
The aim of this study was to examine the prevalence of parental misperception of child weight status, and identify socioeconomic, anthropometric, behavioral and dietary factors associated with underestimation.
MethodCross-sectional study. Data was collected in 14 Brazilian private schools. Parents of children aged 2–8 years (n=976) completed a self-reported questionnaire assessing their perception of their child's weight status, and sociodemographic, anthropometric, behavioral and dietary information. To measure the agreement between parental perception about child weight status and actual child weight status, the Kappa coefficient was estimated, and to investigate associations between parental underestimation and independent variables, chi-squared tests were performed, followed by multiple logistic regression, considering p≤0.05 for statistical significance.
ResultsOverall, 48.05% of the parents incorrectly classified their child's weight. Specifically, 45.08% underestimated their child's weight status, with just 3% of parents overestimating. Children with higher body mass index (OR=2.03; p<0.001) and boys (OR=1.70; p<0.001) were more likely to have their weight status underestimated by parents.
ConclusionSince awareness of weight problems is essential for prevention and treatment, clinical practitioners should help parents at high risk of misperception to correctly evaluate their child's weight status.
Analisar a prevalência de percepção errônea dos pais sobre o status do peso infantil e identificar fatores socioeconômicos, antropométricos, comportamentais e dietéticos associados à subestimação.
MétodoTrata-se de um estudo transversal. Os dados foram coletados em 14 escolas particulares brasileiras. Pais de crianças de dois a oito anos de idade (n=976) preencheram um questionário autoaplicável sobre sua percepção do estado nutricional do seu filho e informações sociodemográficas, antropométricas, comportamentais e dietéticas. Para medir o grau de concordância entre a percepção dos pais do peso do filho e o peso real do filho, estimamos o coeficiente Kappa e investigamos as associações entre subestimação do pai e variáveis independentes, calculamos o qui-quadrado seguido do modelo de regressão logística múltipla considerando p≤0,05 para significância estatística.
ResultadosEm geral, 48,05% dos pais classificaram incorretamente o peso de seus filhos; particularmente, 45,08% subestimaram o peso do seu filho, e apenas 3% subestimaram o peso infantil. A regressão logística demonstrou que as crianças com maior índice de massa corporal (OR=2,03; p<0,001) e os meninos (OR=1,70; p<0,001) tinham maior probabilidade de ter seu peso subestimado pelos pais.
ConclusãoMédicos clínicos devem concentrar suas intervenções nessas crianças para ajudar os pais a avaliar corretamente o seu peso. A consciência dos pais sobre um problema de peso em crianças é essencial para a prevenção e tratamento da obesidade infantil e estilos de vida saudáveis.
Childhood overweight is a recognized public health problem. According to the most recent report about childhood obesity from the World Health Organization (WHO), in 2014, an estimated 41 million children under 5 years of age were overweight or obese. This pandemic has also reached developing nations, including those in Asia, Africa, and Latin America.1 In Brazil, national surveys have demonstrated an increasing trend of overweight and obesity prevalence in children from 5 to 9 years of age. In 1974–1975, the prevalence of overweight in boys was 10.9%, and in 1989, it increased to 15%, reaching 34.8% in the last national survey in 2008–2009. A similar pattern of increase has also been observed in girls, rising from 8.6%, to 11.9%, and then to 32%. These increases in obesity prevalence in both genders follow worldwide trends in overweight,2 with the WHO describing obesity as one of today's most blatantly visible – yet most neglected - public health problems.3
Excessive weight gain in childhood is the result of many factors, including unhealthy eating habits and sedentary behaviors, which are influenced by media, peers and parents.1 Parents play a unique role as the child's first nutritional educators, shaping food environments and eating behaviors. Accurate perception of child's weight status by the parent may be an important factor in motivating the promotion of a healthy lifestyle,4 with parents forming potential ‘agents of change’ in the recognition and treatment of childhood obesity.5 Early intervention by parents could be critical in the prevention and treatment of overweight and obesity, as dietary patterns and eating habits are often formed in childhood, and persist through adolescence into adulthood.6
However, parents can be insensitive to excessive weight in their child, only recognizing it in severe stages or when the child presents with limitations in physical activity, such as breathlessness or reduced physical mobility.7 Population-wide, parental underestimation may be substantially driven by rising rates of childhood obesity over the last decades, which have understandably increased the weight perceived as ‘normal.’8 Studies have repeatedly demonstrated parental underestimation of child weight,9–11 with a meta-analysis reporting that the proportion of parental underestimation among overweight/obese children was 50.7%, and 14.3% for normal weight children.12
