


To analyze the effect of height catch-up at school age on the bone mass of adolescents of a Brazilian birth cohort.
MethodsA cohort study using data obtained from the three moments (birth, 7/9 years and 18/19 years of age) of the Cohorts-RPS study. Height catch-up was defined based on the difference between the schoolchild's z-score and birth z-score. The adolescents’ bone mineral mass was analyzed using the z-score index for the lumbar spine measured by dual emission X-ray absorptiometry. A theoretical model was developed for the proposed analysis using directed acyclic graphs paired through the nearest-neighbor matching propensity score using the STATA software, version 14.0. The level of significance was set at 5%.
ResultsOf the 297 studied children, 24.5% achieved height catch-up. The bone mass below the expected for age was observed in 5.39% of the subjects. The mean lumbar spine z-score was −0.34 (±1.01). After the adjustment, no effect was observed between height catch-up at school age and bone mass in adolescents (Coeff=0.598; 95% CI −0.117 to 1.313; p=0.101).
ConclusionEven using the directed acyclic graphs and the causal inference method by adjusting the propensity score, the height catch-up did not seem to affect bone mass in adolescents, a result perhaps related to the sample size.
Analisar o efeito do catch-up de estatura na idade escolar na massa óssea em adolescentes em uma coorte brasileira de nascimento.
MétodosEstudo de coorte, utilizando dados dos três momentos (nascimento, aos 7/9 anos e 18/19 anos) da pesquisa Coortes-RPS. Catch-up de estatura foi definida a partir da diferença entre o Z-score do escolar e Z-score do nascimento. Para a análise da massa óssea em adolescentes foi utilizado o índice Z-score da coluna lombar medido pela densitometria por dupla emissão de raio X. Para análise proposta, foi construído modelo teórico usando os gráficos acíclicos direcionados e pareado por escore de propensão do tipo vizinho mais próximo utilizando o software STATA versão 14.0. O nível de significância adotado foi de 5%.
ResultadosDas 297 crianças, 24,58% realizaram o catch-up estatural. Massa óssea abaixo do esperado para a idade foi de 5,39%. O Z-score médio da coluna lombar foi -0,34 (± 1,01). Após ajuste, não foi observado efeito entre catch-up de estatura na idade escolar e massa óssea no adolescente (Coef=0,598; IC 95% -0,117 – 1,313; p=0,101).
ConclusãoMesmo com os gráficos acíclicos direcionados e o método de inferência causal por ajuste do escore de propensão, o catch-up de estatura parece não afetar a massa óssea em adolescentes, resultado talvez relacionado ao tamanho da amostra.
The process of bone mineralization begins in intrauterine life and takes place from infancy to early adulthood. However, it is during childhood and adolescence that most bone tissue growth and development occurs, and these periods are essential for bone mass acquisition.1,2
The increase in bone mass accumulation is directly related to the lower risk of fractures and osteoporosis in the future and is sensitive to the influence of multiple modifiable and non-modifiable factors.3 Determinants that occur during the pregnancy and early childhood periods can affect bone mineral mass values in adolescence, and it is possible that the height catch-up in childhood may also have effects on bone mass.
Evidence from animal studies suggests that height catch-up occurs in large part due to delayed growth plate senescence.4,5 Thus, after a period of growth inhibition, these plaques maintain a greater chondrocyte proliferation capacity, are less senescent, and therefore show a higher growth rate than the expected for age, resulting in height catch-up.6
Despite the more recent hypothesis that the increase in chondrocyte proliferation with consequent growth (mainly of the long bones) would result in catch-up, the possible effects of this process on bone mass are still inconclusive in the long term, indicating that growth in height during childhood can be either associated to bone mineral mass in adulthood7 or it may indicate that catch-up does not influence bone mineral mass.8
Therefore, this study aimed to analyze the effect of height catch-up at school age on bone mass in adolescents from a Brazilian birth cohort performed in São Luís, state of Maranhão (MA), Brazil, hypothesizing that it may have beneficial effects on the bone mass in adolescents.
MethodsThis is a cohort study using information from the research “Determinants throughout the life cycle of obesity, precursors of chronic diseases, human capital and mental health – RPS Cohorts” (Determinantes ao longo do ciclo vital da obesidade, precursores de doenças crônicas, capital humano e saúde mental – Coortes RPS), developed by Universidade Federal do Maranhão, Faculdade de Medicina de Ribeirão Preto and Universidade Federal de Pelotas, and funded by the Department of Science and Technology. For this study we used data from São Luís, MA.
