
There is a lack of data on the association between body self-perception and eating patterns in Brazil. Thus, this study aimed to explore the relationship between body image dissatisfaction and eating patterns by the anthropometric status in adolescents.
MethodsA cross-sectional study of 1496 adolescents was conducted. The participants completed the Body Shape Questionnaire. Demographic, anthropometric, and socioeconomic data were collected, as well as information regarding the pubertal development and dietary intake. Logistic regression was performed to evaluate the associations of interest.
ResultsBody image dissatisfaction was identified in 19.5% of the adolescents. Three dietary patterns were identified: (1) the Western pattern was composed of sweets and sugars, soft drinks, typical dishes, pastries, fast food, beef, milk, and dairy products; (2) the Traditional pattern was composed of oils, chicken, fish, eggs, processed meat products, cereals (rice, cassava flour, pasta, etc.), baked beans, and bread; and (3) the Restrictive pattern was composed of granola, roots, vegetables, and fruit. Among overweight/obese adolescents, the data indicated a negative association of slight body image dissatisfaction (OR: 0.240 [0.100; 0.576]) and moderate body image dissatisfaction (OR: 0.235 [0.086; 0.645]) with the Western dietary pattern. Additionally, in this group, there was a positive association between high body image dissatisfaction and the Restrictive pattern (OR: 2.794 [1.178; 6.630]).
ConclusionAmongst overweight/obese adolescents, those with slight and moderate body image dissatisfaction were less likely to follow a Western-like dietary pattern when compared with those satisfied with their body image. Additionally, in this group, adolescents with high body image dissatisfaction was more likely to follow a restrictive pattern.
Há poucos dados sobre a associação entre autopercepção corporal e padrões alimentares no Brasil. Assim, este estudo teve como objetivo explorar a relação entre insatisfação com a imagem corporal (IIC) e padrões alimentares de acordo com o estado antropométrico em adolescentes.
MétodosUm estudo transversal com 1.496 adolescentes foi conduzido. Os participantes preencheram o Questionário de Imagem Corporal. Dados demográficos, antropométricos e socioeconômicos foram coletados, bem como informações relacionadas ao desenvolvimento puberal e ao consumo alimentar. Foi realizada uma regressão logística para avaliar as associações de interesse.
ResultadosA IIC foi identificada em 19,5% dos adolescentes. Três padrões alimentares foram identificados: (1) O padrão Ocidental, composto de doces e açúcares, refrigerantes, pratos típicos, artigos de pastelaria, fast food, carne bovina, leite e laticínios, (2) o padrão Tradicional, composto de óleos, frango, peixe, ovos, produtos de carne processada, cereais (arroz, farinha de mandioca, massas, etc.), feijão cozido e pão e (3) o padrão Restritivo, composto de granola, raízes, verduras e frutas. Entre adolescentes acima do peso/obesos, os dados indicaram uma associação negativa entre IIC leve [RC=0,240 (0,100; 0,576)] e IIC moderada [RC=0,235 (0,086; 0,645)] e padrões alimentares Ocidentais. Além disso, nesse grupo, houve uma associação positiva entre a IIC grave e o padrão Restritivo [RC=2,794 (1,178; 6,630)].
ConclusãoEntre adolescentes acima do peso/obesos, aqueles com IIC (leve e moderada) apresentaram menor probabilidade de seguir um padrão alimentar Ocidental em comparação aos satisfeitos com sua imagem corporal. Além disso, nesse grupo, adolescentes com IIC grave apresentaram maior probabilidade de seguir um padrão Restritivo.
