
Reliable and valid instruments are essential for understanding health-promoting behaviors in adolescents. This study analyzed the psychometric properties of the Portuguese version of the Adolescent Lifestyle Profile (ALP).
MethodsA linguistic and cultural translation of the ALP was conducted with 236 adolescents from two different settings: a community (n=141) and a clinical setting (n=95). Internal consistency reliability and confirmatory factor analysis were performed.
ResultsResults showed an adequate fit to data, yielding a 36-item, seven-factor structure (CMIN/DF=1.667, CFI=0.807, GFI=0.822, RMR=0.051, RMSEA=0.053, PNFI=0.575, PCFI=0.731). The ALP presented a high internal consistency (α=0.866), with the subscales presenting moderate reliability values (from 0.492 to 0.747). The highest values were in Interpersonal Relations (3.059±0.523) and Positive Life Perspective (2.985±0.588). Some gender differences were found. Findings showed that adolescents from the clinic reported an overall healthier lifestyle than those from the community setting (2.598±0.379 vs. 2.504±0.346; t=1.976, p=0.049).
ConclusionThe ALP Portuguese version is a psychometrically reliable, valid, and useful measurement instrument for assessing health-promoting lifestyles in adolescence. The ALP is cross-culturally validated and can decisively contribute to a better understanding of adolescent health promotion needs. Additional research is needed to evaluate the instrument's predictive validity, as well as its clinical relevance for practice and research.
Os instrumentos confiáveis e válidos são fundamentais para entender os estilos de vida de promoção da saúde de adolescentes. Este estudo analisa as propriedades psicométricas da versão em português do Perfil do Estilo de Vida Adolescente (ALP).
MétodosFoi realizada uma tradução linguística e cultural do ALP com 236 adolescentes de duas configurações diferentes: uma configuração de comunidade (N=141) e uma clínica (N=95). Foram realizadas uma análise da confiabilidade da coerência interna e uma análise fatorial confirmatória.
ResultadosOs resultados mostraram-se adequados aos dados, gerando uma estrutura de 7 fatores com 36 itens (CMIN/DF=1,667, IAC=0,807, GFI=0,822, RMR=0,051, RMSEA=0,053, PNFI=0,575, PCFI=0,731). O ALP apresentou grande coerência interna (α=0,866), com as subescalas apresentando valores de confiabilidade moderados (de 0,492 a 0,747). Os maiores valores foram de Relações Interpessoais (3,059±0,523) e Perspectiva de Vida Positiva (2,985±0,588). Foram encontradas algumas diferenças entre os sexos. Os achados mostraram que os adolescentes da clínica relataram um estilo de vida mais saudável em geral que os da configuração da comunidade (2,598±0,379 em comparação a 2,504±0,346; t=1,976, p=0,049).
ConclusãoA versão em português do ALP é um instrumento de mensuração psicometricamente confiável, válido e útil para avaliar os estilos de vida de promoção da saúde na adolescência. O ALP é validado em diferentes culturas e pode contribuir de forma decisiva para um melhor entendimento das necessidades de promoção da saúde na adolescência. É necessária uma pesquisa adicional para avaliar a validade preditiva do instrumento, bem como sua relevância clínica para a prática e pesquisa.
A vital component for attaining the goals of Healthy People 2020 is the promotion of healthy lifestyles. Health promotion continues to be considered the most cost effective approach to improving well-being and quality of life.1 It has been estimated that as much as 60% of the quality of an individual's health and life depends on his/her behavior and lifestyle.1
Results from the 2009/2010 Health Behavior in School-aged Children survey2 indicate variations in patterns of health and its social determinants between countries. Significant inequalities in health and social indicators according to age, gender, and social economic status are also evident. Many effects of health-risk factors among adults are avoidable if these behaviors are identified and changed at an early stage.3 Therefore, it is essential to understand and evaluate health-promoting behaviors among adolescents in order to promote their healthy growth.
