
To identify health-related quality of life in adolescents with excess weight and associated factors, such as gender, age, and weight categories.
MethodA cross-sectional study with collected and secondary data from 276 adolescents aged between 10 and 19 years with overweight and obesity, and whose parents or guardians authorized their participation. Anthropometric data, pubertal development, and the PedsQL 4.0 questionnaire were collected for the health-related quality of life assessment. Categorical data were described as numbers and percentages. For the description of health-related quality of life subscales, medians and the 25th and 75th percentiles were used, as well as the Mann–Whitney test for comparisons between age group, gender, and weight categories.
ResultsThe median health-related quality of life total score was 78.3 (68.5–87.4). The lowest scale was the “emotional score”, 65 (50–80). Higher health-related quality of life was found in boys in most of the scores (p<0.05), except for the “school score” (p=0.09). Regarding the age group, the median of the “physical scores” (p=0.03) and “social score” (p=0.02) were significantly lower in the group younger than 14 years. When separated according to weight categories, it was verified that obese adolescents differed significantly in relation to the “physical score” (p=0.00), “school score” (p=0.04), and “total score” (p=0.02) of the health-related quality of life. However, there was no significant difference between the emotional, social, and psychosocial scores.
ConclusionsAdolescents with overweight and obesity show losses in the health-related quality of life and also between the different domains, when separated by age, gender, and weight categories.
Identificar a qualidade de vida relacionada à saúde entre adolescentes com excesso de peso e fatores associados, como gênero, idade e categorias de peso.
MétodoEstudo transversal com dados coletados e secundários de 276 adolescentes entre 10 e 19 anos, com sobrepeso e obesidade, cujos responsáveis autorizaram a participação. Foram coletados dados antropométricos, desenvolvimento puberal e questionário PedsQL 4.0 para a avaliação da qualidade de vida relacionada à saúde. Os dados categóricos foram descritos por contagens e percentuais. Para a descrição das subescalas da qualidade de vida relacionada à saúde foram usadas medianas e percentis 25 e 75 e teste de Mann-Whitney para comparações entre grupos de faixa etária, gênero e categorias de peso.
ResultadosA mediana do escore total da qualidade de vida relacionada à saúde foi de 78,3 (68,5-87,4). A menor escala foi o “escore emocional” 65 (50-80). Encontramos a qualidade de vida relacionada à saúde maior nos meninos na maioria dos escores (p<0,05), exceto o “escore escolar” (p=0,09). Quanto à faixa etária, a mediana dos “escores físico” (p=0,03) e “escore social” (p=0,02) foram significativamente menores no grupo menor de 14 anos. Ao separar as categorias de peso, percebe-se que os adolescentes obesos diferem significativamente com relação ao “escore físico” (p=0,00); “escore escolar” (p=0,04) e “escore total” (p=0,02) da qualidade de vida relacionada à saúde. Contudo, não houve diferença significativa entre os escores emocional, social e psicossocial.
ConclusõesAdolescentes com sobrepeso e obesidade têm prejuízos na qualidade de vida relacionada à saúde e também entre os diferentes domínios, quando separados por faixa etária, gênero e categorias de peso.
The definition of Health-Related Quality of Life (HRQoL) by the World Health Organization (WHO) is multidimensional, in which there are three main health dimensions (physical, psychological, and social) that can be used as a general health outcome measure.1
The prevalence of excess weight in southern Brazil is 28.2% in adolescents aged 13–17 years, whereas the prevalence of obesity is 10.2%, higher than the prevalence found in other regions of the country.2 It is known that children and adolescents with excess weight at this stage of life may remain with excess weight in adult life. A recent projection for the age group between 2 and 19 years shows that most young people today will be obese by the age of 35 years. In 2 year-old children, the prevalence of obesity increased until adolescence, when it stabilized, but continued to increase after adolescence.3
The concern with excess weight extends beyond the physiological conditions, since it has shown to be an interference factor for an adequate HRQoL in adolescents.4,5 Therefore, identifying and studying adolescents with excess weight is important to prevent negative effects on HRQoL, which may extend into different dimensions of life.6,7 In this context, the aim of the present study was to identify the HRQoL in adolescents with excess weight and to verify probable associated factors such as age, gender, and weight categories.