Obesity has become a major nutritional problem in the modern world, and its incidence increasing rapidly in both developed and many developing countries.1 In Brazil, national surveys conducted over recent decades have also shown an increase in overweight and obesity in Brazilian adolescents, suggesting an epidemic trend. The Household Budget Survey, conducted in Brazil in 2008/2009, estimated that approximately 20% of 10–18-year-olds were overweight.2 Adolescent obesity is associated with significant immediate and long-term health risks; it also predicts obesity in adulthood and increased risk of adult morbidity and mortality.3
In a society where most adults and a significant proportion of children and adolescents are overweight and attempting to lose weight, it is not surprising that weight concerns and body dissatisfaction are common. Body image is considered a multifaceted construct that involves an individual's perceptions, thoughts, feelings, and behaviours about the size, shape, and structure of his/her body.4 Within the adolescent population, a negative body image perception and poor self-esteem may result in health-related effects, such as depressive symptoms and greater risk of clinical eating disorders.5 Previous studies indicate that the prevalence of body image dissatisfaction (BID) in developed countries ranges between 35% and 81% among female adolescents and between 16% and 55% among male adolescents.6 In Brazil, the results from the National Survey of School Health (Pesquisa Nacional de Saúde do Escolar [PeNSE]) show that more than 38% of the adolescents did not consider their body as normal.7 Over 15% of the students reported adopting extreme weight control practices, combining practices to lose or gain weight. Adolescents who considered themselves fat presented with a frequency of extreme practices for weight loss that was 92% higher than that shown by individuals who considered themselves to have a normal weight.7
Overall, the current results highlight the importance of body image for adolescent nutritional habits and food choices.8,9 Individuals who show body dissatisfaction are less likely to engage in healthy weight management behaviours; instead, they are more likely to adopt behaviours that may place them at risk for weight gain and poorer overall health.10–12 The adoption of diet restriction rather than eating healthier food as a method to lose weight among those with a negative body image perception has been demonstrated in the literature.10,12 Moreover, there is a lack of data on the association between body self-perception and eating patterns according the anthropometric status in adolescents.10 Given the lack of Brazilian adolescent studies linking body perceptions with diet, and the general lack of studies focusing on dietary patterns, supplementary studies would be useful to improve knowledge on this subject. The hypothesis tested in the present study was that adolescents are particularly vulnerable to adopting a restricted diet when they experience a negative body image perception, which is aggravated in overweight/obesity adolescents. Thus, this study aimed to explore the relationship between BID and dietary patterns with the anthropometric status in adolescents, in a population from Salvador, Bahia. The present findings will better inform pediatricians and other health care professionals about potential issues around body weight and weight control practices in adolescents.
Materials and methodsThis study consisted of a population-based, cross-sectional dietary survey performed in 2009 in the city of Salvador, the capital of the state of Bahia, Brazil. To estimate the sample size, data supplied by the Bahia State Education Department for the 2007 school year, the most recent available at the time, were used, assuming a BID prevalence of 18.8%.13 Therefore, for a confidence level of 95% and maximum admissible error of 2.5%, a minimum of 1201 students would be required for this study. Overall, 1561 students were evaluated. A detailed description of the sample is provided elsewhere.14 After reviewing the questionnaires and excluding 67 cases due to inconsistent data, the final sample included 1496 students, which is well above the minimum number defined as necessary to investigate BID.
Data were collected between July and December 2009 in the selected schools by ten interviewers who were trained and qualified to conduct the study activities. The parents or guardians who agreed to their child's participation signed an informed consent form. In the case of illiterate parents or guardians, consent was given by providing a fingerprint. The informed consent was obtained from the schools. The internal review board of the Institute of Collective Health, Federal University of Bahia approved the study protocol (No. 002/08).
Instruments and measuresDietary patternsThe Food Frequency Questionnaire (FFQ) recently validated for the Brazilian population by Mascarenhas et al.15 The FFQ consists of 97 food items with the following possible answers for consumption: (a) never/seldom, (b) one to three times a month, (c) once a week, (d) two to four times a week, or (e) ≥ four times a week (for this answer, the number of times per day was also recorded). Daily intake frequency was calculated based on the weekly and monthly consumption of each food.
For the analysis, the foods were grouped into the following 19 food clusters according to the coded nutritional content: sugars and sweets, typical Brazilian dishes, pastries, soft drinks, fast food, oils, milk and dairy products, beef, chicken, fish, eggs, processed meat products, cereals (rice, cassava flour, and pasta), granola, roots, baked beans, bread, vegetables, and fruit. Typical Brazilian dishes were: feijoada (a stew of black beans with beef and pork), feijão tropeiro (a dish made with beans, cassava flour, sausage, garlic, onion, bacon, and eggs), and acarajé (a dish made from peeled black-eyed peas, which are shaped into balls and deep fried in palm oil).