Perceptions are influenced by the relationship between the perceiver and the person who is perceived, as well as the perceiver's experiences, beliefs, and characteristics, which will affect thoughts, feelings and attitudes about the perceived person,13 as well as characteristics of the perceived person. Consistent with this, several studies have shown relationships between parental misperceptions about child weight status and parental and child characteristics. For example, one study reported that obesity in both parent and child increased the chance of underestimation, with parental concern about child overweight increasing, rather than decreasing, the risk of misperception.6 Another study in Chile found that mothers with lower education, mothers of boys, and mothers of older children were more likely to underestimate their child's weight status.14 However, an American study reported an association between greater child age and lower rates of parental misperception about self-reported child weight status.15
Notably, most of the extant studies assessing parent perceptions of child weight have been conducted in developed countries,6,15–18 with only a few performed in Brazil,10,11,19 none of which conducted a comprehensive assessment of parent's misperception and associated factors. A greater understanding of the determinants of weight perceptions in Brazil is important so that education can be focused on parents at greater risk of misperception. The aim of this study was therefore to examine the prevalence of parental misperception of child weight status in a Brazilian sample, and to identify socioeconomic, anthropometric, behavioral, and dietary factors associated with parental underestimation of child weight.
MethodParticipantsParents of children aged 2–8 years were eligible to participate in this study. The study excluded children with diseases that were related to nutrition; siblings, in order to avoid sample unit duplication, keeping only the youngest child; cases with missing answers on parental perception of child weight; and body mass outliers (BMI for age ≥6.00 z-score and ≤−6.00). To estimate the required sample size, a type I and a type II probability of error of 0.05 and 0.20 were considered, respectively, based on the prevalence of child overweight. This resulted in a sample of 320 respondents, incorporating over-recruitment to accommodate an anticipated loss of 10% of the original sample.
ProceduresForty-eight private schools in the cities of São Paulo and Campinas, Brazil were contacted, with initial contacts followed up at a meeting with the school's headmaster and/or coordinator. Of these 48 schools, 14 accepted the invitation to participate in the study. Full details about study procedures are described elsewhere.20,21 This research received ethical approval from the Federal University of São Paulo (UNIFESP) ethics committee. The mother or the father of each participating child gave written informed consent before completing the survey.
MeasuresParents completed a self-reported questionnaire assessing sociodemographic, anthropometric, behavioral, and dietary information. Child food intake was measured using the Food Frequency Questionnaire developed specifically for this project and tested in a pilot study, since there was no instrument validated in Brazil that met the criteria of being both brief and appropriate for this age group. Ultra-processed food intake during the seven days prior to the interview was summed and its mean was calculated (risk was designated if ultra-processed food intake was above the mean intake, i.e., ≥3 times per week). The absence of parents during mealtimes was assessed by the number of major meals (breakfast, lunch, and dinner) for which each parents was absent during a regular week; ‘absence during mealtime’ was designated when both parents were absent for at least one major meal in the week. Parental perception of child weight status was assessed by completing the statement ‘In your opinion, your child is…’ with the following six response options: ‘very thin,’ ‘slightly thin,’ ‘normal,’ ‘slightly fat,’ ‘fat,’ and ‘very fat.’ WHO growth standards were used to calculate BMI z-scores and weight categories based on reported weight and height.22 ‘Extremely underweight’ was defined as z-score <−3; ‘underweight,’ as z-score ≥−3 and <−2; ‘normal weight,’ as z-score ≥−2 and <+1; ‘overweight,’ as z-score ≥+1 and <+2; ‘obese,’ as z-score ≥+2 and <+3; and ‘extremely obese,’ as z-scores ≥+3. In order to create weight categories from reported weight and height data that allowed for a margin of error in parents’ estimates, the continuous variable ‘child BMI z-score’ categories were rounded, such that z-scores −5.50 to −4.50 became −5.0, etc. For ‘Perceived responsibility for child feeding’ and ‘Concern about child overweight’ scales from the Child Feeding Questionnaire (CFQ),23 the authors calculated means and used the median to create dichotomous variables.