Health-promoting behaviors (HPB) are defined as a positive approach to living, increasing well-being, and self-actualization.4 Health promoting activities are defined as those activities that contribute to health, while preventive behaviors are actions to avoid or forestall the development of disease. Pender described a healthy lifestyle as incorporating the complementary components of both health promotion and prevention. HPB develop the energy necessary to increase human potential.4 Use of HPB complements the stabilizing tendency of disease prevention, which is directed toward early detection. Rather than stabilization and avoidance of disease, HPB develop the tension necessary to increase human potential.4
HPB in adolescence have been linked with the psychological attributes of self-esteem, self-efficacy, and hope.5 However, there are few studies on adolescent HPB and a scarce number of instruments have been developed specifically for this purpose: the Adolescent Lifestyle Questionnaire,6 the Adolescent Health-Promoting Scale,7 and the Adolescent Lifestyle Profile (ALP).8
The ALP is conceptually based on the Pender's Health Promotion Model,4 a multidimensional view of HPB that highlights the active role of individuals in managing their own health behavior, widely used for understanding the predictors of health behaviors and lifestyles, namely with adolescents from the USA.9 The ALP was designed to measure the frequency of HPB in adolescents (early, middle, and late) in seven domains: health responsibility, physical activity, nutrition, positive life perspective, interpersonal relations, stress management, and spiritual health. This current version of ALP has been tested in numerous adolescent (11-20 years) samples with documented reliability and validity (alpha coefficient of 0.929).8
Although the ALP has not been used in studies involving others than American adolescents, the adult version from which the ALP was derived (the Health-Promoting Lifestyle Profile) has been translated into Persian,10 Japanese,11 Spanish,12 Turkish,13 Portuguese,14 and Chinese,15 and has been applied to healthy people as well as people with clinical disorders, such as cancer, neurologic, and metabolic syndromes.12
A reliable and valid instrument for the measurement of healthy lifestyles is essential to understand the needs of health promotion among adolescents.16,17 Obtaining an accurate and equivalent cross-cultural assessment of a psychological construct has been considered a key element of research, since the same construct may differ across countries and contexts.18 Moreover, no study so far has applied a standardized instrument for examining such behaviors in a Portuguese adolescent population. Given that Portuguese is the fifth most spoken language in the world, and the third most spoken in the Western Hemisphere, with about 272.9 million speakers, the purpose of the present study was to examine the reliability and construct validity of the Portuguese version of the ALP.
MethodsParticipantsA descriptive cross-sectional study with Portuguese adolescents was conducted. The eligibility criteria were as follows: I) age 12-18 years; II) able to communicate in writing; III) Portuguese nationality; IV) provided informed consent to participate in the study. Exclusion criteria were the presence of severe psychopathology and the inability to complete the questionnaires because of language barriers.
A wide range of recommendations regarding sample size in factor analysis have been made. Some authors19 suggest that 100 respondents is the absolute minimum number to be able to undertake factor analysis. Others would suggest that an adequate sample size for confirmatory factor analysis (CFA) considered n≥200.20 There is also a rule of thumb of five respondents per item.21 Therefore, it was necessary to recruit at least 220 adolescents (5×44 items).
A convenience sample (n=236) was selected based on the eligible population response to the online questionnaire. Adolescents were recruited from two different settings: setting A) students from a community setting (a public high school); setting B) adolescents from a pediatric obesity clinic. Addressing promotion of healthy lifestyles requires a broad approach that includes both health promotion and prevention.4 The option to select a wide variety of participants has the purpose of increasing the external validity of the instrument and addressing this demand.
Participants of setting A (n=141) were recruited with the support of the teachers, according to the research protocol previously given. Participants of setting B (n=95) were recruited with the support of the clinical staff, according to the research protocol previously given. Data collection in both samples occurred in 2012. Baseline comparison indicated that both settings were equivalent regarding adolescents¿ sociodemographic characteristics.