Body imageThe Body Shape Questionnaire (BSQ)16 was used to identify various aspects of dissatisfaction or concern with weight and body image in the four weeks prior to the interview. The BSQ consists of 34 items rated on a Likert-type scale, ranging from 1 to 6. Based on their scores, the adolescents were classified into one of the following groups: satisfied with their body image (scores≤80); slightly dissatisfied (scores from 81 to 110); moderately dissatisfied (scores from 111 to 140); or highly dissatisfied (scores>140). The BSQ had already been translated into Brazilian Portuguese17 and validated for use in Brazilian adolescents.18 The Cronbach's alpha coefficient (a) was 0.96, and this was independent of sex. The internal consistency in the current study was 0.95. This scale was correlated with body mass index (BMI) in the validation study sample (r=0.41, p<0.01).18
Anthropometric dataParticipants were weighed on a portable digital scale (Master Balanças®, GO, Brazil), and their height was measured using a Leicester Height Measure® portable stadiometer (Seca, Hamburg, Germany). The weight of the uniform (100g) was subtracted during the analysis. WHO reference tables (2007)19 with percentile values of the body mass index (BMI=weight [kg]/height [m2]) were used to assess the anthropometric status according to age and sex. For classification to an anthropometric status, the 2006 WHO criteria was used20: underweight (<3rd percentile), normal weight (≥3rd percentile and <85th percentile, the reference category), overweight (≥85th percentile and <97th percentile), or obese (≥97th percentile). The overweight and obese categories were grouped; therefore, overweight/obese children were those at or above the 85th percentile.
Other variablesThe participants’ dates of birth were obtained from the school records. Age was dichotomized into <14 years, the reference category, or ≥14 years. To classify the socioeconomic conditions of each family, the Brazilian Criteria for Economic Classification (BCEC) was used.21 These criteria included the education level of the head of the family and number of family members with a regular job, as well as nine other items related to material goods.21 For the purpose of this analysis, families were grouped into better socioeconomic status (8–27 points; the reference category) or worse socioeconomic status (0–7 points). The cut-off points were determined by the BCEC.21 Pubertal development was established by assessing participants’ male or female sexual characteristics, as well as age at menarche in the case of girls.22 In accordance with this staging system, adolescents were grouped as prepubescent, pubescent (the reference category), or post-pubescent. These stages were self-reported by the participants, based on reference images provided by the interviewers.
Statistical analysisThe Epi Info software, version 6.04 (Centers for Disease Control and Prevention – Atlanta, USA), was used to construct the database and conduct the analyses. Data were entered in duplicate after all questionnaires had been reviewed and any coding errors had been corrected. The characteristics of the population were identified by descriptive analysis, and the prevalence of the categorical variables was calculated. Before proceeding to the exploratory factor analysis (EFA), the Kaiser-Mayer-Olkin coefficient (KMO) was estimated, and Bartlett's sphericity test was used to indicate the adequacy of the data analysis. Factor analysis with principal component estimation followed by an orthogonal rotation (varimax) was used for the exploratory factor structure (pattern) analysis. To identify the number of principal components to be retained, the following criteria were used: eigenvalues exceeding 1, scree plot (which is a graphical presentation of eigenvalues), and interpretability of each component.23 The derived factors were labelled based on the data and on a literature review. The factor score for each pattern was calculated by summing intakes of food groups weighted by their factor loadings, and each participant received a factor score for each identified pattern. Food groups with factor loadings greater than 0.40 and communality over 0.20 were retained in the identified patterns.24 The scores of each consumption pattern were dichotomised as percentile >75th versus percentile ≤75th.
A logistic regression model considering the complex survey design was used to examine the relationship between BID and dietary pattern. Analysis was stratified according to anthropometric status (BMI). The magnitude of the association was assessed by logistic regression and expressed by odds ratios (OR) with 95% confidence intervals (95% CI). The models were adjusted for sex, age, sexual development, and economic conditions. The choice of confounding variables for modelling was based on data published in the literature.8–12 The statistical tests were two-tailed, with a 5% significance level. Statistical analyses were corrected according to a complex sample design using the STATA commands STATA (Software de Estatistica: Version 13. College Station, TX, USA).
