
To describe the current scientific knowledge on the effects of physical exercise on the growth of children and adolescents since intrauterine life.
Source of dataA search was carried out in the Medline, Embase, Scielo, and Cochrane databases of studies published from 1990 to 2018. The authors included studies with different designs: clinical trials, cohort, cross-sectional and review studies.
Synthesis of dataStudies that addressed the subject of physical exercise or physical activity, and weight–height growth or bone or muscle tissue growth were identified. These studies were analyzed, classified, and presented by age group: fetuses, preterm newborns, preschoolers, schoolchildren, and adolescents. It was observed that almost all studies indicated the safety of physical exercises, of mild to moderate intensity, for pregnant women, as well as children and adolescents, including both aerobic and anaerobic exercises. The retrieve studies did not demonstrate that the practice of physical exercises or certain sports, especially basketball and floor gymnastics, influenced the linear growth of children or adolescents. Some studies showed an increase in bone and muscle tissue growth in child and adolescent athletes.
ConclusionsDespite the small number of studies with adequate methodology, especially randomized clinical trials, evidence appears to indicate that physical exercise is safe for both the pregnant woman and the child, from fetal life to adolescence. Physical exercise does not appear to impair the child's linear growth and contributes to the ideal shaping of bone and muscle tissues, ensuring possible beneficial effects throughout life.
Descrever o conhecimento científico atual sobre os efeitos do exercício físico no crescimento das crianças e adolescentes desde a vida intrauterina.
Fonte dos dadosPesquisa nas bases de dados, Medline, Embase, Scielo e Cochrane que envolveu estudos publicados desde 1990 até 2018. Foram incluídos estudos com diferentes desenhos: ensaios clínicos, coorte, transversais e revisões.
Síntese dos dadosForam identificados estudos que abordaram o tema, exercício físico ou atividade física e crescimento pondero-estatural ou dos tecidos ósseo ou muscular. Os estudos foram analisados, classificados e apresentados por faixa etária: fetos, recém-nascidos pré-termos, pré-escolares, escolares e adolescentes. Observou-se que quase todos todos os apontaram para a segurança do exercício físico de leve a moderada intensidade, tanto para a gestante como para a criança e o adolescente, inclusive tanto os exercícios aeróbicos como os anaeróbicos. Os estudos identificados não comprovaram que a prática de exercícios físicos ou determinados esportes, em especial o basquete e a ginástica de solo, exerciam influência no crescimento linear das crianças ou adolescentes. Alguns estudos demonstraram um maior crescimento do tecido ósseo e muscular em crianças e adolescentes atletas.
ConclusõesApesar do pequeno número de estudos com metodologia adequada, em especial ensaios clínicos randomizados, as evidências parecem indicar que o exercício físico seja seguro, tanto para a gestante como para a criança, desde a vida fetal até adolescência. O exercício físico não parece comprometer o crescimento linear da criança e contribui para moldar de forma ideal os tecidos ósseo e muscular e assegurar possíveis efeitos benéficos ao longo da vida.
Growth, considered as the increase in body size, measured as weight and height gain, is one of the main health indicators in childhood and adolescence.1 The growing phase is when human beings experience the greatest bio-psycho-social vulnerability. The pediatrician has one of the main tasks in medicine: to ensure that the child reaches their full potential for genetically determined growth.2 Several conditions directly or indirectly influence the child's growth, such as genetic, environmental, nutritional, metabolic, hormonal, and psychoactive factors, morbid conditions, and physical activity level. However, the latter still generates controversies regarding its effect on the growth of children and adolescents.3–6
Physical activity is defined as any activity of the body with the involvement of skeletal muscle that results in energy expenditure.7 During physical activity, increased heart rate and sweating are usually observed. Physical exercise is considered as a type of structured, organized, and previously planned physical activity, with repetitive practice and aiming at improving or maintaining physical conditioning.7
Physical activity brings several advantages to the human body, both regarding disease prevention and the treatment and rehabilitation of these conditions.8 When practiced during childhood, it also has another great benefit, as it tends to be maintained throughout life.9 The main doubts about possible harmful effects of physical exercise on weight–height growth, are concentrated on those practiced with vigorous intensity, as well as high-impact or resistance exercises.