MethodsThis was a cross-sectional, descriptive study of primary data from overweight and obese adolescents of both genders, attending elementary school in the municipality of Cachoeira do Sul (CS), state of Rio Grande do Sul (RS), Brazil, and data obtained from another database from adolescents with overweight and obesity of both genders, attending elementary schools in the municipality of Santa Cruz do Sul – RS (SCS). The participating schools were located in the central region and were representative of the respective municipalities.
Inclusion and exclusion criteriaThe inclusion criteria considered overweight and obese students who were regularly enrolled in the schools involved in the project, aged between 10 and 17 years old, in the case of the SCS group. For the CS group, the enrolled students were in the 6th and 7th grades of a public elementary school, with ages ranging from 9 to 18 years old and who were overweight and obese. For both CS and SCS groups, those who agreed to and signed the Term of Assent (TA) and whose parents and/or guardians residing in the same household signed the informed consent were included in the study.
The exclusion criteria were the same for the SC and SCS students and those without the physical conditions to undergo the anthropometric evaluation, such as wheelchair users, those with amputated limbs or with a cast, pregnant adolescents, and students without the mental conditions and/or those unable to complete the questionnaires were excluded.
The sample was obtained by convenience, and considering a 95% Confidence Interval, margin of error of 3.5, and standard deviation of 18.0,8 reached a sample size of 105 adolescents with overweight, and with a 95% Confidence Interval, margin of error of 3.5, and standard deviation of 20.1, a sample size of 130 obese adolescents was obtained.
Data collectionRegarding the primary data, the students who agreed to participate and signed the TA and had parents and/or guardians who signed the informed consent were submitted to anthropometric measurements (weight, height, and waist circumference [WC]) by the researcher, as well as self-evaluation of Pubertal Stage (PS) and Pediatric Quality of Life Inventory 4.0 (PedsQL 4.0) for the assessment of QoL. Data on age and date of birth were supplied by the school. Data collection took place in 2016, with 3 month duration, during which data were collected from 72 students.
Data from a database of the project “Obesidade em adolescentes da educação básica: um estudo de intervenção interdisciplinar – Fase III” (“Obesity in Elementary School adolescents: an interdisciplinary intervention study – Phase III”) carried out in SCS were collected from an initially cross-sectional database of 25 schools, of which students had the signed the TA and the informed consent. The schools were similar regarding the sociodemographic characteristics. The measurements were carried out at Universidade de Santa Cruz do Sul (UNISC) by a trained team. The study was performed between 2015 and 2016, when data were collected from 285 adolescents. Data such as weight, height, age, skin color, WC, PS, and PedsQL were obtained from adolescents with overweight and obesity.
Tools and measuresNutritional statusThe following data were collected: age reported by the school, weight (kg), and height (cm). The weight and height measurements were used to calculate Body Mass Index (BMI) (weight [kg]/height [m2]). The adolescents were classified as having excess weight (overweight or obesity) based on the BMI/age expressed in z-score, calculated using the software WHO-Anthro Plus 2007 (World Health Organization), and following the recommendations proposed by the WHO.9 The WC was measured at midpoint between the last rib and the iliac crest. This study followed the cutoff points that identify abdominal obesity when WC is greater than the 90th percentile.10
Pubertal stageTo verify the PS, the self-assessment questionnaire according to Tanner criteria11 was applied at the same time of the anthropometric evaluation. The adolescent was placed in a private space to prevent embarrassment. The adolescents’ self-evaluation was carried out through illustrative images.
Quality of lifeThe generic questionnaire was applied – PedsQL 4.0 – validated for the Brazilian population, with four subscales, containing 23 items comprising: (1) physical dimension, (2) emotional dimension, (3) social dimension, and (4) school dimension.7
The analysis of the PedsQL 4.0 responses was performed as follows: they were inversely scored and linearly transposed to a scale of 0–100 (never=0=100 points, almost never=1=75 points, sometimes=2=50 points, many times=3=25 points, almost always=4=0 points); thus, the higher the score, the better the HRQoL.7
A psychosocial summary score was created, which demonstrates the student's psychosocial health through the mean of the sum of the items: social dimension, emotional dimension, and school dimension.