Statistical analysisTo measure agreement between parental perceptions of child weight status and child weight status as reported by parents, the Kappa coefficient was estimated for the whole sample. Kappa values <0.00 indicate poor agreement, and values >0.80 indicate almost perfect agreement.24 In order to explore the distribution of the variables in the dataset and choose the appropriate cut-off for dichotomization, descriptive analyses were conducted. Since the aim of the study was to evaluate parental underestimation of child weight, the dependent variable was dichotomized to form the categories ‘underestimation’ and ‘no underestimation.’ Dichotomization of independent variables was based on the distribution of each variable and guided by a literature review exploring values associated with risk of misperception. Chi-squared tests were used to identify associated factors with parental perception of child weight status. Then, all variables with p≤0.20 in the chi-squared test were carried forward to a multiple regression model. Variables with p≤0.05 were considered significant in this model. The consistency of the dataset was verified by entering the data twice with the help of two trained assistant researchers. The analyses were performed using Stata (Stata Statistical Software, Version 14. College Station, TX, USA).25
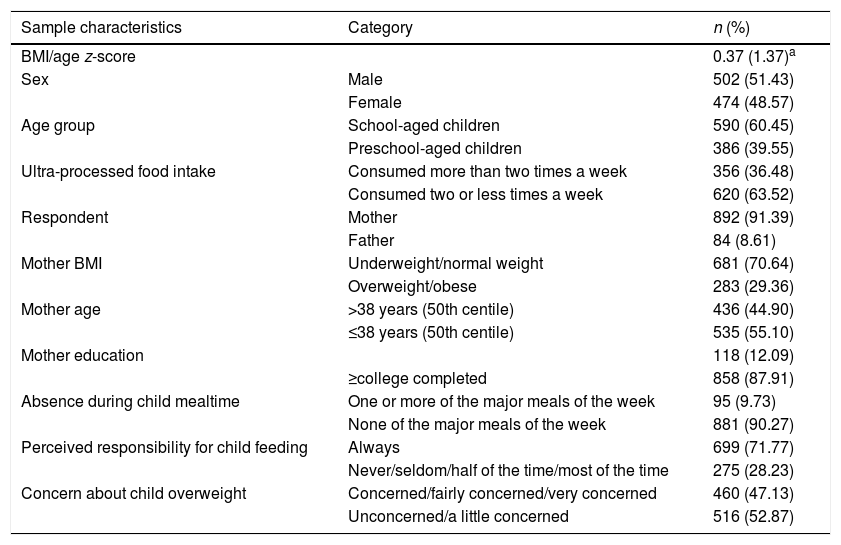
ResultsTable 1 shows the results of descriptive analyses of anthropometric, sociodemographic, dietary, and behavioral characteristics. Most of the respondents were mothers (91.39%), almost 30% were classified as overweight/obese, and the majority was highly educated (87.91%). Approximately 72% of the parents perceived themselves as always responsible for child feeding on the evaluated dimensions.
Anthropometric, sociodemographic, dietary, and behavioral characteristics of the sample (n=976).
| Sample characteristics | Category | n (%) |
|---|---|---|
| BMI/age z-score | 0.37 (1.37)a | |
| Sex | Male | 502 (51.43) |
| Female | 474 (48.57) | |
| Age group | School-aged children | 590 (60.45) |
| Preschool-aged children | 386 (39.55) | |
| Ultra-processed food intake | Consumed more than two times a week | 356 (36.48) |
| Consumed two or less times a week | 620 (63.52) | |
| Respondent | Mother | 892 (91.39) |
| Father | 84 (8.61) | |
| Mother BMI | Underweight/normal weight | 681 (70.64) |
| Overweight/obese | 283 (29.36) | |
| Mother age | >38 years (50th centile) | 436 (44.90) |
| ≤38 years (50th centile) | 535 (55.10) | |
| Mother education | 118 (12.09) | |
| ≥college completed | 858 (87.91) | |
| Absence during child mealtime | One or more of the major meals of the week | 95 (9.73) |
| None of the major meals of the week | 881 (90.27) | |
| Perceived responsibility for child feeding | Always | 699 (71.77) |
| Never/seldom/half of the time/most of the time | 275 (28.23) | |
| Concern about child overweight | Concerned/fairly concerned/very concerned | 460 (47.13) |
| Unconcerned/a little concerned | 516 (52.87) |
BMI, body mass index.
