



To analyze the occurrence of anemia and iron deficiency in children aged 1 to 5 years and the association of these events and retinol deficiency.
MethodsThis was an observational analytic cross-sectional study conducted in Vitoria, ES, Brazil, between April and August of 2008, with healthy children aged 1 to 5 years (n=692) that lived in areas covered by primary healthcare services. Sociodemographic and economic conditions, dietary intake (energy, protein, iron, and vitamin A ingestion), anthropometric data (body mass index-for-age and height-for-age), and biochemical parameters (ferritin, hemoglobin, and retinol serum) were collected.
ResultsThe prevalence of anemia, iron deficiency, and retinol deficiency was 15.7%, 28.1%, and 24.7%, respectively. Univariate analysis showed a higher prevalence of anemia (PR: 4.62, 95% CI: 3.36, 6.34, p<0.001) and iron deficiency (PR: 4.51, 95% CI: 3.30, 6.17, p<0.001) among children with retinol deficiency. The same results were obtained after adjusting for socioeconomic and demographic conditions, dietary intake, and anthropometric variables. There was a positive association between ferritin vs. retinol serum (r=0.597; p<0.001) and hemoglobin vs. retinol serum (r=0.770; p<0.001).
ConclusionsAnemia and iron deficiency were associated with low levels of serum retinol in children aged 1 to 5 years, and a positive correlation was verified between serum retinol and serum ferritin and hemoglobin levels. These results indicate the importance of initiatives encouraging the development of new treatments and further research regarding retinol deficiency.
Analisar a ocorrência de anemia e de deficiência de ferro em crianças de 1 a 5 anos e a associação destes desfechos com a deficiência de retinol.
MétodosTrata-se de um estudo observacional analítico do tipo transversal, realizado no município de Vitória – ES, entre abril e agosto de 2008, com crianças (n=692) saudáveis de 1 a 5 anos, residentes em áreas de abrangência de Unidades Básicas de Saúde. Foram avaliados dados sociodemográficos, econômicos, dietéticos (ingestão de energia, proteína, ferro e vitamina A), antropométricos (índice de massa corporal-por-idade e estatura-por-idade) e bioquímicos (níveis séricos de ferritina, hemoglobina e retinol).
ResultadosDetectou-se anemia, deficiência de ferro e deficiência de retinol em 15,7%, 28,1% e 24,7% das crianças, respectivamente. A análise univariada evidenciou maior ocorrência de anemia (RP: 4,62; IC 95%: 3,36; 6,34, p<0.001) e de deficiência de ferro (RP: 4,51; IC 95%: 3,30; 6,17, p<0.001) entre crianças que apresentavam deficiência de retinol. As mesmas relações se mantiveram após o ajuste pelas variáveis socioeconômicas, demográficas, dietéticas e antropométricas. Houve relação positiva entre os valores de ferritina sérica vs. retinol (r=0,597; p<0,001) e hemoglobina vs. retinol (r=0,770; p<0,001).
ConclusõesA anemia e a deficiência de ferro mostraram-se associadas com baixos níveis de retinol em crianças de 1 a 5 anos, e houve correlação positiva dos níveis de retinol com os de ferritina sérica e hemoglobina. Isto torna importante iniciativas que estimulem o desenvolvimento de novos tratamentos e a ampliação de pesquisas em relação à deficiência de retinol.
Iron is an essential nutrient for proper functioning of the body and is involved primarily in oxygen transport. Therefore, iron deficiency and, in more severe cases, anemia, affects every cell of a living organism, impairing behavior, cognitive performance, physical growth, and immunity.1,2
Anemia is one of the main deficiency diseases in the world and is characterized as a severe public health problem. The World Health Organization (WHO) estimates that anemia primarily affects 1.62 billion people worldwide and that the occurrence of iron deficiency is 2.5-fold higher.2 In Brazil, anemia is observed in all age groups in different regions of the country, regardless of income or nutritional status.1 In 2006, the National Demographic and Health Survey (Pesquisa Nacional de Demografia e Saúde - PNDS) showed a 20.9% prevalence of this disease in children younger than 60 months.3
The different consequences of anemia and iron deficiency, alongside the difficulties in their control and treatment, encourage the study of the reasons for their high prevalence and potential risk factors, aiming at directing public policies.2,4 To date, intervention programs that include prevention and treatment of iron deficiency diseases through drug supplementation and food fortification do not appear to be effective or sufficient for reversing the epidemiological picture of these problems, considering the high prevalence observed. The failure of these programs can be associated with the complexity of other factors involved in the development of anemia, among them, retinol deficiency.4,5
Low levels of retinol lead to vitamin A deficiency, which affects 140 million children under 5 years of age worldwide, 127 million at preschool age alone.6,7 Several epidemiological studies show a significant association between retinol deficiency and the occurrence of anemia.