In the presence of missing data, the scale scores were considered as the sum of items divided by the number of answered items. However, when more than 50% of the scale items were absent, the scale score was not recorded. The consistency of this computation is similar to that of other publications that use the PedsQL as a reference, as well as other established HRQoL measurements.7
Statistical analysisCategorical data were described as counts and percentages, for variables such as municipality, gender, WC, and BMI classification. Age was described by mean and standard deviation (m±SD). The normality of distribution was verified for all continuous variables using the Kolmogorov–Smirnov test. When the sample did not show a normal distribution, median and 25th and 75th percentiles were used to describe the QoL subscales. The comparisons between age groups, gender, and weight category were performed using the Mann–Whitney test. The data were analyzed using IBM SPSS software (IBM SPSS Statistics for Windows, Version 20.0. NY, USA).
Ethical aspectsThe initial project in SCS already had approval of the Research Ethical Committee of UNISC, under CAAE no. 54985316.0.0000.5343 and Opinion no. 1.498.330. The study was submitted to the Research Ethics Committee of Universidade Federal do Rio Grande do Sul (UFRGS) to obtain approval for the use of the data collected in the municipality of CS, concomitantly to the SCS data, approved under CAAE no. 71390416.1.0000.5347 and Opinion no. 2.395.088, which followed all the ethical principles recommended by Resolution 466/12 of the National Health Council.
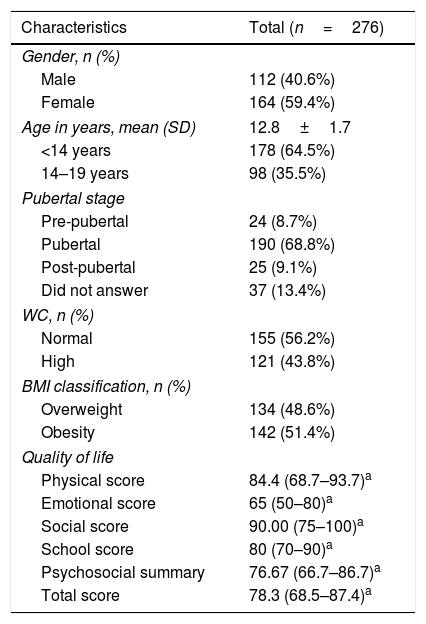
ResultsData were collected from 298 adolescents. Due to incomplete data, 22 adolescents were excluded. The study included 276 adolescents with excess weight, that is, with overweight (n=134) and obesity (n=142). The mean age was 12.8 years, ranging from 9 to 18 years. Most adolescents had normal abdominal adiposity (Table 1). The median of the total HRQoL score was 78.3 (68.5–87.4) for the adolescents. The lowest scale was the “emotional score”, with a result of 65 (50–80).
Characteristics of the adolescents participating in the study.
| Characteristics | Total (n=276) |
|---|---|
| Gender, n (%) | |
| Male | 112 (40.6%) |
| Female | 164 (59.4%) |
| Age in years, mean (SD) | 12.8±1.7 |
| <14 years | 178 (64.5%) |
| 14–19 years | 98 (35.5%) |
| Pubertal stage | |
| Pre-pubertal | 24 (8.7%) |
| Pubertal | 190 (68.8%) |
| Post-pubertal | 25 (9.1%) |
| Did not answer | 37 (13.4%) |
| WC, n (%) | |
| Normal | 155 (56.2%) |
| High | 121 (43.8%) |
| BMI classification, n (%) | |
| Overweight | 134 (48.6%) |
| Obesity | 142 (51.4%) |
| Quality of life | |
| Physical score | 84.4 (68.7–93.7)a |
| Emotional score | 65 (50–80)a |
| Social score | 90.00 (75–100)a |
| School score | 80 (70–90)a |
| Psychosocial summary | 76.67 (66.7–86.7)a |
| Total score | 78.3 (68.5–87.4)a |
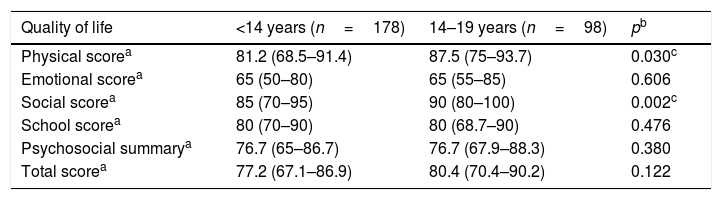
The effect of the age group on the PedsQL subscale scores was analyzed. The median of the “physical score” (p=0.03) and “social score” (p=0.02) were significantly lower in the age group younger than 14 years, compared to adolescents aged 14–19 years. However, there was no difference between the medians of the emotional, school, psychosocial summary, and total scores (Table 2).