The aim of this review is to describe current scientific knowledge on the benefits and harmful effects of physical activity on the weight–height growth of children and adolescents since intrauterine life.
MethodsSource of dataFor this review, a search was carried out in the PubMed/Medline, Embase, Scielo, and Cochrane databases, of studies published between January 1990 and October 2018. The combination of Medical Subject Headings (MeSH) and Portuguese descriptors (Descriptors of Health Sciences – DECS) was used to generate the list of terms for the search. The bibliographic search strategy was based on the combination of the independent variable (physical activity/physical exercise), dependent variable (weight–height growth) and the population of interest (fetuses, newborns, infants, preschoolers, schoolchildren, and adolescents). The following keywords were used: “physical activity” OR “physical exercise” OR “resistance training” OR “strength training” OR “sports” OR “athlete” AND “growth” OR “physical growth” OR “linear growth” OR “statural growth” OR “height” OR “body composition” AND “fetus” OR “newborn” OR “infant” OR “premature” OR “children” OR “school children” OR “preschool children” OR “teenage” OR “adolescent”.
Studies that presented an intervention or observation with some type of physical activity on the weight–height growth, involving the fetus, children or adolescents were included. Studies with different designs (cross-sectional, case–control, cohort, clinical trials, and review studies) were included in the review. The exclusion criteria were: studies in which the intervention with physical activity was associated with another intervention (diet, medication or other types) or with a population of children or adolescents with some type of disease. The methodological quality of the selected studies was independently assessed by the two authors using the CONSORT, STROBE, and PRISMA guidelines for clinical trials, observational studies, and systematic reviews, respectively.
Synthesis of dataA total of 1629 studies retrieved after the search carried out using the search terms were screened by reading the summary. After excluding the duplicate studies and applying the inclusion criteria, a total of 85 studies were selected, which were read in full and analyzed. Of these, 49 were excluded because physical activity was associated with another intervention or the population had some disease; thus, 36 studies were analyzed in this review, of which 20 were review articles.
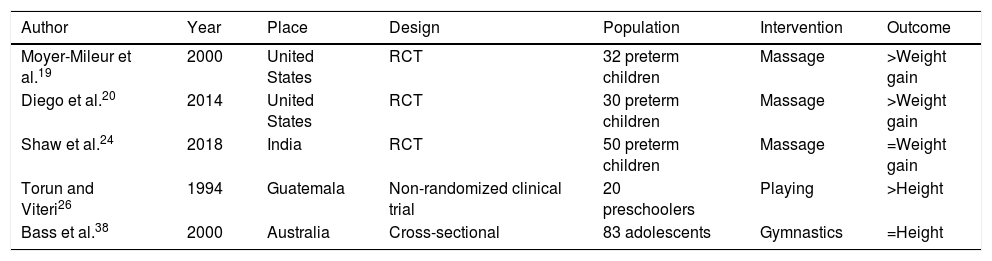
Table 1 shows the main studies with physical activity interventions and inclusion in the weight–height growth outcomes. It was observed that, in addition to the small number of participants, there were bias risks in the randomized clinical trials, both due to the uncertainty of the randomization process and the lack of blinding. Another clinical trial was nonrandomized and the cross-sectional study, by concomitantly analyzing exposure and response, is not appropriate for the research question proposed here.
Some characteristics of the studies involving physical activity and growth of children and adolescents.
| Author | Year | Place | Design | Population | Intervention | Outcome |
|---|---|---|---|---|---|---|
| Moyer-Mileur et al.19 | 2000 | United States | RCT | 32 preterm children | Massage | >Weight gain |
| Diego et al.20 | 2014 | United States | RCT | 30 preterm children | Massage | >Weight gain |
| Shaw et al.24 | 2018 | India | RCT | 50 preterm children | Massage | =Weight gain |
| Torun and Viteri26 | 1994 | Guatemala | Non-randomized clinical trial | 20 preschoolers | Playing | >Height |
| Bass et al.38 | 2000 | Australia | Cross-sectional | 83 adolescents | Gymnastics | =Height |
RCT, randomized clinical trial.
