

to estimate the prevalence of high blood pressure (BP) in schoolchildren, as well as the reported frequency of previous measurements of BP in these children, and to identify high BP risk markers in the sample.
Methodsthis was a cross-sectional study involving 794 children aged 6 to 13 years, enrolled in public elementary schools. A questionnaire was given to parents/guardians, consisting of perinatal, socioeconomic data, and information on previous measurements of BP in these children. Anthropometric measurements included weight, height, waist, hip, and arm and neck circumference, in addition to the three BP measurements. Classification of BP levels was carried out according to current international recommendations, established in 2004.
Resultsthe prevalence of high BP (hypertension or prehypertension) was 7%. Only 21.7% of children had previously undergone BP measurements. The odds ratio of high BP among children with and without overweight was 2.9 (95% CI=1.7 to 5.0, p<0.001). None of the anthropometric measurements was superior to the Z-score of BMI as a predictor of high BP. History of hypertension during pregnancy (p<0.001), prematurity (p=0.006), maternal hypertension (p=0.01), and paternal hypertension (p=0.008) were also correlated with the presence of high BP in children.
Conclusionsoverweight and family history constitute the main risk markers of high BP in children. The low frequency of BP measurement in children observed in this municipality contributes to the underdiagnosis of the disease, with irreversible consequences for these individuals.
estimar a prevalência de pressão arterial (PA) elevada em escolares, assim como a frequência relatada de aferição prévia da PA nessas crianças. Identificar marcadores de risco de PA elevada na amostra.
Métodosestudo transversal envolvendo 794 crianças de 6 a 13 anos, matriculadas no ensino público fundamental. Questionário entregue aos pais, com informações perinatais, sócio-econômicas e sobre aferição prévia da PA nas crianças. Avaliação antropométrica: peso, altura, circunferências abdominal, de quadril, braquial e cervical, além das três aferições da pressão arterial. Classificação dos níveis pressóricos conforme as recomendações internacionais atuais, estabelecidas em 2004.
Resultadosa prevalência de PA elevada (hipertensão ou pré-hipertensão) foi de 7%. Apenas 21,7% das crianças haviam sido previamente submetidas a aferições de PA. A razão de chances de PA elevada entre crianças com e sem excesso de peso foi de 2,9 (IC 95%=1,7 a 5,0, p<0,001). Nenhuma das medidas antropométricas foi superior ao Z de IMC como preditor de PA elevada. Histórico de hipertensão na gestação (p<0,001), de prematuridade (p=0,006), hipertensão materna (p=0,01) e hipertensão paterna (p=0,008) também se correlacionaram à presença de PA elevada nas crianças.
Conclusõesexcesso de peso e história familiar configuram como principais marcadores de risco de PA elevada em crianças. A baixa frequencia de aferição da PA observada em crianças deste município contribui para o subdiagnóstico da doença, com consequências futuras irreversíveis para esses indivíduos.
Systemic arterial hypertension (SAH) is considered a public health problem both in Brazil and worldwide. The early diagnosis and treatment of this disease are essential for reducing associated cardiovascular risks.
Until recently, SAH was considered nonexistent in the pediatric age range. Early studies of normal range blood pressure (BP) in children started in the late 1970s,1 and since then, several reviews have been performed.2–4 The currently used references were developed by The National High Blood Pressure Education Program of the United States in 2004, establishing the 50th, 90th, 95th, and 99th percentiles, adjusted according to gender, age, and height percentiles, and defining that values of systolic BP (SBP) and/or diastolic BP (DBP) are compatible with SAH when ≥ 95th percentile.4
It is estimated that over half of cases of SAH in children aged ≥ 7 years are of the essential type, and there is evidence that SAH in adults may have originated in childhood, thus contributing to the occurrence of early complications and adverse events in young adults.5,6 Additionally, complications such as left ventricular hypertrophy, hypertensive encephalopathy, and cerebrovascular accidents consequent to SAH have been reported even in the pediatric age range.7,8
Despite current recommendations for BP to be assessed annually from age 3 years,4 there is evidence that undervaluation and underdiagnosis are predominant in many health services in Brazil, resulting in irreversible future risks for these individuals.9,10
In the state of Espírito Santo, Brazil, data on the magnitude of the problem of high BP in children are scarce, and in the city of Vila Velha, they are absent. As a result, little or no attention has been given by the public health policies to this problem, whose worldwide impact is increasingly evident. Thus, the objectives of this study were to estimate the prevalence of elevated BP levels in children enrolled in primary schools in the city of Vila Velha, Brazil, to estimate the reported frequency of previous measurements of BP in these children, to identify anthropometric predictors associated with a higher risk of high BP, and to evaluate the presence of an association between high BP and socioeconomic, perinatal, and family characteristics in the sample.