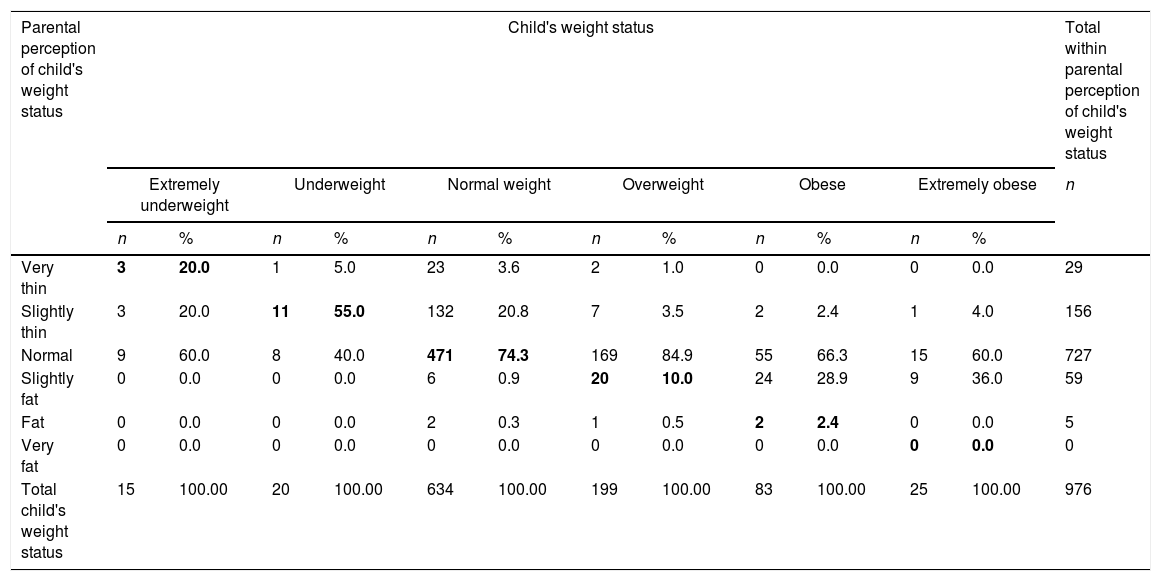
Table 2 shows the agreement between parental perceptions of child weight status and child weight status reported by parents. Parents of underweight and normal weight children tended to accurately perceive their child's weight status, when compared to overweight and obese children. The sample was composed of 31.45% overweight and obese children. Among these, the more overweight the child, the more inaccurate the parent's perception of child actual weight status, e.g. when the child was classified as extremely obese, the majority of parents perceived them as slightly fat (36.0%) or even normal weight (60.0%), and when the child was classified as overweight, parents perceived them as normal weight (84.9%). Overall, 48.05% of the parents incorrectly classified their child's weight. More specifically, 2.97% of parents overestimated and 45.08% underestimated their child's weight status. The poor agreement of parent's perception and child's weight status was confirmed by the Kappa coefficient (0.038).
Agreement between parental perceptions of child's weight status and child's weight status in a sample of preschool and school-aged children from São Paulo and Campinas-SP, Brazil. n=976.
| Parental perception of child's weight status | Child's weight status | Total within parental perception of child's weight status | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Extremely underweight | Underweight | Normal weight | Overweight | Obese | Extremely obese | n | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Very thin | 3 | 20.0 | 1 | 5.0 | 23 | 3.6 | 2 | 1.0 | 0 | 0.0 | 0 | 0.0 | 29 |
| Slightly thin | 3 | 20.0 | 11 | 55.0 | 132 | 20.8 | 7 | 3.5 | 2 | 2.4 | 1 | 4.0 | 156 |
| Normal | 9 | 60.0 | 8 | 40.0 | 471 | 74.3 | 169 | 84.9 | 55 | 66.3 | 15 | 60.0 | 727 |
| Slightly fat | 0 | 0.0 | 0 | 0.0 | 6 | 0.9 | 20 | 10.0 | 24 | 28.9 | 9 | 36.0 | 59 |
| Fat | 0 | 0.0 | 0 | 0.0 | 2 | 0.3 | 1 | 0.5 | 2 | 2.4 | 0 | 0.0 | 5 |
| Very fat | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 |
| Total child's weight status | 15 | 100.00 | 20 | 100.00 | 634 | 100.00 | 199 | 100.00 | 83 | 100.00 | 25 | 100.00 | 976 |
Bold values represent accurate parental perception about child's weight status. Kappa coefficient: 0.038; agreement: 51.95%; p-value:=0.013.