Differently from what was thought until recently, science now indicates that physical exercise during pregnancy is safe and brings benefits to both the pregnant woman and the child.10 For the pregnant woman, it reduces edema, back pain, constipation, anxiety, insomnia, and the risk of depression.2 Moreover, it improves the mood, disposition, and favors an eutocic delivery.11 The current recommendation is that of exercises of mild to moderate intensity for previously sedentary pregnant women, and of moderate to vigorous intensity for previously physically active pregnant women.9,10 Ideally, low impact exercises, such as water exercises and aerobics, should be performed at least three times a week.9,10 Several studies have indicated that this type of physical activity performed by the pregnant woman is not associated with a higher risk of growth deficit for the newborn.
A systematic review with meta-analysis of 30 clinical trials found that the weight of newborns of pregnant women that performed physical exercises of mild or moderate intensity were not different from those of physically inactive women; however, for women who performed vigorous physical exercises in the last trimester of pregnancy, the weight of the newborn decreased by 200–400g.12 The authors state that the data collected did not allow them to conclude whether this change had clinical repercussions, reflecting the low weight at birth or fetal macrosomia. However, more recently, another systematic review with meta-analysis assessed 28 randomized clinical trials and verified that the practice of supervised physical exercises during pregnancy protected against the birth of neonates that were large for gestational age (OR 0.69; 95% CI: 0.55–0.86), whereas it did not increase the risk of low birth weight.13 Nascimento et al., also in a systematic review, concluded that physical exercise by the pregnant woman, regardless of the type and intensity, had no effect on the weight of the newborn and did not increase the risk of preterm birth.14
In another systematic review, Aquilar Cordero et al. also failed to observe any changes in fetal growth in pregnant women who performed physical exercises, especially in those who practiced water exercises.15 A narrative review by Barakat et al. emphasized the heterogeneity of the studies with different physical activity interventions during pregnancy, but concluded for the safety of this practice, with no interference on fetal growth.16 Another more recent narrative review also concluded that the practice of physical exercise during pregnancy provided adequate fetal growth.17
Hopkins et al. observed that physical activity practice during the second half of the pregnancy increased levels of leptin and free fatty acids but did not interfere with the growth factor (insulin-like) and did not have any significant effects on fetal growth.18
This evidence appears to indicate that exercising during pregnancy does not alter fetal growth and contributes to the newborn's adequate birth weight.
Passive physical exercise for preterm infantsSome studies have indicated that passive or assisted physical exercise, i.e., the one produced by an external force, such as another person flexing or extending the limbs of the preterm child, brings benefits to the child's growth.
One of the first studies that indicated the possible benefits of passive exercises for the growth of preterm infants was a randomized clinical trial carried out in 2000. Moyer-Mileur et al. studied 32 preterm children and found that passive physical exercise, comprising passive resistance movements in the limbs, for five to ten minutes a day, resulted in greater weight gain and increased arm length, bone mass, bone mineral content, and fat-free mass in preterm infants.19
More recently, Diego et al. found that both massage and passive physical exercise (flexion and extension of the limbs), for ten minutes, three times a day, increased weight gain of preterm infants.20 Litmanovitz et al. studied 34 very-low-birth-weight infants whose intervention consisted in the passive flexion and extension of the limbs starting on the eighth day to the fourth week of life and observed that passive exercise increased bone strength.21
A recent systematic Cochrane review22 assessed 11 trials with 324 preterm infants with gestational age between 26 and 34 weeks, submitted to physical activity interventions ranging from three to eight weeks of duration. The meta-analysis with four trials found a positive effect of physical activity on weight gain and linear growth during the study period. Although the authors observed variations in the quality of the studies, they concluded there was some evidence suggesting that these programs promote weight gain and linear growth, as well as bone mineralization in these preterm infants. These effects on growth appear to occur through stimuli that promote the growth of long bones, and include increased bone mass and mineral deposition.23,24
Although these initial studies suggest that passive physical exercise contributes to preterm infants’ growth, investigations are still scarce and their methodologies are heterogeneous, which indicates the need for further studies, aiming to prove these findings.