MethodsThe study was approved by the Research Ethics Committee of the Universidade Vila Velha in October of 2011. It was a cross-sectional study of children enrolled in the municipal elementary school units (unidades municipais de ensino fundamental - UMEFs) of Vila Velha, the most densely inhabited city in the state of Espírito Santo, Brazil, in 2012. The first stage of sampling consisted of random selection, by drawing lots, of a school from each of the five political-geographical regions of the city. In the second stage, an unsystematic selection of students from each school was performed, according to their adherence to the study and consent from parents or guardians.
The unsystematic rather than random selection is justified by exhaustive attempts at randomization, which were abandoned due to the difficulty in obtaining informed consent from the parents or guardians. With the objective of obtaining greater homogenization of the sample in terms of age, children younger than 6 or older than 13 years, who accounted for less than 2% of the enrolled children, were excluded.
Sample size calculation was performed by using Statcalc Epi Info, release 6.04. The following were considered in the calculation: number of students enrolled in UMEFs in the study year, mean prevalence of SAH in children of 4%,11 absolute error of 2%, confidence interval of 95%, statistical power of 80%, and design effect of 2, resulting in 730 children. In order to account for eventual losses, the final number was rounded to 800.
The selected children underwent measurements of height, weight, and arm, abdominal, hip, and neck circumferences, in addition to BP measurements. All measurements were performed in duplicate or triplicate by the same team, trained in anthropometric techniques in order to control measurement and/or equipment reading errors.
Measurements of height were performed using a portable stadiometer graduated from 20 to 200cm, with scale accuracy of 0.1cm; the mean of three consecutive measurements was used. The child was placed in the standing position, without shoes, with hips and shoulders perpendicular to the central axis of the body, heels firmly planted on the ground, knees close together and extended, relaxed arms, and head in the Frankfurt plane. Body weight was determined through a digital anthropometric scale graded from 0 to 150kg with a resolution of 0.05kg. The body mass index (BMI) was calculated by the quotient of body mass in kg by height in meters squared (m2).
All circumference measurements were performed using an inelastic measurement tape. Abdominal circumference was measured as recommended by the I Brazilian guidelines for metabolic syndrome, halfway between the iliac crest and the lower costal margin. The hip measurement was performed in the horizontal plane, at the point of maximum circumference of the buttocks, with the individual in the standing position and feet placed together. The arm circumference was measured at midpoint between the acromion and the elbow, with the arm flexed at 90 degrees with the forearm. The neck circumference was measured having as reference a horizontal line at the level of half of the thyroid cartilage, with the neck in neutral position.12
BP was measured in the right arm with a cuff of appropriate size for the arm dimensions, with the child seated with the arm at the same level of the heart, according to the recommendations of the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents.4 After the child had remained at rest for 5min in the sitting position, three measurements were performed with a 3-minute interval between them. Initially, the measurement was performed by palpation, followed by measurements by auscultation using an aneroid sphygmomanometer.
For BP classification, the following were considered: age, gender, and height percentile, according to the National High Blood Pressure Education Program of the United States, established in 19872 and updated in 2004.4 Children with mean SBP and/or DBP ≥ the 95th percentile for gender, age, and height were classified as having SAH; children with mean SBP and/or DBP between the 90th and 95th percentiles or > 120/80mmHg were classified as pre-hypertensive; both groups were referred for medical assessment.
Socioeconomic, family, and perinatal variables possibly associated with the risk of high BP in children were assessed through written questionnaires given to parents or guardians, who provided information such as: hours per week of regular physical activity performed by the children, type of delivery, gestational age, weight and length at birth, duration of breastfeeding, age, weight, height, educational level and occupation of parents, family history of SAH, and total and per capita monthly family income. Additionally, parents or guardians were asked about the frequency of routine annual pediatric visits and the occurrence of prior assessment of BP in the child during these consultations.
For statistical analyses, measurements of height, weight, BMI and BP (systolic – SBP and diastolic – DBP) were converted to Z-scores (adjusted for gender, age and, in the case of BP, also adjusted for height percentile) according to international reference parameters.4,13
The sample was characterized regarding the distribution of gender, age, nutritional status, and other assessed variables. Association analyses were conducted by tests of correlation (Pearson or Spearman as appropriate), as well as by simple and multiple linear regression tests in order to estimate the independent influence of the predictor variables on outcomes. Both the adjusted levels of BP (BP Z-score, SBP and DBP) and the individual classification regarding BP levels as normal, borderline, or high, were used as dependent variables.
All statistical analyses were performed with SigmaStat for Windows (release 3.5, SPSS, Inc. - San Rafael, CA); p-values<0.05 were considered statistically significant.