InstrumentThe ALP8 was designed to measure the frequency of health promoting behaviors in adolescents (early, middle, and late). The revised Health-Promoting Lifestyle Profile-II served as the prototype for the initial generation of the ALP. It became apparent that items used for adults did not “fit” adolescents. Internal consistency reliability and construct validity indicated that the ALP was reliable and valid.8
The ALP has undergone some minor revisions since its development. The ALP current version (ALP-R2©) is a 44-item summated behavior rating scale that employs a four-point Likert-type response format, ranging from 1=“Never” to 4=“Always”, with a possible score between 44 and 176.
Hendricks et al.8 reported Cronbach's alphas for the seven subscales: Health Responsibility (HR; 0.825), Physical Activity (PA; 0.773), Nutrition (N; 0.648), Positive Life Perspective (PLP; 0.810), Interpersonal Relations (IR; 0.769), Stress Management (SM; 0.656), and Spiritual Health (SH; 0.824). The total ALP reliability score was 0.929. A principal axis factor analysis supported the presence of the seven factors used as subscales. The higher the score on a subscale, the greater the health behavior for that domain. Both subscales and a total scale score can be obtained. Strong correlations between the ALP and the Adolescent Hope Scale and between the ALP and the Self-Efficacy Scale were identified in a previous study with a sample of 168 student-athletes.9
ProceduresThe cultural adaptation of ALP to the Portuguese language was authorized by the authors of the original version. Two bilingual translators, specialists in health sciences, separately translated the English original version into European Portuguese, reaching a consensual version after two iterations. Next, two other bilingual translators (independent of the firstpair), also specialists in health sciences, back translated the scale into English, obtaining a final version by consensus after two iterations.22 The translation procedure was evaluated for conceptual, semantic, content, technical, and criterion equivalences by a panel of five investigators with extensive background in health intervention research, behavioral modification, and health promotion. The two versions were sent to the ALP authors, who considered the versions equivalent.
A pilot study was then conducted with eight adolescents, aged 12-18 years, who were not included in the main study. The adolescents evaluated the instructions, response format, and the instrument items for clarity. Each participant rated the instructions and scale items as either clear or unclear. No difficulties in understanding and completing the instrument were identified.
The research protocol was formally approved by the Ethics Committee and the Hospital Administration, and by the Portuguese Department of Education (Direção Geral de Inovação e de Desenvolvimento Curricular). All procedures respected the Declaration of Helsinki23 and the ethical principles of the American Psychological Association.24 All participants had access to the description of the study and its objectives, and were informed of all the ethical aspects inherent to the confidentiality and voluntary basis of their participation.
Data AnalysisThe online questionnaire data was analyzed with Statistical Package for Social Sciences (SPSS Inc. Statistics for Windows, version 17.0, Chicago, USA) and AMOS (SPSS Inc. Computer Program, version 20.0, Chicago, USA) software. Descriptive statistics were calculated for each item. The ALP total score was obtained by averaging the responses to all items. The same procedure was adopted for all the subscales scores.
Internal consistency using Cronbach's alpha was calculated for the total scale as well as for each subscale. The homogeneity indices was also analyzed in order to determine which items to consider for elimination. According to Hair et al.,25 an item with a corrected item-total correlation less than 0.20 should be deleted. An acceptable alpha reliability coefficient is considered to be 0.80 or greater for a tested scale.26
A confirmatory factor analysis (CFA) was used to test the adequacy of the model underlying the original structure of the ALP proposed by the authors. Once the model was defined, the multivariate normality was analyzed with the Mardia coefficient (99.974). Therefore, assuming the existence of multivariate normality, the model parameters were estimated using the maximum likelihood procedure. The CFA criteria for an acceptable model were:
- -
chi-squared/degrees of freedom (CMIN/DF)<3.0; comparative fit index (CFI) and goodness of fit index (GFI)>0.80; root mean square residual (RMR) and root mean square error of approximation (RMSEA)<0.05;25,27
- -
parsimony normed fit index (PNFI) and parsimony comparative fit index (PNFI)>0.50.28
Following the recommendations of Marsh et al.,29 the criteria applied in the selection of items to develop a short-form of ALP were: factor loadings, corrected item-test correlation, Cronbach's alpha, skewness/kurtosis (sk/ku) values, and the theoretical importance in itself of the different items.