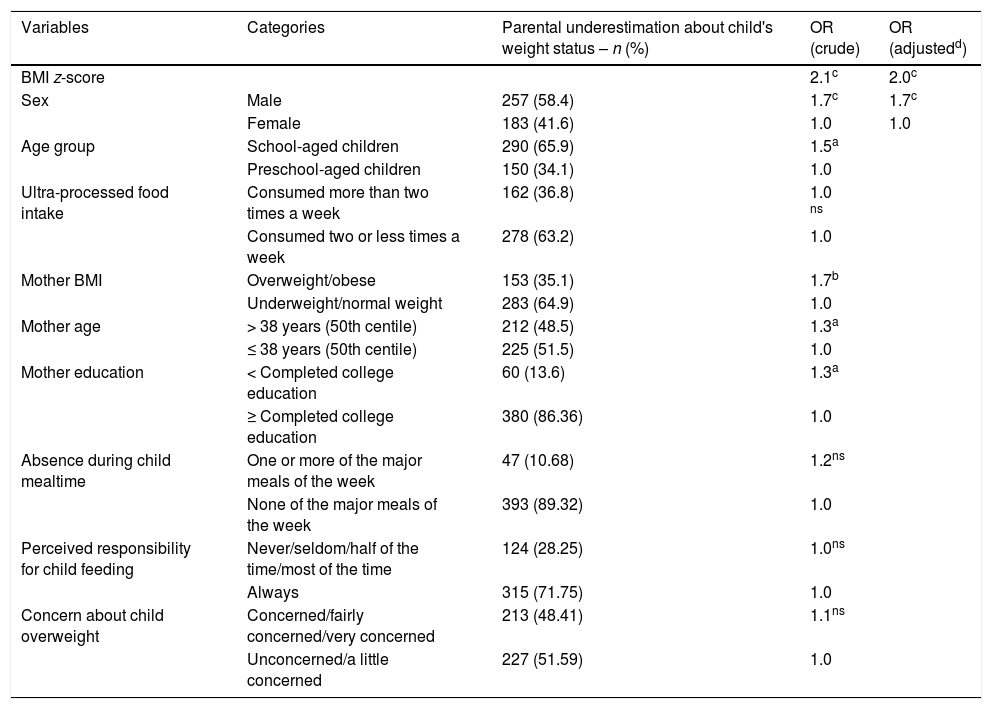
Univariate analyses demonstrated that boys, children with higher BMIs, and school-aged children were more likely to have their weight status underestimated by their parents. Overweight/obese mothers and older mothers were also more likely to underestimate child weight status. Independently associated factors emerging from the multiple regression included higher child BMI (OR=2.03) and being a boy (OR=1.70), regardless of child age, and mother's age, education, and BMI (Table 3).
Univariate and multiple logistic regression models predicting parental underestimation of child's weight status in a sample of preschool and school-aged children from São Paulo and Campinas-SP, Brazil.
| Variables | Categories | Parental underestimation about child's weight status – n (%) | OR (crude) | OR (adjustedd) |
|---|---|---|---|---|
| BMI z-score | 2.1c | 2.0c | ||
| Sex | Male | 257 (58.4) | 1.7c | 1.7c |
| Female | 183 (41.6) | 1.0 | 1.0 | |
| Age group | School-aged children | 290 (65.9) | 1.5a | |
| Preschool-aged children | 150 (34.1) | 1.0 | ||
| Ultra-processed food intake | Consumed more than two times a week | 162 (36.8) | 1.0 ns | |
| Consumed two or less times a week | 278 (63.2) | 1.0 | ||
| Mother BMI | Overweight/obese | 153 (35.1) | 1.7b | |
| Underweight/normal weight | 283 (64.9) | 1.0 | ||
| Mother age | > 38 years (50th centile) | 212 (48.5) | 1.3a | |
| ≤ 38 years (50th centile) | 225 (51.5) | 1.0 | ||
| Mother education | < Completed college education | 60 (13.6) | 1.3a | |
| ≥ Completed college education | 380 (86.36) | 1.0 | ||
| Absence during child mealtime | One or more of the major meals of the week | 47 (10.68) | 1.2ns | |
| None of the major meals of the week | 393 (89.32) | 1.0 | ||
| Perceived responsibility for child feeding | Never/seldom/half of the time/most of the time | 124 (28.25) | 1.0ns | |
| Always | 315 (71.75) | 1.0 | ||
| Concern about child overweight | Concerned/fairly concerned/very concerned | 213 (48.41) | 1.1ns | |
| Unconcerned/a little concerned | 227 (51.59) | 1.0 |
OR, odds ratio; ns, not significant.