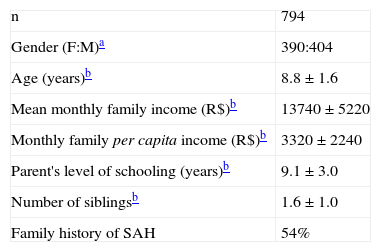
ResultsA total of 794 children were evaluated. The mean age of the students was 8.8±1.6 years. Gender distribution was 390 females (49.1%) and 404 males (50.9%). General, socioeconomic, and family characteristics of the sample are summarized in Table 1.
General, socioeconomic, and family characteristics of the sample of children aged 6 to 13 years from Vila Velha, ES, Brazil.
| n | 794 |
| Gender (F:M)a | 390:404 |
| Age (years)b | 8.8±1.6 |
| Mean monthly family income (R$)b | 13740±5220 |
| Monthly family per capita income (R$)b | 3320±2240 |
| Parent's level of schooling (years)b | 9.1±3.0 |
| Number of siblingsb | 1.6±1.0 |
| Family history of SAH | 54% |
SAH, systemic arterial hypertension.
Although 51.3% of parents reported routine visits to the pediatrician at least once a year, only 21.7% of the children had previously undergone BP measurements.
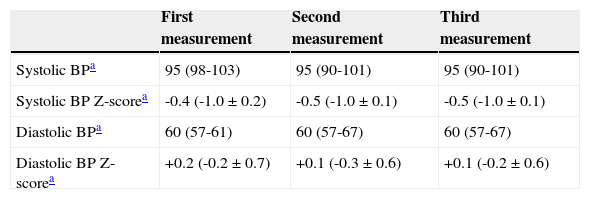
Based on the analysis adjusted for gender, age and height percentile, of the mean of three BP measurements, 7% (n=58) of the children were classified as having high BP, 4% (n=31) were compatible with the diagnosis of SAH, and 3% (n=27) were consistent with a diagnosis of pre-SAH. No significant differences were observed between the BP levels - absolute or Z-scores - when comparing the values obtained at the first, second, or third measurements (Table 2).
Blood pressure (BP) levels (absolute and adjusted for gender, age, and height as Z-scores) obtained during the first, second, and third measurements of BP in children aged 6 to 13 years from Vila Velha-ES.
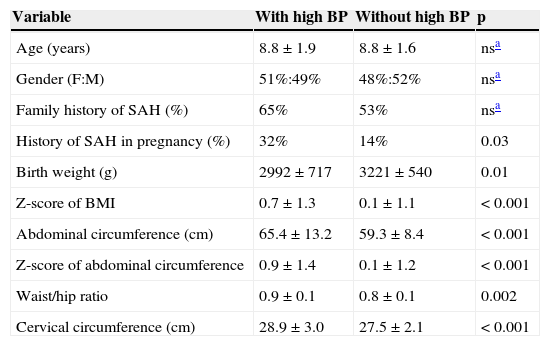
Regarding the nutritional status, 10.8% (n=85) were obese, 12.9% (n=102) were overweight, and 3.9% (n=30) were underweight. There was a strong association between the presence of overweight and high BP. Children with high BP had an average BMI Z-score 0.6 SD higher than children with Z-score of normal BP (95% CI: 0.3 to 0.9, p<0.001, Table 3). While 14% of overweight children had high BP, only 5% of children with normal weight showed abnormal BP levels (p<0.001). The odds ratio of high BP among obese or overweight children and children with normal or low weight was 2.9 (95% CI=1.7 to 5.0, p<0.001).
Distribution of independent variables in patients with and without high blood pressure (BP).
| Variable | With high BP | Without high BP | p |
|---|---|---|---|
| Age (years) | 8.8±1.9 | 8.8±1.6 | nsa |
| Gender (F:M) | 51%:49% | 48%:52% | nsa |
| Family history of SAH (%) | 65% | 53% | nsa |
| History of SAH in pregnancy (%) | 32% | 14% | 0.03 |
| Birth weight (g) | 2992±717 | 3221±540 | 0.01 |
| Z-score of BMI | 0.7±1.3 | 0.1±1.1 | < 0.001 |
| Abdominal circumference (cm) | 65.4±13.2 | 59.3±8.4 | < 0.001 |
| Z-score of abdominal circumference | 0.9±1.4 | 0.1±1.2 | < 0.001 |
| Waist/hip ratio | 0.9±0.1 | 0.8±0.1 | 0.002 |
| Cervical circumference (cm) | 28.9±3.0 | 27.5±2.1 | < 0.001 |
F:M, female:male; SAH, systemic arterial hypertension.