ResultsSociodemographic and behavioral characteristicsThe study sample included 236 adolescents, 45.8% male and 54.2% female. The mean age of the participants was 15.15±1.583. The mean overall lifestyle score reported by adolescents was 2.542±0.362. On the ALP domains, adolescents scored highest on IP (3.059±0.523) and PLP (2.985±0.588), and scored lowest on SH (1.860±0.640).
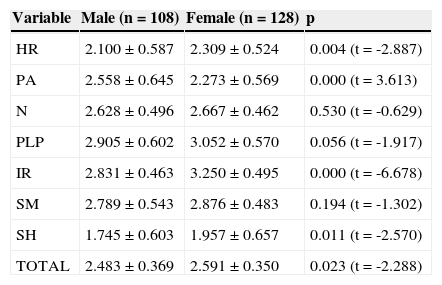
Table 1 presents the descriptive statistics of the total scale and subscales. Total and subscale mean scores differed between males and females. Females reported an overall healthier lifestyle than males (2.591±0.350 vs. 2.483±0.369; t=-2.288, p=0.023). Adolescents from the clinic reported an overall healthier lifestyle than those from the community setting (2.598±0.379 vs. 2.504±0.346; t=1.976, p=0.049). They also reported higher values on the N subscale (t=4.000, p=0.000) and lower values on the SM subscale (t=2.559, p=0.011).
Descriptive statistics of Portuguese version of the Adolescent Lifestyle Profile (36 items) according to gender and clinical/community setting.
| Variable | Male (n=108) | Female (n=128) | p |
|---|---|---|---|
| HR | 2.100±0.587 | 2.309±0.524 | 0.004 (t=-2.887) |
| PA | 2.558±0.645 | 2.273±0.569 | 0.000 (t=3.613) |
| N | 2.628±0.496 | 2.667±0.462 | 0.530 (t=-0.629) |
| PLP | 2.905±0.602 | 3.052±0.570 | 0.056 (t=-1.917) |
| IR | 2.831±0.463 | 3.250±0.495 | 0.000 (t=-6.678) |
| SM | 2.789±0.543 | 2.876±0.483 | 0.194 (t=-1.302) |
| SH | 1.745±0.603 | 1.957±0.657 | 0.011 (t=-2.570) |
| TOTAL | 2.483±0.369 | 2.591±0.350 | 0.023 (t=-2.288) |
| School (n=141) | POC/HSM (n=95) | ||
|---|---|---|---|
| HR | 2.178±0.558 | 2.266±0.567 | 0.243 (t=1.170) |
| PA | 2.399±0.588 | 2.410±0.668 | 0.887 (t=0.143) |
| N | 2.550±0.456 | 2.796±0.474 | 0.000 (t=4.000) |
| PLP | 2.936±0.564 | 3.056±0.618 | 0.124 (t=1.544) |
| IR | 3.039±0.509 | 3.087±0.545 | 0.487 (t=0.697) |
| SM | 2.767±0.483 | 2.939±0.538 | 0.011 (t=2.559) |
| SH | 1.895±0.651 | 1.807±0.624 | 0.303 (t=-1.032) |
| TOTAL | 2.504±0.346 | 2.598±0.379 | 0.049 (t=1.976) |
HR, health responsibility; PA, physical activity; N, nutrition; PLP, positive life perspective; IR, interpersonal relations; SM, stress management; SH, spiritual health; POC/HSM, Pediatric Obesity Clinic, Department of Pediatrics, Hospital de Santa Maria.
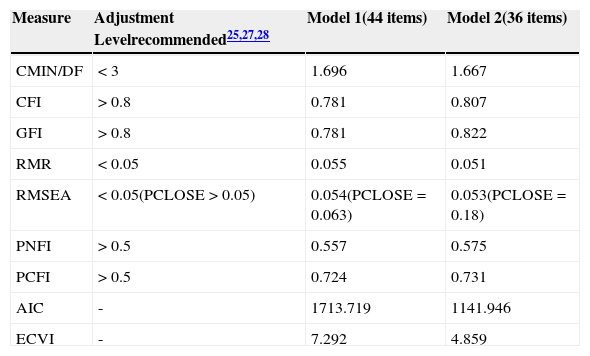
CFA was performed to test how well the correlations between the items corresponded to the original ALP scale structure. The results of the CFA did not provide satisfactory fit indexes for the initial model (CFI=0.781, GFI=0.781, RMR=0.055, RMSEA=0.054; Table 2).