Population and data collectionThis cohort currently encompasses 3 moments:
Moment 1 – BirthThe perinatal study of the São Luís (SL) cohort was started in ten public and private hospitals in the city, at birth, from March 1997 to February 1998. The population-based sample included 96.3% of the births from the period, excluding non-hospital births and births in hospitals with fewer than 100 deliveries per year. Systematic sampling with proportional stratification was used, according to the number of births in each maternity unit, of one in seven deliveries. The total of 2541 hospital births included women living in São Luís, live births, stillbirths and single and multiple births. After excluding multiple births and stillbirths, the final sample consisted of 2443 births, and losses due to refusal or impossibility to locate the mother occurred in 5.8% of the cases.9
Moment 2 – School ageThe São Luís cohort was followed in 2005/2006, at 7/9 years of age, through a complex sampling design, using the birth weight variable to define the sample necessary for the school age evaluation.10
For the height catch-up investigation, the z-score of the birth length for gestational age was calculated using an application from The International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH21st),11 and the height z-score at school age was calculated using the growth curves of the World Health Organization.12
The height catch-up at school age variable was defined based on the difference between the schoolchild's z-score and birth z-score using the definition proposed by Ong et al.,13 which consists of defining a z-score change ≥0.67 as catch-up. The children whose z-score changes on the studied anthropometric indexes were between −0.669 and 0.669 were considered as having normal growth. When defining catch-up as the difference between the z-score of the schoolchild's height and z-score of the birth length, of the 805 followed children, those whose birth length was ignored (totalizing 691 children) were excluded.
Moment 3 – AdolescenceIn 2015, the participants were invited to return for further evaluation at 18/19 years old. Two strategies were developed to locate them: search in the military enlistment records (for boys only) and schools (for both boys and girls). For the search in schools, the participants were located from the 2014 school census by comparing the mother's name, the participant's date of birth and name (for those who came in 2005/2006) and mother's name and the participant's date of birth (for those who did not come for the follow-up).
From January to November 2016, those adolescents – totaling 659 individuals – were scheduled to undergo evaluation. At that stage, the following data were investigated, among others: nutritional status, body composition, origin of complex chronic diseases, mental diseases, socioeconomic and demographic status, income, living habits and cognitive skills, using equipment such as BOD POD® (Life Measurement, Inc, CA, USA) and dual X-ray absorptiometry (DXA), laboratory tests and structured and validated questionnaires.
For the bone mass analysis in this study the z-score of lumbar spine (L1-L4) was obtained through the Lunar GE DXA (GE Healthcare, CA, USA) device, which was calibrated daily. In this evaluation, the participant, wearing standard clothes, laid on the bed beside the device and was submitted to a whole body, spine and femur scanning. The adolescents did not wear any metal objects or had pins/plates in the bones. This device measures the difference between the patient's bone mineral density and the mean bone mineral density of the population of same age, gender and ethnicity. Adolescents with z-scores ≤−2.0 SD (standard deviation) were considered “below the expected range for age”.14 However, the continuous z-score was used for the statistical analysis.
In this study, it was necessary to evaluate the individuals who participated in the three moments, as birth length, height at 7/9 years old and bone mass during adolescence were all necessary, thus totaling 297 adolescents.
Theoretical model, variables and statistical analysisInitially, descriptive analyses were performed to obtain the absolute and relative frequencies for categorical variables.
To analyze the effect of height catch-up in students and bone mass in adolescents, a theoretical model was developed using the Directed Acyclic Graphs (DAGs) generated with the aid of the DAGitty software, version 3.0.15 The DAGs are causal diagrams that allow the researcher to visualize the study question, establish causal assumptions between variables, and define a minimum set of variables to estimate the effect of exposure on the outcome, controlling the confounding effects and avoiding unnecessary adjustments.16
In this study, based on the literature, the model proposes to graphically represent the influence of height catch-up at school age on bone mass during adolescence, according to Fig. 1.

The set for the minimum required adjustment indicated by the DAG in order to control confounding effects consisted of the following variables:
- •
Moment 1 – Birth
- •
Smoking in pregnancy: yes or no;
- •
Child's gender: female or male;
- •
Gestational age imputed in months;
- •
Intrauterine growth restriction defined by Kramer et al.17 based on the birth weight ratio calculated by the computer application The International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH21st),11 equivalent to the ratio between the newborn's weight and the mean weight for GA. According to Kramer et al.,17 a birth weight ratio ≥0.85 was defined as without Intrauterine Growth Restriction (IUGR), and birth weight ratio <0.85 was defined as IUGR.
- •
School age
- •
Family income in minimum wages: less than 1 minimum wage, from 1 to less than 4, and 4 or more minimum wages;
- •
Maternal and paternal heights: continuous variables (meters);
- •
Exclusive breastfeeding until the sixth month: yes or no, obtained from the breastfeeding time and age at the introduction of complementary feeding.