Mariath et al.,8 for instance, demonstrated an association between nutritional status of retinol and serum iron in children up to 10 years in Santa Catarina. A study conducted with Brazilian preschoolers showed an association between serum hemoglobin and retinol levels.9
It is believed that retinol deficiency reduces the availability of iron stores from macrophages and the liver to erythropoiesis and, consequently, to the synthesis of hemoglobin. Some studies indicate that this ratio is related to an increased expression of hepcidin, a liver hormone that regulates the availability of iron storage. High concentrations of hepcidin imply that there is an internalization and lysosomal degradation of ferroportins, transmembrane proteins that allow transport of iron into the blood stream. As there is no available circulating iron, red cell production is impaired, leading to anemia. However, this metabolic process is still hypothetical, with no clear conclusions yet.10,11
Considering the above, this study aimed to analyze the occurrence of anemia and iron deficiency in children between 1 and 5 years of age and the association of these outcomes with retinol deficiency. It is expected to contribute to public health programs concerning the prevention and treatment of iron deficiency and anemia.
MethodsThis was an analytical observational cross-sectional study, conducted in Vitória, ES, Brazil, with children aged between 1 and 5 years, in the months of April to August of 2008. Mobilization for data collection was carried out by community health agents (CHAs), who invited the parents or legal guardians of children in that age group to present at the Basic Health Unit (BHU) in the area where they resided. Only children who came to the BHU on the scheduled date were included in the study.
The city of Vitoria is divided into eight administrative regions - Jardim Camburí, Maruípe, São Pedro, Santo Antônio, Jucutuquara/Bento Ferreira, Continental, Praia do Canto, and Centro - which, in turn, are divided into 28 healthcare areas, each represented by a BHU. The population of children aged 1 to 5 years in the municipality is estimated at 26,967.12 Based on this information and assuming a prevalence of anemia of 37.3%,13 an α error of 5%, and a power of 95% of the test, the sample size calculation was performed,14 which established a minimum of 395 children for the study, distributed proportionately among the administrative regions. This number was reached for almost all regions of the county, except for Praia do Canto (estimated sample size: 42; achieved sample size: 23) and Jardim Camburi (estimated sample size: 33; achieved sample size: 26).
The children included in the study were apparently healthy as perceived by parents or guardians and general clinical evaluation. Data collection was performed at BHU by trained nutritionists, undergraduate students of Nutrition, and technical nursing staff. The children were accompanied by their parents or guardians. A structured questionnaire was applied, which included sociodemographic, economic, and dietary data. Subsequently, the anthropometric and biochemical assessment of the children was performed.
Among the sociodemographic and economic data, the child's age, premature birth, gender, maternal age, number of people in family, and social class were evaluated. A child was considered premature if he/she had been born after less than 37 gestational weeks (GW); borderline premature, between 37 and 38; and full-term, after 38 GW. For assessment of social class, a questionnaire adapted from the 2000 Census was used,15 consisting of a list of ten consumer goods and information on the education level of the household head. These items were scored according to the recommendations of the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística - IBGE) and it allowed for the classification of the children into social strata.15
Dietary intake was assessed using a semiquantitative Food Frequency Questionnaire (FFQ), created exclusively for the study and not validated, consisting of 62 foods representing seven food groups (cereals, tubers, roots and derivatives; legumes; fruits and natural fruit juices; vegetables; milk and dairy; meat and eggs; oils, fats and oilseeds) from the “Food Guide for the Brazilian population”.16 This questionnaire included the amount of food consumed in household measures and frequency of consumption (daily, weekly, fortnightly, monthly, rarely, or never/nonexistent).