Preschoolers’ physical activity and growthCertain stimuli aiming at increasing physical activity levels in preschool children have shown positive results on growth. In Germany, a randomized clinical trial showed the effects on growth of an intervention based on parental counseling carried out during regular childcare visits in the second week of life and in the second, fourth, and 11th months of age. During these visits, the parents were instructed to stimulate the motor development and physical activity of their children as much as possible.25 Of the 143 assessed children, differences were observed in relation to adipose tissue growth, as measured by skinfolds, which was lower in the intervention group. Girls also had lower weight and a smaller abdominal circumference.
Torun and Viteri26 observed that the linear growth of preschool children with nutritional recovery syndrome under the same diet was more intense in those who were stimulated to practice physical activity (games and activities that involved climbing stairs, ramps, running, pedaling, and jumping), than those not stimulated (control); in six weeks, both groups gained about 1.98kg; however, the physically active group grew more in height: 22±8 vs. 14±6mm, p<0.05.
Krneta et al.,27 in a controlled manner, observed the effects of an intervention program with kinesiological activities, applied intensively and for 60min daily, twice a week for nine months, on the growth and development of preschool children. They observed significant differences in the development of motor skills, muscle strength, flexibility, and coordination. According to the authors, these findings observed in the first year of life can shape the morphological growth of children, leading to greater growth of osteoarticular and muscle tissue. In turn, a clinical trial of 72 infants found that calcium intake influenced bone mineral content more than a motor exercise program focused on loading activities over the skeletal system, for 15–20min a day, five days a week for 18 months. Bone mineral content was associated with weight and height.28 Physical activity is important for the growth of bone, muscle, and adipose tissue.29,30 There appears to be a consensus that physical exercise can contribute to the child's future health, especially regarding body composition, and for this purpose, physical activity should be incorporated since the first years of life.29 Moreover, the literature has indicated that both the patterns of physical activity and body composition in childhood tend to persist into adult life.30
The studies on the effects of physical exercise on the growth of preschool children are scarce, and do not allow further conclusions yet. However, studies indicate that physical activity in early life appear to shape some tissues such as muscle, bone, and adipose tissue, exerting an influence throughout life.
SchoolchildrenThere is a well-established belief in our society that children should not attend gyms, because physical strength exercises can compromise linear growth. A systematic review with a meta-analysis31 assessed the effect of strength training or resistance exercises on the longitudinal growth in children aged 7–12 years. Of the 16 studies with 1008 analyzed participants that had measured longitudinal growth, no difference was observed in the linear growth of the children who underwent strength training and those who did not (p=0.46). The authors’ conclusion was that strength training does not negatively influence children's linear growth. Another cohort study found that vigorous physical activity limited adipose tissue growth but not linear growth in schoolchildren.32
The practice of competitive exercises also appears to be healthy. Damsgaard et al.33 found that prepubertal adolescents (184 children aged 9–13 years) did not have their growth modified by the practice of competitive sports. They also observed that constitutional factors were decisive in the child's choice of sports practice (tennis, swimming, handball, and gymnastics). The determinants of height were the predicted final height assessed between 2 and 4 years of age and the pubertal stage, whereas the type of sports practice had no influence on height.
It is known that physical exercise during childhood favors the increase in peak bone mass, which contributes to reduce the risk of osteoporosis and fractures throughout life. A systematic review of 19 cohort studies confirmed the importance of physical activity for bone mass growth, especially during the phases of greater growth, such as in the first months of life and puberty.34 Fuchs et al.35 studied the effects of a type of vigorous physical exercise, i.e., jumping, on bone mass. Of 89 randomized students, aged from 5.9 to 9.8 years, one group (control) performed only relaxation exercises, without impact, and the other (intervention), performed vigorous exercises, 100 jumps off a 61-cm platform, during seven months, three times a week. No growth differences were observed between the two groups (weight, height and adiposity); however, the bone mass in the group of jumpers increased more than that of the control group, 4.5% vs. 3.1%, respectively. The authors concluded that this program of physical exercise is safe, and that the jumping activity contributes to bone mass increase in schoolchildren.