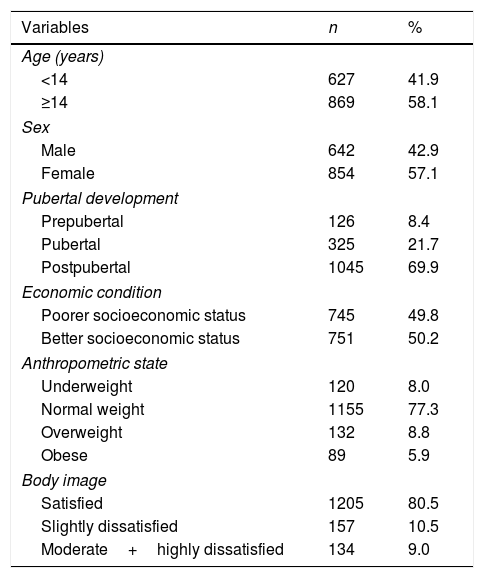
ResultsOverall, 1496 students with complete sets of data were included in the analysis. There was a slightly higher percentage of girls (57.1%) when compared with boys. Regarding the anthropometric status, most students (77.2%) who belonged to the group were considered to be of normal weight, whereas 14.7% were classified as overweight/obese and 8.0% as underweight. BID was identified in 19.5% of the students. Nearly 50.0% of the study participants were classified as belonging to the poorest socioeconomic class. According to the classification system used, no individuals were classified in the highest income strata (A) (Table 1).
Demographic, economic, biological, and behavioral data of students enrolled in public schools in Salvador, Bahia, Brazil, 2009 (n=1496).
| Variables | n | % |
|---|---|---|
| Age (years) | ||
| <14 | 627 | 41.9 |
| ≥14 | 869 | 58.1 |
| Sex | ||
| Male | 642 | 42.9 |
| Female | 854 | 57.1 |
| Pubertal development | ||
| Prepubertal | 126 | 8.4 |
| Pubertal | 325 | 21.7 |
| Postpubertal | 1045 | 69.9 |
| Economic condition | ||
| Poorer socioeconomic status | 745 | 49.8 |
| Better socioeconomic status | 751 | 50.2 |
| Anthropometric state | ||
| Underweight | 120 | 8.0 |
| Normal weight | 1155 | 77.3 |
| Overweight | 132 | 8.8 |
| Obese | 89 | 5.9 |
| Body image | ||
| Satisfied | 1205 | 80.5 |
| Slightly dissatisfied | 157 | 10.5 |
| Moderate+highly dissatisfied | 134 | 9.0 |
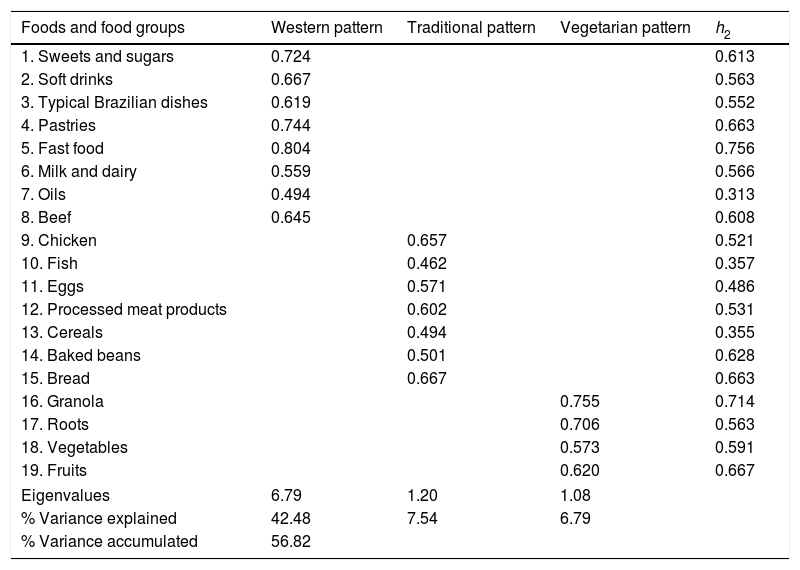
Both the KMO index (0.942) and Bartlett's test (χ2=11,247.656; p<0.001) indicated that the correlation among the variables was sufficiently strong for a factor analysis. To reduce bias from multiple testing and better identify common dietary patterns, only the dietary patterns with an eigenvalue of >1.08 were extracted. The choice of the number of factors was first based on the Kaiser criterion, namely eigenvalues over 1.0. This is the most frequently used criterion in factor analysis, and the theoretical basis behind it is that each retained factor should explain more variance than the original variable in the data set. Factor determination was also based on the eigenvalue plot (scree plot), which plots the total variance associated with each factor.