PedsQL subscale scores of groups of adolescents younger than 14 years and between 14 and 19 years old.
| Quality of life | <14 years (n=178) | 14–19 years (n=98) | pb |
|---|---|---|---|
| Physical scorea | 81.2 (68.5–91.4) | 87.5 (75–93.7) | 0.030c |
| Emotional scorea | 65 (50–80) | 65 (55–85) | 0.606 |
| Social scorea | 85 (70–95) | 90 (80–100) | 0.002c |
| School scorea | 80 (70–90) | 80 (68.7–90) | 0.476 |
| Psychosocial summarya | 76.7 (65–86.7) | 76.7 (67.9–88.3) | 0.380 |
| Total scorea | 77.2 (67.1–86.9) | 80.4 (70.4–90.2) | 0.122 |
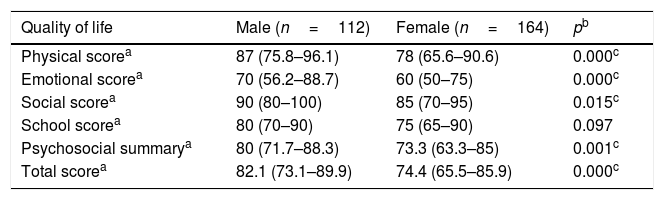
Table 3 highlights the comparisons between male and female adolescents. When analyzing the HRQoL in the different groups, a statistically significant difference was observed, since the HRQoL median was higher in boys in all scores (p<0.05), except for the “school score” (p=0.09).
PedsQL subscale scores and adolescents’ gender.
| Quality of life | Male (n=112) | Female (n=164) | pb |
|---|---|---|---|
| Physical scorea | 87 (75.8–96.1) | 78 (65.6–90.6) | 0.000c |
| Emotional scorea | 70 (56.2–88.7) | 60 (50–75) | 0.000c |
| Social scorea | 90 (80–100) | 85 (70–95) | 0.015c |
| School scorea | 80 (70–90) | 75 (65–90) | 0.097 |
| Psychosocial summarya | 80 (71.7–88.3) | 73.3 (63.3–85) | 0.001c |
| Total scorea | 82.1 (73.1–89.9) | 74.4 (65.5–85.9) | 0.000c |
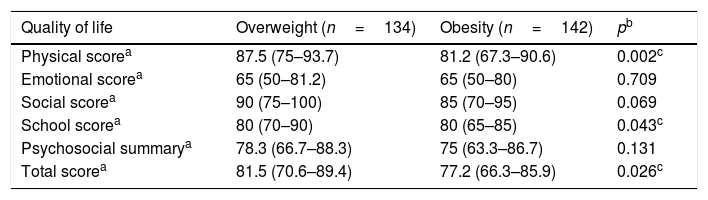
The effects of the variables overweight and obesity were analyzed in Table 4. The obese adolescents showed significant differences regarding the “physical score” (p=0.00), “school score” (p=0.04), and “total score” (p=0.02) when compared to overweight adolescents. There was no significant difference between the emotional, social, and psychosocial scores.