Summary of the adjustment indices of the Portuguese version of the Adolescent Lifestyle Profile.
| Measure | Adjustment Levelrecommended25,27,28 | Model 1(44 items) | Model 2(36 items) |
|---|---|---|---|
| CMIN/DF | < 3 | 1.696 | 1.667 |
| CFI | > 0.8 | 0.781 | 0.807 |
| GFI | > 0.8 | 0.781 | 0.822 |
| RMR | < 0.05 | 0.055 | 0.051 |
| RMSEA | < 0.05(PCLOSE>0.05) | 0.054(PCLOSE=0.063) | 0.053(PCLOSE=0.18) |
| PNFI | > 0.5 | 0.557 | 0.575 |
| PCFI | > 0.5 | 0.724 | 0.731 |
| AIC | - | 1713.719 | 1141.946 |
| ECVI | - | 7.292 | 4.859 |
CMIN/DF, chi-squared/degrees of freedom; CFI, comparative fit index; GFI, goodness of fit index; RMR, root mean square residual; RMSEA, root mean square error of approximation; PNFI, parsimony normed fit index; PCFI, parsimony comparative fit index; AIC, Akaike information criterion; ECVI, expected cross validation index; PCLOSE, p value of close fit.
Therefore, a shorter version was developed, taking into consideration the predefined criteria. Eight items were eliminated: three items with low factor loads or low item-total correlations, and five items with sk/ku values either below -1 or above 1. Two items were kept attending to their theoretical importance (ALP4 and ALP13). The HR, SH, SM, and PA subscales lost one item each and the PLP and IR subscales lost two items each.
The model 2 structure comprised seven latent variables, 36 observed variables, and 36 error terms. The refinement of model 2 was based on modification indices. The correlations trajectories were allowed between the error terms e4-e6, and e19-e20.
The goodness-of-fit values were adequate attesting the factorial validity of ALP Portuguese version (Table 2): CMIN/DF=1.667, CFI=0.807, GFI=0.822, RMR=0.051, RMSEA=0.053, PNFI=0.575, PCFI=0.731. Analysing comparative measures of fit with the Akaike information criterion (AIC) and expected cross validation index (ECVI), both estimated models were compared. Model 1 (44 items) scores were: AIC=1,713.719 and ECVI=7.292. Model 2 (36 items) scores were: AIC=1,141.946 and ECVI=4.859. As lower values indicate a better fit, Model 2 was considered the best fitting model.