Dietary frequency data were transformed into daily consumption amount, according to the methodology proposed by Costa et al.17 Foods marked as “daily” frequency were quantified according to reported household measure; for foods classified as “rare” or “never/nonexistent”, consumption was assigned zero value; and for those that had weekly, fortnightly, or monthly consumption, the amount was divided by seven, fifteen or thirty, respectively.17
The analysis of food intake data was performed with the aid of DietWin Nutrition® program, professional version 2008 (DietWin softwares, Rio Grande do Sul, Brazil), which allowed for the calculation of the ingested daily calories, as well as dietary data on protein, iron, and vitamin A. The first variable was categorized into<1,500kcal, between 1,500kcal and 3,000kcal, and ≥ 3,000kcal. Protein intake was classified as adequate, inadequate, and excessive, according to the criteria of the Institute of Medicine (IOM).18
Micronutrient intake was qualitatively assessed18 as: intake below the estimated average requirement (EAR), intake between the EAR and recommended dietary allowances (RDA), and intake higher than the RDA.
EAR is characterized as the mean daily nutrient intake estimated to meet the needs of 50% of healthy individuals, and RDA represents the amount of nutrients sufficient to meet the needs of approximately 97% to 98% of healthy individuals.18
Anthropometric assessment included weight and height measurements, conducted as recommended by the Food and Nutrition Surveillance System (Sistema de Vigilância Alimentar e Nutricional – SISVAN).19 Based on these measurements, the height-for-age and the body mass index (BMI)-for-age values were obtained using the WHO growth curves,20 assessed according to the cutoffs proposed by the Brazilian Ministry of Health.19 It should be emphasized that individuals classified as at risk for overweight were considered as normal weight in this study.
Biochemical evaluation consisted in investigating the nutritional iron status, with measurement of serum ferritin, hemoglobin, and retinol. For this purpose, 3 mL of blood were collected by nursing technicians.
Ferritin was measured by chemiluminescent immunometric assay and using the Inmulite® (Siemens, Erlangen, Germany) device in a specific lab of the Faculdade Salesiana de Vitória. Iron storage depletion was defined when ferritin concentrations were<12μg/L.21
Regarding the assessment of hemoglobin levels, approximately 30μL of collected blood were placed in a disposable micro test tube to undergo reading at HemoCue® portable photometry system (Hemocue, Ängelholm, Sweden). Anemia was considered when hemoglobin values were<11.0g/dL21 and when iron depletion was confirmed by assessment of serum ferritin levels.1
Serum retinol levels were classified according to the Brazilian Society of Pediatrics; vitamin A levels<0.70 mmol/L were considered low.22 Theis measurement was performed using the spectrophotometric method in a specific laboratory.
It is noteworthy that all children were assessed regarding the use of nutritional supplements.
All data were tabulated in Excel® (Microsoft Excel, Washington, USA) spreadsheets and their internal consistency was assessed. Descriptive analysis included variable categorization and frequency distributions. The inferential analysis was performed using Poisson regression with robust variance and Spearman's correlation. The final adjustment of the multivariate Poisson regression model was performed using the goodness-of-fit test.
Variables related to iron nutritional status were considered as dependent variables, serum retinol deficiency as an independent variable, and the variables related to sociodemographic and economic status, food consumption, and nutritional status as adjustment variables. Statistical analyses were performed using SPSS version 17.0 (SPSS Statistics for Windows, Version 17.0, Chicago, USA) and STATA 11.0 (Stata Statistical Software: College Station, TX: StataCorp LP), with a significance level of 5% (p<0.05).
The children's parents or guardians signed an informed consent after being informed on the study objectives and measurements. It is noteworthy that children diagnosed with anemia during the study were referred for treatment at the BHU nearest to their residence. The study was approved by the Research Ethics Committee of the Faculdade Salesiana de Vitória and met the ethical recommendations of Resolution 466/2012 of the Brazilian National Health Council
ResultsThe sample (n=692) was homogeneous regarding gender (52.3% of girls) and consisted mostly of children aged between 24 and 48 months (53%).
Stature deficit and overweight were observed in 7.4% and 22.9% of the children. Social classes C (45.9%) and D+E (46.5%) were the most common (Table 1).
Sociodemographic, economic, and anthropometric characteristics of the study population.
| Variable | n | Frequency (%) |
|---|---|---|
| Age in months | ||
| 12- 24 | 154 | 22.3 |
| 24 - 48 | 367 | 53.0 |
| 48 - 60 | 171 | 24.7 |
| Gender | ||
| Female | 362 | 52.3 |
| Male | 330 | 47.7 |
| Prematurity | ||
| Full-term (> 38 GW) | 609 | 88.0 |
| Borderline prematurity (37 to 38 GW) | 48 | 6.9 |
| Prematurity (< 37 GW) | 35 | 5.1 |
| Height-for-age classificationa | ||
| Low | 51 | 7.4 |
| Adequate | 639 | 92.6 |
| BMI-for-age classificationb | ||
| Thinness | 22 | 3.2 |
| Normal weight | 509 | 73.9 |
| Overweight | 144 | 20.9 |
| Obesity | 14 | 2.0 |
| Maternal age | ||
| Adolescent | 37 | 5.9 |
| Adult | 591 | 94.1 |
| Number of family members | ||
| 0 - 4 | 343 | 50.4 |
| > 4 | 338 | 49.6 |
| Social class | ||
| A+B | 52 | 7.6 |
| C | 317 | 45.9 |
| D+E | 321 | 46.5 |
GW, gestational weeks; BMI, body mass index.