Factor analysis revealed three eating patterns that were responsible for 56.82% of the total variance. These eating patterns were termed Western, Traditional, and Restrictive. The factor loadings of the eating patterns for each component are shown in Table 2. The first component was positively correlated with the intake of sweets and sugars, soft drinks, typical Brazilian dishes, pastries, fast food, beef, milk and dairy products. The second component was positively correlated with oils, chicken, fish, eggs, processed meat products, cereals (rice, cassava flour, pasta, etc.), baked beans, and bread. The third component was positively correlated with granola, roots, vegetables, and fruit.
Distribution of the factor loadings for the food consumption patterns of students enrolled in public schools in Salvador, Bahia, Brazil, 2009.
| Foods and food groups | Western pattern | Traditional pattern | Vegetarian pattern | h2 |
|---|---|---|---|---|
| 1. Sweets and sugars | 0.724 | 0.613 | ||
| 2. Soft drinks | 0.667 | 0.563 | ||
| 3. Typical Brazilian dishes | 0.619 | 0.552 | ||
| 4. Pastries | 0.744 | 0.663 | ||
| 5. Fast food | 0.804 | 0.756 | ||
| 6. Milk and dairy | 0.559 | 0.566 | ||
| 7. Oils | 0.494 | 0.313 | ||
| 8. Beef | 0.645 | 0.608 | ||
| 9. Chicken | 0.657 | 0.521 | ||
| 10. Fish | 0.462 | 0.357 | ||
| 11. Eggs | 0.571 | 0.486 | ||
| 12. Processed meat products | 0.602 | 0.531 | ||
| 13. Cereals | 0.494 | 0.355 | ||
| 14. Baked beans | 0.501 | 0.628 | ||
| 15. Bread | 0.667 | 0.663 | ||
| 16. Granola | 0.755 | 0.714 | ||
| 17. Roots | 0.706 | 0.563 | ||
| 18. Vegetables | 0.573 | 0.591 | ||
| 19. Fruits | 0.620 | 0.667 | ||
| Eigenvalues | 6.79 | 1.20 | 1.08 | |
| % Variance explained | 42.48 | 7.54 | 6.79 | |
| % Variance accumulated | 56.82 | |||
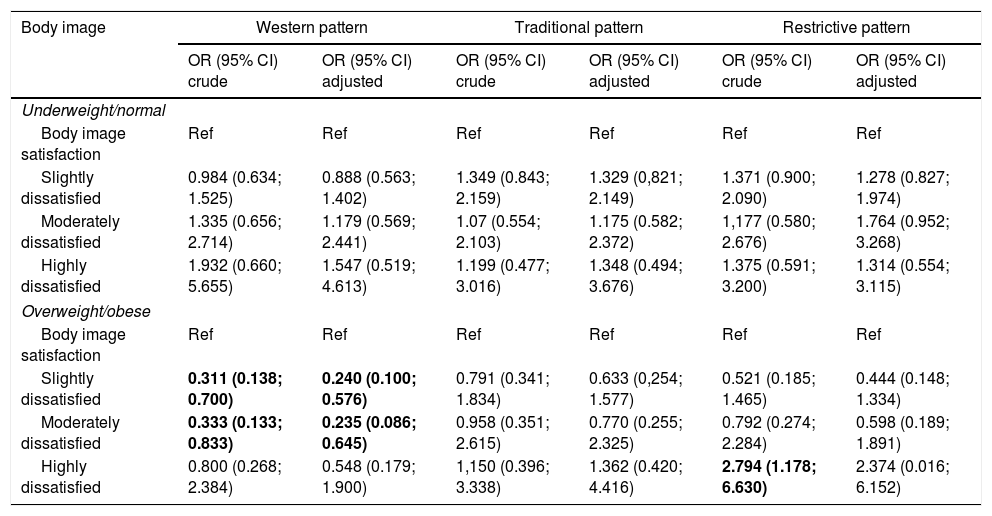
An analysis was conducted to explore the relationship between BID and eating patterns by anthropometric status. The models were analysed by multivariate unconditional logistic regression adjusted for sex, age, sexual development, and economic conditions. In overweight/obese adolescents, there was a significant negative association of slightly BID (OR: 0.240 [0.100; 0.576]) and moderate BID (OR: 0.235 [0.086; 0.645]) with the standard Western pattern. Additionally, in this group, there was a positive association of high BID with the Restrictive pattern (OR: 2.794 [1.178; 6.630]). Moreover, BID was not associated with any dietary pattern among underweight or normal weight adolescents, even after the appropriate adjustments were made (Table 3).