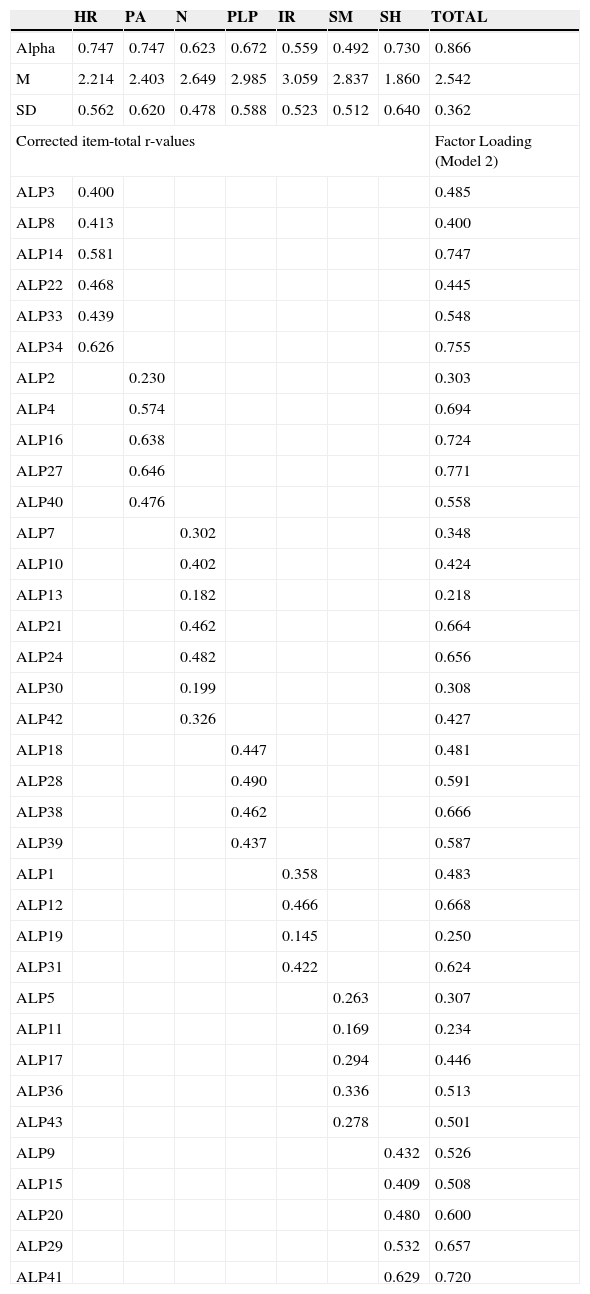
ReliabilityCronbach's alpha was used as an estimate of internal consistency reliability. The total alpha was 0.866 and the reliability values of the seven subscales ranged from 0.492 (SM) to 0.747 (HR and PA). Corrected item-total r-values ranged between 0.145 (ALP19) and 0.646 (ALP27); factor loadings ranged between 0.218 (ALP13) and 0.771 (ALP27; Table 3).
Descriptive statistics, corrected item-total r-values, factor loadings, and Cronbach's alpha of the Portuguese version of the Adolescent Lifestyle Profile (ALP; 36 items).
| HR | PA | N | PLP | IR | SM | SH | TOTAL | |
|---|---|---|---|---|---|---|---|---|
| Alpha | 0.747 | 0.747 | 0.623 | 0.672 | 0.559 | 0.492 | 0.730 | 0.866 |
| M | 2.214 | 2.403 | 2.649 | 2.985 | 3.059 | 2.837 | 1.860 | 2.542 |
| SD | 0.562 | 0.620 | 0.478 | 0.588 | 0.523 | 0.512 | 0.640 | 0.362 |
| Corrected item-total r-values | Factor Loading (Model 2) | |||||||
| ALP3 | 0.400 | 0.485 | ||||||
| ALP8 | 0.413 | 0.400 | ||||||
| ALP14 | 0.581 | 0.747 | ||||||
| ALP22 | 0.468 | 0.445 | ||||||
| ALP33 | 0.439 | 0.548 | ||||||
| ALP34 | 0.626 | 0.755 | ||||||
| ALP2 | 0.230 | 0.303 | ||||||
| ALP4 | 0.574 | 0.694 | ||||||
| ALP16 | 0.638 | 0.724 | ||||||
| ALP27 | 0.646 | 0.771 | ||||||
| ALP40 | 0.476 | 0.558 | ||||||
| ALP7 | 0.302 | 0.348 | ||||||
| ALP10 | 0.402 | 0.424 | ||||||
| ALP13 | 0.182 | 0.218 | ||||||
| ALP21 | 0.462 | 0.664 | ||||||
| ALP24 | 0.482 | 0.656 | ||||||
| ALP30 | 0.199 | 0.308 | ||||||
| ALP42 | 0.326 | 0.427 | ||||||
| ALP18 | 0.447 | 0.481 | ||||||
| ALP28 | 0.490 | 0.591 | ||||||
| ALP38 | 0.462 | 0.666 | ||||||
| ALP39 | 0.437 | 0.587 | ||||||
| ALP1 | 0.358 | 0.483 | ||||||
| ALP12 | 0.466 | 0.668 | ||||||
| ALP19 | 0.145 | 0.250 | ||||||
| ALP31 | 0.422 | 0.624 | ||||||
| ALP5 | 0.263 | 0.307 | ||||||
| ALP11 | 0.169 | 0.234 | ||||||
| ALP17 | 0.294 | 0.446 | ||||||
| ALP36 | 0.336 | 0.513 | ||||||
| ALP43 | 0.278 | 0.501 | ||||||
| ALP9 | 0.432 | 0.526 | ||||||
| ALP15 | 0.409 | 0.508 | ||||||
| ALP20 | 0.480 | 0.600 | ||||||
| ALP29 | 0.532 | 0.657 | ||||||
| ALP41 | 0.629 | 0.720 | ||||||
HR, health responsibility; PA, physical activity; N, nutrition; PLP, positive life perspective; IR, interpersonal relations; SM, stress management; SH, spiritual health.