Anemia, iron deficiency, and retinol deficiency were detected in 15.7%, 28.1%, and 24.7% of the children, respectively. Dietary iron intake was below the EAR in 14.9% of the sample and 83.4% of the children had vitamin A ingestion above the RDA (Table 2).
Health and dietary characteristics of the study population.
| Variable | n | Frequency (%) |
|---|---|---|
| Use of supplements | ||
| No | 538 | 81.9 |
| Ferrous sulphate | 73 | 11.1 |
| Multivitamin | 33 | 5.0 |
| Others | 13 | 2.0 |
| Anemia | ||
| Yes | 104 | 15.7 |
| No | 557 | 84.3 |
| Iron deficiency | ||
| Yes | 105 | 28.1 |
| No | 269 | 71.9 |
| Retinol deficiency | ||
| Yes | 92 | 24.7 |
| No | 281 | 75.3 |
| Dietary intake of energy | ||
| <1,500 kcal | 214 | 46.0 |
| 1,500 - 3,000kcal | 223 | 48.0 |
| ≥ 3,000 kcal | 28 | 6.0 |
| Dietary intake of protein | ||
| Insufficient | 1 | 0.2 |
| Adequate | 321 | 69.0 |
| Excessive | 143 | 30.8 |
| Dietary intake of iron | ||
| <EAR | 72 | 14.9 |
| ≥ EAR ≤ RDA | 281 | 57.9 |
| > RDA | 132 | 27.2 |
| Dietary intake of vitamin A | ||
| <EAR | 55 | 11.3 |
| ≥ EAR ≤ RDA | 26 | 5.3 |
| > RDA | 406 | 83.4 |
EAR, estimated average requirements; RDA, recommended dietary allowances intakes.
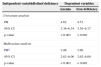
The univariate analysis showed a higher incidence of anemia (OR: 4.62, 95% CI: 3.36-6.34) and iron deficiency (OR: 4.51, 95% CI: 3.30, 6.17) in children who had retinol deficiency (Table 3).
Association of anemia and iron deficiency with retinol deficiency in the study population.
| Independent variableRetinol deficiency | Dependent variables | |
|---|---|---|
| Anemia | Iron deficiency | |
| Univariate analysis | ||
| PR | 4.62 | 4.51 |
| 95% CI | 3.36–6.34 | 3.30–6.17 |
| p-value | <0.001 | <0.001 |
| Multivariate analysis | ||
| PRa | 3.96 | 3.96 |
| 95% CI | 2.62–6.00 | 2.62–6.00 |
| p-value | <0.001 | <0.001 |
PR, prevalence ratio; CI, confidence interval.
Coefficients adjusted for sociodemographic, economic, anthropometric, and dietary variables. Adjusted value of p > 1.00.
Obs: Poisson regression coefficient with robust variance with iron deficiency anemia (hemoglobin+ferritin) and iron deficiency (ferritin) as dependent variables and serum retinol (mmol/L) as the independent variable.
Spearman's correlation showed a moderately positive association between serum ferritin vs. retinol (r=0.597; p<0.001) and a strong positive association between hemoglobin vs. retinol (r=0.770; p<0.001) (Fig. 1).
 with serum ferritin (μ/L) and hemoglobin (g/dL).")
After adjusting for sociodemographic, economic, anthropometric, and dietary variables, the influence of serum retinol deficiency on anemia and iron deficiency remained. The prevalence of anemia and iron deficiency among children with retinol deficiency was 3.96-fold (95% CI: 2.62-6.00) higher when compared to those who did not have an altered nutritional status of retinol (Table 3).
DiscussionThis study investigated the occurrence of anemia and iron deficiency and its association with retinol levels in children aged 1 to 5 years in Vitória, ES, Brazil. The results indicated a positive association of serum retinol deficiency with anemia and iron deficiency, regardless of sociodemographic, economic, anthropometric, and dietary variables.
