse disciplinary and coercive power and become aggressors against children and adolescents.25 Therefore, positive aspects of family support reveal the importance of parents in the promotion of children's mental health through increasing their self-confidence and social and family ties, improving their ability to resolve conflicts and investing in the prevention of risk behavior.2,26
According to results found in this study, the authors highlight a relationship between intrafamilial violence and the increase of mental disorders among the victims.27,28 Loneliness, combined with feelings of depression and anxiety, are symptoms of internalization and mental disorders resulting from family interactions based on conflict and violence, which can be minimized by supportive relationships between family members.28 This research also reveals the association between intrafamilial violence and harmful effects such as increased suicidal tendencies, traumatic experiences, psychosocial maladjustment, aggressive behavior, physical violence, self-esteem problems, anxiety, and sexual-risk taking.28 Thus, intrafamilial violence in adolescence, coupled with peer and community violence, contributes to the increase in mental suffering and feeling of loneliness, which is considered to be the cause of the increase seen in the frequency of mental disorders in this age group.2,3,6,29
This study reveals that loneliness is an aggravating factor that is becoming frequent in the daily life of adolescents, with a detrimental effect on their physical and mental health. It has been observed that social and structural resources to further harmonious family relations reduces loneliness and promote better conditions for the quality of life among adolescents. Therefore there is unquestionably a need to invest in health policies aimed at enhancing the physical and mental well-being of adolescents that take into account their specific needs and concerns. Attention should also be paid to those factors that contribute to the onset and aggravation of mental disorders among adolescents, including familial and school violence, alcohol consumption, and a lack of emotional support from family and friends.
For future studies, it is also necessary to investigate the influence of social networks on the family and social behavior of the adolescent, in order to estimate their relationship with loneliness among schoolchildren by including this theme in the PeNSE.
Since this is a cross-sectional study, the results have limitations concerning the attribution of causative factors, verification of which requires further investigation. In addition, the question incorporated in the PeNSE questionnaire on loneliness does not cover the topics of suicide, depression and other mental disorders among adolescents thereby making it difficult to investigate between mental health and loneliness among adolescents. Therefore, the presented results demonstrated the association between the investigated phenomena and adolescents characteristics, thus indicate the necessity to investigate the effects of age, maternal schooling, insomnia, and alcohol consumption on the mental health of adolescents through studies capable of inferring the causality of these factors.
FundingFundo Nacional de Saúde: TED 66/2018.