Logistic regression for evaluating the relationship between body image dissatisfaction and eating patterns of students enrolled in public schools in Salvador, Bahia, Brazil, 2009.
| Body image | Western pattern | Traditional pattern | Restrictive pattern | |||
|---|---|---|---|---|---|---|
| OR (95% CI) crude | OR (95% CI) adjusted | OR (95% CI) crude | OR (95% CI) adjusted | OR (95% CI) crude | OR (95% CI) adjusted | |
| Underweight/normal | ||||||
| Body image satisfaction | Ref | Ref | Ref | Ref | Ref | Ref |
| Slightly dissatisfied | 0.984 (0.634; 1.525) | 0.888 (0.563; 1.402) | 1.349 (0.843; 2.159) | 1.329 (0,821; 2.149) | 1.371 (0.900; 2.090) | 1.278 (0.827; 1.974) |
| Moderately dissatisfied | 1.335 (0.656; 2.714) | 1.179 (0.569; 2.441) | 1.07 (0.554; 2.103) | 1.175 (0.582; 2.372) | 1,177 (0.580; 2.676) | 1.764 (0.952; 3.268) |
| Highly dissatisfied | 1.932 (0.660; 5.655) | 1.547 (0.519; 4.613) | 1.199 (0.477; 3.016) | 1.348 (0.494; 3.676) | 1.375 (0.591; 3.200) | 1.314 (0.554; 3.115) |
| Overweight/obese | ||||||
| Body image satisfaction | Ref | Ref | Ref | Ref | Ref | Ref |
| Slightly dissatisfied | 0.311 (0.138; 0.700) | 0.240 (0.100; 0.576) | 0.791 (0.341; 1.834) | 0.633 (0,254; 1.577) | 0.521 (0.185; 1.465) | 0.444 (0.148; 1.334) |
| Moderately dissatisfied | 0.333 (0.133; 0.833) | 0.235 (0.086; 0.645) | 0.958 (0.351; 2.615) | 0.770 (0.255; 2.325) | 0.792 (0.274; 2.284) | 0.598 (0.189; 1.891) |
| Highly dissatisfied | 0.800 (0.268; 2.384) | 0.548 (0.179; 1.900) | 1,150 (0.396; 3.338) | 1.362 (0.420; 4.416) | 2.794 (1.178; 6.630) | 2.374 (0.016; 6.152) |
Adjusted by gender, age, sexual maturation, and economic classification
Bold values are statistically significant.
The adolescents included in the present study were grouped into the following three dietary categories according to their dietary pattern, as identified through the EFA method: (1) the Western pattern consisted of sweets and sugars, soft drinks, typical Brazilian dishes, pastries, fast food, beef, milk, and dairy products; (2) the Traditional pattern consisted of oils, chicken, fish, eggs, processed meat products, cereals (rice, cassava flour, pasta, etc.), baked beans, and bread; and (3) the Restrictive pattern consisted of granola, roots, vegetables, and fruit. The Western dietary pattern appeared to reflect the patterns already reported in another study on food consumption in the Brazilian population.25 The adoption of the Western pattern reflects the lifestyle changes experienced by Brazilian families in recent years, including eating out, as well as increase consumption of fast and processed foods.