Although the circumferences of the abdomen, hip and neck have demonstrated the capacity to predict the presence of elevated BP (p<0.001), BMI Z-score showed a greater predictive capacity of predicting BP levels in these children, both for SBP (p<0.001, R2=0.06) and for DBP (p<0.001, R2=0.04) (Fig. 1).
 Z-score (A) and diastolic BP Z-score (B) in children aged 6 to 13 years from Vila Velha, ES, Brazil.")
Non-anthropometric variables significantly associated with the presence of high BP included maternal history of SAH during pregnancy (p<0.001), history of prematurity (p=0.006), maternal SAH (p=0.01) and paternal SAH (p=0.008). In addition, children with high BP showed significantly lower mean birth weight than children with normal BP (Table 3).
Multiple linear regression analyses using the Z-scores of BP as dependent variables demonstrated that when the variables associated with SAH were evaluated together, only the Z-score of BMI (p=0.02) and age (p=0.01) were significantly associated with the Z-score of SBP, whereas the independent predictors of DBP were Z-score of BMI (p=0.03), male gender (p=0.01), and family history of SAH (p=0.01). These predictive models were able to explain 8% of the variability of Z-score of the SBP and 10% of the variability of Z-score of DBP.
Multiple logistic regression using the presence or absence of high BP as the dependent variable, in turn, emphasized once again the important role of the presence of overweight (p<0.001, OR=6.4, 95% CI=2.2 to 18.7) and family history of SAH, particularly maternal SAH (p=0.008, OR=4.9, 95% CI=1.5 to 16.2) in determining risk of high BP in these children.
DiscussionSAH in children is a clinical condition that has been unacknowledged until recently, and it is often overlooked in clinical practice. Currently, the impact of early diagnosis is indisputable, both for the possibility of identifying secondary causes, as well as preventing its progression to adverse cardiovascular events. The public health problem is amplified due to the misconception by health professionals that this disease is rare in children, resulting in delayed diagnosis and lack of epidemiological data in most Brazilian cities.
The estimated prevalence in this sample, 7% of children with elevated BP, is significant and reinforces the idea that the disease is not as rare as previously thought. There are few studies in Brazil that evaluated this information based on the most recent criteria, established in 2004.14 Nevertheless, the available studies presented results that ranged from 2.7% to 13.8% in children aged 7 to 12 years, which is similar to that observed in the present study.11,14–16
The low frequency of previous measurements of BP in these children (21.7%) is noteworthy, which probably results in underdiagnosis, as suggested by other authors.11,17–19 It is likely related to factors such as underdiagnosis in the clinical setting, as well as the methodological complexity required for its diagnosis.19
Regarding risk markers, the importance of factors such as the presence of overweight and family history of SAH is noteworthy, which demonstrated consistent association with the presence of high BP in these children in the different analyses. Although the identification of these markers may not be reproducible in other populations, and are far from explaining the complex etiopathogenesis of this disorder, it is important that health professionals are aware of their presence to identify children especially susceptible to the disease.
The findings regarding the association between low birth weight and risk of high BP in this sample corroborate those of recent studies, which show an inverse association between birth weight and future cardiometabolic risk in general. Although the mechanism of this association is yet to be clarified, it is believed that it may be attributable to epigenetic fetal reprogramming mechanisms, in which the fetus alters certain physiological set points in response to an adverse intrauterine environment caused by a number of situations, such as maternal malnutrition, gestational hypertension, smoking, and others.20
Regarding anthropometric markers of risk, it is believed that parameters representative of the fat distribution pattern, such as abdominal circumference, waist-hip ratio, and cervical circumference, could add information to the isolated assessment of BMI, as central distribution of fat is the variable most correlated with cardiovascular risk.18,21,22 In the present sample, although all these parameters were useful as risk markers for high BP, none was shown to be superior to BMI Z-score, and all of them were directly related to this parameter, with no independent influence when analyzed by multiple linear regressions.
In conclusion, the presence of high BP in children is not as rare as previously thought, and overweight children, and those with positive family history and/or low birth weight deserve increased attention regarding the risk of disease. Low medical adherence to current recommendations for routine assessment of BP in children older than 3 years is an issue that deserves special attention from public health policies, since it allows for underdiagnosis with possible irreversible consequences for these individuals.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the principals, teachers, school employees, and parents and guardians of public school students who gave their consent for the conduction of this study.
Please cite this article as: Fuly J, Giovaninni NP, Marcato DG, Alves ER, Sampaio JD, Moraes LI, et al. Evidence of underdiagnosis and markers of high blood pressure risk in children aged 6 to 13 years. J Pediatr (Rio J). 2014;90:65–70.
Study conducted at Universidade Vila Velha - ES (UVV-ES), Vitória, ES, Brazil.