PedsQL subscale scores of adolescents according to nutritional status.
| Quality of life | Overweight (n=134) | Obesity (n=142) | pb |
|---|---|---|---|
| Physical scorea | 87.5 (75–93.7) | 81.2 (67.3–90.6) | 0.002c |
| Emotional scorea | 65 (50–81.2) | 65 (50–80) | 0.709 |
| Social scorea | 90 (75–100) | 85 (70–95) | 0.069 |
| School scorea | 80 (70–90) | 80 (65–85) | 0.043c |
| Psychosocial summarya | 78.3 (66.7–88.3) | 75 (63.3–86.7) | 0.131 |
| Total scorea | 81.5 (70.6–89.4) | 77.2 (66.3–85.9) | 0.026c |
The present study aims to describe the HRQoL of adolescents with excess weight and to compare the probable associated factors such as age, gender, and weight categories (overweight and obesity). To date, this is the first study to publish data on the HRQoL between overweight and obese adolescents from two municipalities in the state of Rio Grande do Sul. When analyzing the PedsQL subscales, this study found a median HRQoL of 78.3 (68.5–87.4) in adolescents with overweight and obesity. The lowest PedsQL subscale score was the “emotional score”.
Some studies,5,12,13 as well as the present one, found the emotional score to be the lowest PedsQL subscale score in overweight and obese adolescents, warning that obesity may be a determinant factor for the decline in HRQoL, especially in the emotional dimension. Lower emotional domains are of concern, mainly when related to the young population with excess weight, since a recent review study14 shows that the food consumption motivated by the emotional state is associated with the development and maintenance of excess weight and obesity.
When adolescents were separated by age group, <14 years and 14–19 years, the group <14 years reported lower scores in the “physical score” and “social score”. The study by Su et al. showed that obese boys in the 3rd and 4th grades had greater difficulties related to the physical score than their peers with normal weight. However, boys in the 5th and 6th grades did not show this difference, which is similar to the findings of this study.15 One hypothesis for the finding is that the perception of children and adolescents about obesity may explain these lower scores regarding the physical score, since the negative perception decreases in an inversely proportional manner to age; also, most adolescents realize that obesity creates limitations in physical performance.16 Contrary to the findings of this study, obesity was associated with a higher HRQoL in younger students (12–14 years), together with higher scores in the emotional and school function and well-being.17
As for the affected “social score” among younger adolescents, it is believed that the age group of 14–19 years shows greater socialization, as they attend more parties, a behavior typical of adolescence. Young obese individuals may suffer a decline in the social domain and perceive these levels as lower than most young individuals, but the perceived social support of classmates, in particular, can have a significant effect on the long-term outcomes of HRQoL for young people who remain obese.18,19
Female gender is associated with a lower HRQoL. In the present study, PedsQL subscale scores were significantly lower in girls, with the exception of the “school score”, and this finding corroborates some studies in which this association is observed in individuals with normal and excess weight.13,20–22 It is believed that the process of body transformation, together with the environment (social media, family and friends) has a greater impact on the female population with excess weight; as a consequence, it may be related to the low levels of HRQoL. The overvaluing of body weight and body image may be another factor that influences HRQoL specifically in girls, as well as physical factors such as puberty (due to menstruation), hormones, and social and beauty norms that are difficult to achieve.15,20,21 Female adolescents with overweight and obesity (self-perceived and measured) require more attention, due to the previously mentioned factors and also due to the increased likelihood of suicidal ideation.23 In this context, it is emphasized that the treatment of overweight and obesity in adolescents should be performed frequently and in the long term, based on targets of dietary behavior rather than weight,19 aiming to prevent a greater decline in the HRQoL of these adolescents with excess weight caused by an inadequate treatment.
It was verified that obese adolescents reported significantly greater losses in the physical, school, and total scores of HRQoL when compared to the overweight category.