This study aimed to explore the relationship between BID and dietary patterns with anthropometric status. A logistic regression analysis was conducted, adjusting for the age, sex, pubertal development, and socioeconomic classification. This study found that, among overweight/obese adolescents, those with slight and moderate BID were less likely to follow a Western-like dietary pattern when compared with those who were satisfied with their body image. Additionally, in this group, individuals with high BID were more likely to follow a Restrictive pattern.
A negative association was observed between dissatisfaction with current body image and the Western dietary pattern among overweight adolescents, reinforcing the findings from other studies in individuals from a similar age range.12,26 A study of Massachusetts high school students found that adolescents attempting to lose weight consumed fewer servings of fatty foods, but failed to increase their fruit and vegetable intake.12 To lose weight, they also ate fewer desserts, whereas those who wished to gain weight ate more servings of these foods. Evaluation studies of the relationships between BID and dietary patterns usually observe that overweight adolescents with BID eat more health-promoting foods, such as fruit, vegetables and fish, but they reported eating fewer high fat, sugar-containing snack foods.12,26 These findings from these studies indicated that, in general, lower body satisfaction does not serve as a motivator for engaging in healthy weight management behaviours; rather, it appears to predict behaviours that may place adolescents at risk for weight gain and poorer overall health. The adoption of restrictive diets is a behavioural phenomenon that is becoming more frequent among adolescents, and the search for weight loss through dieting may result in an unbalanced nutrition, both quantitatively and qualitatively.27
As previously shown, restriction diets are an inappropriate dietary behaviour and do not prevent obesity.12,26 Those individuals have a higher BMI and they have more difficulties in maintaining a correct body mass. The mechanisms by which a restricted calorie diet in individuals with BID can lead to a gain in excess weight have not been clearly elucidated. It is hypothesized that obesity may be the source of stress, which reinforces obesity by increasing body mass28; in turn, dissatisfaction with one's body image may act as a spur to alter body mass.28 This could explain why the attempt to diet is more frequent and the adoption of restriction diets is more common in obese individuals.29 Nevertheless, restriction diets can result in excess body mass. When constant attention to limiting food consumption fails, individuals fall prey to temptation, and overeating may occur.29
The present study also had some limitations that must be mentioned. These included its cross-sectional nature, which implies that the temporal sequence of events was not considered, making it impossible to determine causality. Longitudinal studies would provide a deeper understanding of the causal pathways involved. Furthermore, the nutritional intakes of adolescents estimated through this questionnaire might not represent their true intakes, as it might have been affected by recall bias and social desirability. However, it is an appropriate instrument for ranking dietary intakes. Additionally, it is suspected that individuals aware of the beneficial or harmful effects of particular foods may give distorted accounts of their consumption of these foods. In turn, the strengths associated with the present study are that (a) the collection of detailed data regarding the participants’ dietary consumption; (b) inclusion of both males and females, while previous studies on body image have mainly focused on girls; and (c) use of exploratory factor analysis with the main component estimation method to measure eating patterns.
Despite the limitations, the current results highlight the importance of body image for adolescent food choices. Among overweight/obese adolescents, those with slight and moderate BID were less likely to follow a Western-like dietary pattern when compared with those satisfied with their body image. Additionally, in this group, individuals with high BID were more likely to follow a Restrictive pattern. These findings support the importance of treatment and prevention of BID in overweight/obese adolescents to help change their eating patterns to healthier ones.
FundingFundação de Amparo à Pesquisa do Estado da Bahia (FAPESB) – Project No. 7638/2009.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Ribeiro-Silva RC, Fiaccone RL, Conceição-Machado ME, Ruiz AS, Barreto ML, Santana ML. Body image dissatisfaction and dietary patterns according to nutritional status in adolescents. J Pediatr (Rio J). 2018;94:155–161.