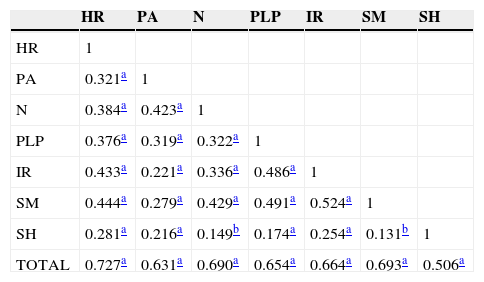
All subscales had significant, moderate-to-strong correlations with the total scale, meeting minimal criteria (Table 4). Correlations ranged from 0.506 (SH) to 0.727 (HR). Subscale to subscale correlations were also statistically significant (p<0.05), ranging from 0.131 (SH–SM) to 0.524 (SM–IR).
Pearson correlations between thePortuguese version of the Adolescent Lifestyle Profile factors and total score.
| HR | PA | N | PLP | IR | SM | SH | |
|---|---|---|---|---|---|---|---|
| HR | 1 | ||||||
| PA | 0.321a | 1 | |||||
| N | 0.384a | 0.423a | 1 | ||||
| PLP | 0.376a | 0.319a | 0.322a | 1 | |||
| IR | 0.433a | 0.221a | 0.336a | 0.486a | 1 | ||
| SM | 0.444a | 0.279a | 0.429a | 0.491a | 0.524a | 1 | |
| SH | 0.281a | 0.216a | 0.149b | 0.174a | 0.254a | 0.131b | 1 |
| TOTAL | 0.727a | 0.631a | 0.690a | 0.654a | 0.664a | 0.693a | 0.506a |
HR, health responsibility; PA, physical activity; N, nutrition; PLP, positive life perspective; IR, interpersonal relations; SM, stress management; SH, spiritual health.
In order to assess adolescent lifestyle behaviors and help planning appropriate interventions, a comprehensive, easy to administer, both psychometrically sound and clinically useful instrument is needed.8 The purpose of this study was to report the psychometric properties of the Portuguese version of the ALP.
Construct validity was tested through CFA. The Revised CFA resulted in a better fit of the model for the Portuguese version (36 items), when compared to the original structure. The exclusion of eight items may reflect the fact that some items have meanings that overlap with more than one concept. The difficulties perceived in translating some of the items into Portuguese were noteworthy, which may explain the differences encountered.
The IR subscale lost two items (ALP6 - “Congratulate others…” and ALP37 - “Make a special effort to be helpful…”). The PLP subscale also lost two items (ALP23 - “Am happy with who I am” and ALP26 - “Work toward important goals…”). The SM subscale lost one item (ALP25 - “Take time for myself…”), as well as the SH subscale (ALP35- “Spend time in prayer or meditation”). The exclusion of these items was based on low corrected item-test correlations and irregular sk/ku values, and may reflect the difficulty of Portuguese adolescents in accepting these as HPB. The PLP concept, SH, and SM strategies may not be sufficiently used or understood by Portuguese adolescents yet.