Anemia and iron deficiency were found in 15.7% and 28.1% of children, respectively.
Prevalence studies in Brazil exhibit a great variation in relation to these data. Cardoso et al.23 found 10.3% of anemia and 45.4% of iron deficiency in children aged 6 months to 10 years in the Amazon region. In Rio Grande do Sul, the findings were 58.8% and 90.3%, respectively, in children aged 12 to 16 months.24 Mariath et al.8 observed a prevalence of 16.7% of iron deficiency in children up to 10 years in Itajaí, SC. These discrepancies are justifiable considering the different definitions of anemia and iron deficiency adopted in the studies, as well as the multiple factors that explain the occurrence of these outcomes, such as the child's age, maternal education, family income, and anthropometric indicators, among others.4
The prevalence of retinol deficiency was 24.7%. Similarly to the occurrence of anemia, retinol deficiency has great amplitude in the literature. Netto et al.,25 in a study of children in the state of Paraíba, observed a prevalence of 39.6% of vitamin A deficiency, while Cardoso et al.23 detected 14.2% in the Amazon region. The variations found between studies are mainly due to whether this deficiency is endemic in the region, as well as the socioeconomic status of the sample.4,25
It is worth mentioning that since the study population was predominantly formed by social classes C, D, and E, higher prevalence of anemia and deficiencies of ferritin and retinol were expected. This is due to the fact that the low socioeconomic status has a negative impact on food consumption, housing conditions, and children's health.1
The positive association found between retinol deficiency and the occurrence of anemia and iron deficiency corroborates the findings of experimental and epidemiological studies. It is believed that the altered nutritional status of vitamin A does not interfere with iron absorption process, but with its mobilization in the liver.9,26 Citelli et al.,11 in experiments with mice and cell cultures, found an association between levels of vitamin A and the transcription factors of protein genes related to iron bioavailability. The results demonstrated that serum retinol deficiency increased hepcidin expression and directly affected hepatic mobilization of the iron storage required for erythropoiesis. The same results were found in epidemiological assessments.8,23,27
Since the association of these two minerals has been confirmed, when analyzing the evolution of anemia and iron deficiency in children, it is possible to observe that the prevalence remained high even with the progress of medicine. It is currently know that the drug treatment used for the reversal of this picture has a positive impact on children's health; however, this treatment alone cannot solve the public health problem of anemia and iron deficiency. The reasons include the low adherence to treatment or abandonment caused by the different side effects of the iron supplement,28,29 or by the influence of other factors, such as vitamin A deficiency.
Some studies have demonstrated that iron supplementation concomitant with vitamin A supplementation significantly reduced anemia;7 the finding persisted even with the isolated supply of vitamin A.26 It is believed that this supplementation can improve iron metabolism, suppress the infectious process, stimulate the synthesis of transferrin, and exert positive effect on the elevation of iron blood levels.9,10 Thus, progress in the treatment of iron deficiency may improve the iron status of children in Brazil.
One limitation of the present study was its cross-sectional design, which prevents the understanding of cause-and-effect association. Moreover, the sample was not representative of the municipality of Vitória and consisted only of children that came to the BHU on the scheduled date for data collection. Although these characteristics limit the extrapolation of data, the strength and significance of the associations obtained, which remained after adjusting for potential confounders, indicate that the findings are real.
The study also failed by not excluding hemoglobinopathies, which could have been mistaken for anemia, and for not carrying out the control with CRP (C-reactive protein) for detection of non-apparent infections, which may have caused an overestimation of the anemia prevalence. Finally, a FFQ validated in the literature was not used. However, the questionnaire has been designed considering the main foods in the Food Guide for the Brazilian Population16 and, therefore, it is expected to have contemplated the food items consumed by the study population.
Based on the present results, it can be concluded that anemia and iron deficiency were associated with low levels of retinol in children aged 1to 5 years and there was a positive correlation between levels of retinol with serum ferritin and hemoglobin. These findings make it important to establish initiatives that stimulate the development of new treatments and further research on retinol deficiency in order to help reduce long-term hematological problems related to iron deficiency.
FundingFundação de Apoio à Ciência e Tecnologia do Espírito Santo (FAPES).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Saraiva BC, Soares MC, Santos LC, Pereira SC, Horta PM. Iron deficiency and anemia are associated with low retinol levels in children aged 1 to 5 years. J Pediatr (Rio J). 2014;90:593–9.
Study conducted at the Department of Nutrition, School of Nursing, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil.