Regarding the physical domain, it is believed that Internet use among obese adolescents, social isolation, and emotional state may contribute to the decrease in the HRQoL in the physical domain. A study associating HRQoL and Internet addiction found that obese adolescents have a higher rate of Internet addiction, associated with a lower physical and psychosocial domain. It is likely that Internet addiction caused by emotional malfunction contributes to obesity, since online activities keep individuals from practicing physical activities, and this decrease directly contributes to obesity.24 Another factor that may explain lower physical scores in this study is the damage to social and emotional health caused by obesity, as obese adolescents are generally excluded from competitive activities that require physical effort.25 It is important to emphasize that health professionals should promote their support regarding the adolescents’ behavior to include the increase of vigorous and playful physical activity (at least one hour per day), which the adolescent will enjoy practicing, and which also will reduce screen time.19
An academic consequence was found to be associated with obesity, in which lower school scores were reported by the adolescents, and these losses corroborate the literature data.25–28 A study with Chinese adolescents suggests that learning and memory processes in obese adolescents are different from those in the normal weight category.26 That study found an association between obesity and lower academic performance due to poor basic ability of working memory. The authors proposed that obese adolescents are more sensitive to memory of food and beverage brand materials, and that functional memory deficit for obese adolescents may be domain-specific.26 Additionally, there is a hypothesis that obesity is associated to detectable structural differences in the brain when compared to the brains of normal-weight individuals during childhood and adolescence.27 A recent study28 involving children and adolescents, carried out in Spain, found a positive association between the components of physical fitness with gray matter volume in the cortical and subcortical structures of the brain in children with overweight and obesity. Some of these brain structures were related to better academic performance. The authors hypothesized that promoting physical activity, which leads to improvement in cardiorespiratory fitness and agility/speed, may also be important for the development of the brain and the academic abilities in overweight and obese adolescents.28
The present study found a lower total HRQoL score in obese individuals when compared to overweight adolescents, suggesting that the higher weight category is associated with a lower overall HRQoL. In São Paulo, Brazil, obese adolescents showed an impaired HRQL in PedsQL, affecting the social, emotional, and psychosocial function domains, as well as the general HRQoL, corroborating the present finding.5 Moreover, another Brazilian study of adolescents with excess weight showed the negative impact of the HRQoL perceived by the parents regarding the physical and psychosocial aspects.29
It is thought that this finding may be related to an inversely proportional effect between BMI and HRQoL. A meta-analysis of studies using the PedsQL indicates that there is evidence that HRQoL decreases as BMI increases, a gradient of normal weight, with excess weight for obesity in adolescents.30 Studies often separate adolescents with and without obesity, showing that those with obesity have worse HRQoL.4,5 Thus, it is important to consider the psychosocial aspects involved in adolescents with excess weight. It is necessary to consider the HRQoL in the prevention and treatment of obesity.
However, this study has some limitations. It is a cross-sectional study, so causal inferences cannot be made. The study assessed schools in two cities, and it was not possible to evaluate the socioeconomic status. However, the schools were located in similar socioeconomic areas, which made the schools comparable. As to the HRQoL self-assessment, the PedsQL has already demonstrated its validity and reliability, which has little impact on the conclusions.
These findings highlight the need for clinicians and researchers to incorporate the assessment of HRQoL in overweight and obese adolescents, whereas the identification of more impaired domains may lead to new, more specific interventions for the treatment of overweight and obesity in childhood, as well as treatment adherence. The authors suggest interventions focused on the emotional aspect of this population.
Based on the self-assessment of overweight and obese adolescents, it can be concluded that there are losses in the HRQoL, in different domains, when they are separated by age, gender, and weight category (overweight and obesity). Age was shown to be an associated factor, since the younger age group (<14 years) reported losses in the “physical score” and “social score”. Girls reported lower HRQoL scores in most domains, except for the “school score”. Finally, obese adolescents reported lower scores in the “physical score”, “school score”, and total HRQoL score when compared to the overweight adolescents.
FundingUniversidade de Santa Catarina do Sul – UNISC.
Conflicts of interestThe authors declare no conflicts of interest.
The HRQoL study described in this article was performed using the PedsQL, developed by Dr. James W. Varni. Acknowledgments to the Universidade de Santa Cruz do Sul for authorizing the use of data from the project entitled “Obesidade em adolescentes da educação básica: um estudo de intervenção disciplinar fase III” (“Obesity in adolescents in elementary education: an interdisciplinary intervention study – Phase III”), from the Postgraduate Program in Health Promotion, Master's Degree. Also, the authors would like to thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the grant.