The growth in muscle mass is also positively influenced by the practice of physical activity by schoolchildren and is associated with the growth of bone mass.36 A study with 98 prepubertal children, divided into those who practiced basketball and those that did not, indicated that the players had a higher bone and muscle mass growth when compared to those who did not play basketball and did not practice any other type of sports.37
Despite the scarce number of studies in schoolchildren addressing the effect of physical exercise on growth, the evidence tends to indicate benefits to bone and muscle mass growth and no height growth impairment caused by resistance or strength exercises.
Athlete adolescentsThe very popular beliefs that certain sports can modify the individual's final height, such as for instance, basketball practice increases height and gymnastics decreases, has no scientific basis. The choice of these sports is based on the individual's biotype and thus, tall people are more likely to succeed playing basketball, while those with shorter stature are more likely to practice and succeed in gymnastics. Bass et al., in a study with 125 gymnasts and 154 controls, observed that the practice of this sport was more sought after by athletes who had shorter leg length and its practice did not influence final height after puberty.38 Another study39 followed-up prepubertal and pubertal adolescents, male athletes who practiced high-impact gymnastics and non-athletes who did not exercise regularly, for 18 months. The height of gymnasts at baseline was shorter than that of non-athletes, although they were at the same stage of pubertal development (Tanner). No differences were observed regarding growth velocity and insulin growth factor-1 (IGF-1) during the 18-month follow-up. The authors’ conclusion was that the short stature observed in the gymnasts was due to a selection bias and not due to the effect of gymnastics itself.
The practice of vigorous physical exercises by adolescents does not appear to impair growth, as long as there is no negative energy balance, that is, as long as the diet is not adequate. In this situation, delayed pubertal development may occur due to hypothalamic–pituitary axis alteration.40
The effects of physical exercise during the pubertal spurt seem to bring benefits for the rest of the life. Nilsson et al.41 observed in 597 men studied that those who practiced more competitive exercises in adolescence had a larger bone cortical area in the tibia (6.3%, p<0.001) and a periosteal circumference (1.6%, p=0.011) in the diaphysis. That study appears to demonstrate that the practice of physical exercises during the individual's growth stage increases the cortical bone through periosteal expansion by providing a more durable bone throughout life. However, there is still controversy whether high impact exercises cause negative alterations in bone growth.42
As at the school age, there is no scientific basis for the idea that resistance training leads to changes in the growth plates in the pubertal stage. In this phase, immediately after the performance of resistance exercises, there is an increase in the circulating levels of testosterone and growth hormone.43
As for muscle mass, there appears to be no doubt regarding the benefits of physical exercise on its increase, especially in adolescence. The increase in muscle mass, which is more than 25% of the newborn's weight and is approximately 40% in adult life, reaches its peak velocity in the pubertal phase and benefits from physical activity. Research has shown that physical exercises in adolescence contribute to more muscle tissue in young adults.44
In adolescence, the practice of different sports does not appear to hinder or favor linear growth. In this age group, studies tend to indicate a special growth of bone and muscle tissues.
ConclusionsDespite the importance of the subject, the authors retrieved few studies with adequate methodology, especially randomized clinical trials, exploring the effects of physical exercises on the growth of children and adolescents. However, the evidence collected in this review appears to indicate that physical exercise during pregnancy is safe and does not alter fetal growth.
Passive physical exercise appears to contribute to the growth of preterm infants. The practice of physical exercises by children and adolescents is safe and appears to determine the growth of some tissues such as muscle, bone, and adipose tissue, exercising its influence throughout life.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Alves JG, Alves GV. Effects of physical activity on children's growth. J Pediatr (Rio J). 2019;95:S72–S78.