The primary aim of this study was to examine parental misperception of child weight status. In accordance with the predicted outcome, poor agreement was observed between parental weight status perception and children's actual BMI z-scores based on reported data. Specifically, we found that 48.05% of parents misclassified their child weight, with parents vastly more likely to underestimate (45.08%) than to overestimate (3%). Other studies using South American samples found a similar prevalence of parental misperception. A Chilean study reported underestimation in almost 54% of parents.9 However, two Brazilian studies, in Salvador and Goiás, reported lower prevalences of parental underestimation (18% and 29%, respectively)10,11; this could be due to the restricted response formats for parental weight perception used in these studies (three categories only), or the lower rates of overweight and obese children in these regions.2
Parental underestimation of child's weight status in the present sample occurred more often among overweight, obese, and extremely obese children (92.51%), with only a quarter of parents underestimating the weight status of their normal weight children. A high prevalence of underestimation among overweight/obese children was also reported in a Mexican study.8 In a recent meta-analysis, which calculated adjusted effect sizes, 51% of parents underestimated the weight of their overweight/obese children, while the weight of normal weight children was underestimated in 14% of the cases.12 However, most of the studies found lower rates of parental underestimation of overweight/obese children.16,26
Notably, the Mexican study evaluated maternal perceptions of child weight status using both a question, and silhouette picture scale, and found that mothers underestimate more when answering a question.8 The higher prevalence of maternal underestimation in the present sample may therefore arise from the fact that a question was used rather than a picture scale. Other reasons for discrepancies across studies could include not only across-study variation in the tools used to evaluate parental perceptions of child weight status, but also in child and parent age groups, and in cultural and social backgrounds. Importantly, the perception of what is a healthy weight seems to be changing in modern society, such that children who would previously have been classified as overweight may now be viewed by their family and the society as ‘normal’ weight.8,27 This is likely related to the increasing prevalence of childhood overweight across countries, especially in Brazil,2 and it is consistent with an instance of social comparison theory such that parents assess their child's weight in comparison to their peers, not according to an absolute scale.17
Evidence suggests that parents may underestimate their child weight because they believe that a heavier child is healthier,27 despite the fact that overweight, as well as underweight, are associated with health consequences.10 In addition, mothers may consider physical limitations, eating habits and social consequences when evaluating childhood overweight, i.e., as long as their child is active, has a good appetite and eats healthy foods, and is not teased about his or her size, they consider them to be healthy and are not concerned about their weight.7 All these factors are considered symptoms, which are what encourage parents to seek professional assistance, while excessive weight could be a sign detected by health professionals only. To summarize, it appears that parents may not see what health professionals see, and only seek professional help when childhood obesity is severe.28
After performing univariate analyses, eligible variables were included in a multiple logistic regression model adjusted for child's age, mother's age, education, and BMI. The remaining independent determinants of parental underestimation of child weight status were child BMI and male sex. For child weight, it was observed that the chance of underestimating doubled for every point of BMI z-score. A similar result was reported in another study, which showed a 1.49-fold greater likelihood of underestimating for each BMI z-score point.14 A recent study in Brazil also found a greater risk of underestimation of child weight for overweight children (PR=2.52).10 A study from the United States additionally found that the ability to correctly identify their child weight status was lower among parents of children with overweight or risk for overweight, as compared to normal weight children.29
The finding that male children are more at risk for underestimation (OR=1.67) is consistent with the results of one Brazilian19 and one Greek study,14 although another Brazilian study found no association between these variables.10 The tendency of parents to underestimate sons’ more than daughters’ weights may be related to gender differences in body composition, but could also reflect social norms such that girls are pressured to have a smaller body size, while larger bodies in boys are seen as more acceptable, even conferring a physical advantage.10,14