However, the need for elimination of the items ALP44 (Avoid behaviors that damage my health - smoking, drinking, doing drugs, sexual activity) and ALP32 (Play active games with my friends - basketball, softball, volleyball, tennis, etc.) may be explained differently. The complexity of the items, as they contain multiple behaviors, might have contributed to the difficulty encountered in answering.
Despite presenting a low factor loading (ALP13: Eat breakfast) and high sk/ku values (ALP4: Engage in vigorous physical activity for 20minutes or more three days a week), it was decided to keep these two items, due to their theoretical importance. In fact, they provide valuable information on nutrition and physical activity behavior strategies that are essential for learning about lifestyle choices.8
The construct validity of the original ALP was analyzed using exploratory factor analysis (EFA). Therefore, there are no CFA model fit indexes available for use for comparison. However, taking into consideration recent recommendations for using structural equation modeling,25,27,28 the emerging model (36 items) presented an adequate fit to the data, yielding a seven-factor structure. Previous studies have noted that major caution must be adopted when assuming a single ‘critical cut-off point’ value, especially using GFI, TLI, IFI, and CFI, considering the susceptibility of indices to model complexity and data distribution.
The Cronbach's alpha obtained was adequate (α=0.866) but lower than in the original study (0.929),8 which may reflect the cultural difference for items originally in the ALP. Moreover, some authors consider that the maximum expected value is 0.90. Above this value, either there is redundancy or duplication, or several items are measuring the same element of a construct.30
The present results suggest a strong relationship between the concepts represented by each subscale, particularly between IR and SM, which is consistent with the fact that both subscales analyze cognitive and emotional aspects. The concept of stress management involves identifying and mobilizing psychological and physical resources for reducing and managing stress effectively. The IR subscale refers to the use of communication to achieve a sense of intimacy and closeness in meaningful relationships, involving sharing of thoughts and feelings, through verbal and nonverbal messages.4
Findings also suggests that these adolescents tend to engage in meaningful and healthy relationships, maximizing their human potential for wellness through finding a sense of purpose, and working toward a goal in life. However, they may have difficulty in considering spiritual aspects as protective, and as HPB.
Interestingly, some gender differences were found. Female adolescents reported higher mean scores in HR, IR, and SH, with male adolescents reporting higher PA mean scores.
These findings also demonstrated that adolescents from the clinic reported higher scores in HPB, probably reflecting the fact that they are regularly exposed to multidisciplinary medical, psychological, nutritional, and physical activity support.
Among the limitations of this study is the sampling technique, namely use of a non-random sample from two settings, which prevents generalizability of the results to other samples of Portuguese adolescents and may have caused some bias. Another limitation concerns the small sample size (n=236), which may limit the interpretation of the CFI results.
The Portuguese version of the ALP showed good psychometric properties, both in terms of validity and reliability. The current study supports the cross-cultural utility of the ALP as a tool for assessing health-promoting lifestyles among adolescents, representing a crucial instrument to understand and meet adolescents’ health promotion needs. Future research is needed to examine the predictive validity of the Portuguese version of the scale.
FundingThis work was partially funded by Fundação para a Ciência e a Tecnologia (PTDC/DTP-PIC/0769/2012) and supported by the Polytechnic Institute of Leiria, Portugal and the Department of Pediatrics at Hospital de Santa Maria, Lisbon, Portugal.
Conflicts of interestThe authors declare no conflicts of interest.
This work was partially funded by Fundação para a Ciência e a Tecnologia (PTDC/DTP-PIC/0769/2012) and supported by the Polytechnic Institute of Leiria, Portugal and the Department of Pediatrics at Hospital de Santa Maria, Lisbon, Portugal. The authors gratefully acknowledge the clinical staff of the Pediatric Obesity Clinic for their dedication. They also thank all the adolescents and parents for their participation and collaboration.
Please cite this article as: Sousa P, Gaspar P, Fonseca H, Hendricks C, Murdaugh C. Health promoting behaviors in adolescence: validation of the Portuguese version of the Adolescent Lifestyle Profile. J Pediatr (Rio J). 2015;91:358–65.