Several limitations should be taken into consideration when interpreting the current findings. First, the cross-sectional design does not allow causal inference, so interpretation of the associations should be made with caution. Second, a question about perceived child weight was used rather than a silhouette rating scale, which may increase misperception rates.8 However, the question had six possible responses, and allowed parents to classify children as only mildly different from normal weight, thus increasing the likelihood of correct classification. Third, child height and weight were reported by the parent, potentially introducing inaccuracy and bias, which could result in imprecise information. However, self-reported data are often necessary in large samples, for economic and logistical reasons. Further the majority (about 70%) of the anthropometric information provided by parents was derived from pediatrician/medical reports or measured at home (data not shown), and parents of children of this age group are likely to be more aware of child's anthropometrics due to contact with health professionals for checks on development.30 Additionally, the fact that such high rates of misperception were observed, despite potential underestimation of reported weights due to reporting bias, testifies to the strength of the misperception effect. Child BMI is not the most accurate measure of adiposity; however, it is highly correlated with more direct measures of adiposity. The terms ‘normal weight’ or ‘about the right weight’ may not fully capture parents’ evaluations of their child's weight in terms of health etc., as their own weight status, peers and media exposure could influence what they consider those terms to mean; however, the majority of studies of parental perception of child weight have used this terminology.9,14,17 Although external validity was compromised by the homogeneity of the sample, who were generally high regarding parental income and education, the results were impressively similar to those in populations with lower levels of these characteristics. Finally, the use of the words ‘very’, ‘too,’ or ‘extremely’ may have discouraged parents to choose these options.
This study also had significant strengths. The large sample size allowed the statistical detection of poor agreement between parental perception of child weight status and child weight status, and robust estimates of associations. This investigation adds to a very small body of studies in the Brazilian population about parental perception of child weight status. The Southeast of Brazil, where this study was conducted, is the most developed region in the country; the increasingly Westernized, obesogenic food environment justifies the need of research in this particular area. Unlike other studies, this study comprises both preschool and school-aged children, and uses the most recent and appropriate growth standards for children.22
Parents are potential ‘agents of change’ for child obesity and their awareness of children's health and weight problems may form a first step to improve lifestyle. However, a recent study found that children who were accurately perceived as overweight at age four were not protected against weight gain at age 13.18 This suggests that accurate weight perception alone is not sufficient to prevent overweight and obesity. The transtheoretical framework, which is recommended as a way to educate parents via health care providers,15 suggests that the process for health behavior change occurs in five stages, starting with parental awareness and information before going through the stages in order to encourage long lasting results. However, information about health and nutrition has to be simplified to reach parents optimally. Potential ways of doing this are through family-based interventions, starting in early childhood,31 or, since these are often not available, at pediatric visits occurring for the first two years of life.29 Since outpatient clinics are less frequently visited by older children, continuation of medical consultations incorporating exposure to nutritional and health education may be a useful intervention.
To conclude, this study revealed that almost half of parents in a Brazilian sample of parents underestimated their preschool or school aged child's weight status, and that risk of underestimation was higher for older children and male children. Clinical practitioners should therefore focus interventions to assist parents to correctly evaluate their child weight status on male children with higher BMIs. Parental awareness of weight issues in children could form a vital first step toward promotion of healthy environments and lifestyles, and prevention and treatment for childhood obesity.
Conflicts of interestThe authors declare no conflicts of interest.
Data collection was performed at schools in Campinas and São Paulo, SP, Brazil. The authors thank the participating schools, parents, and children for their valuable contribution. They also thank the CAPES for scholarships for LAM and SW, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK; Grant No. R00DK088360) for funding for SC, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and Office of the Director, National Institutes of Health (OD) under Grant No. U54HD070725 to the Global Obesity Prevention Center (GOPC) at Johns Hopkins for funding for SC, and the Conselho Nacional de Pesquisa (CNPq) for a productivity scholarship for JAACT.
Please cite this article as: Warkentin S, Mais LA, Latorre MR, Carnell S, Taddei JA. Factors associated with parental underestimation of child's weight status. J Pediatr (Rio J). 2018;94:162–169.