The indication of these variables for minimum adjustment occurred based on the back-door criterion, which considers the need for adjustment for a variable that is common cause to other two variables, in a certain causal pathway, and does not indicate adjustment for a collider variable, one which is caused by other two variables, in the same causal path. Through the back-door principle, incorrect and unnecessary adjustments that could lead to estimation errors are prevented in data analyses.15,18,19
We chose the causal inference method to perform this analysis to search for a closer approximation of causality, as well as to eliminate the bias associated with the distribution differences of the variables in the exposed and non-exposed groups. This method also allows the comparison of different situations in the same individual, with the latter being evaluated both as treated (exposed) and nontreated (not exposed), since the observed (factual) data and estimates contribute to the estimation of the non-observed ones (counterfactual).20
The nearest-neighbor matching propensity score technique was used, in which the treated individual is paired with the control that has the nearest propensity score through the nnmatch routine of the teffects command. The propensity score matching was used to remove selection bias associated with differences in the covariate distributions in the catch-up group and those without catch-up. Each child was assigned a weight or a propensity of being in the group. According to Rosenbaum and Rubin,21 the propensity score is the conditional probability of receiving treatment given the preestablished characteristics, since its efficiency in removing the bias originated by the observed variables has been demonstrated in both large and small samples.22
After obtaining the causal effect estimation, the balancing was verified through the tebalance summ routine, to verify whether the balance between the groups (treated and nontreated) was achieved, that is, if the predictor variables showed standardized differences equal or close to zero and rates of variance equal to or close to one. The level of significance was set at 5%. All analyses were performed using the STATA software (Stata Statistical Software: Release 14. College Station, TX, USA).
The project meets the criteria of Resolution 466/2012 of the National Health Council and its complementary regulations. The interviewees were invited to participate in the study. When they agreed to participate, they signed the Free and Informed Consent Form. The interviewees were allowed to leave the study at any stage of the research, without any harm to them and their families. The project was approved by the Research Ethics Committee of the Hospital Universitário – UFMA, under Opinion n. 1,302,489.
ResultsOf the participants who returned for the follow-up at 18/19 years old 73 (24.58%) went through height catch-up in childhood. Sixteen adolescents (5.39%) had bone mass below the expected for age. The mean z-score of the lumbar spine was −0.34 (±1.01).
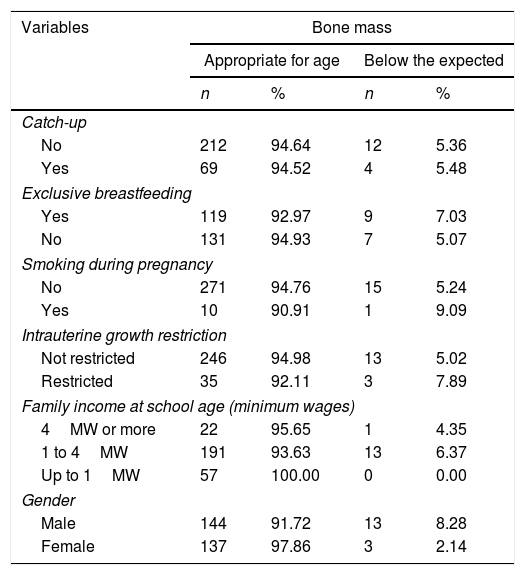
The maternal gestational and socioeconomic characteristics and the characteristics of the children from the cohort according to bone mass are described in Table 1.
Maternal and participants’ characteristics and bone mass of the RPS Cohort, São Luís, MA, 2017.
| Variables | Bone mass | |||
|---|---|---|---|---|
| Appropriate for age | Below the expected | |||
| n | % | n | % | |
| Catch-up | ||||
| No | 212 | 94.64 | 12 | 5.36 |
| Yes | 69 | 94.52 | 4 | 5.48 |
| Exclusive breastfeeding | ||||
| Yes | 119 | 92.97 | 9 | 7.03 |
| No | 131 | 94.93 | 7 | 5.07 |
| Smoking during pregnancy | ||||
| No | 271 | 94.76 | 15 | 5.24 |
| Yes | 10 | 90.91 | 1 | 9.09 |
| Intrauterine growth restriction | ||||
| Not restricted | 246 | 94.98 | 13 | 5.02 |
| Restricted | 35 | 92.11 | 3 | 7.89 |
| Family income at school age (minimum wages) | ||||
| 4MW or more | 22 | 95.65 | 1 | 4.35 |
| 1 to 4MW | 191 | 93.63 | 13 | 6.37 |
| Up to 1MW | 57 | 100.00 | 0 | 0.00 |
| Gender | ||||
| Male | 144 | 91.72 | 13 | 8.28 |
| Female | 137 | 97.86 | 3 | 2.14 |
MW, minimum wage.
There was an association between height catch-up at school age and bone mass in adolescence in the non-adjusted analysis (Coeff=0.35, 95% CI: 0.085–0.617, p=0.010) (Table 2).
Non-adjusted and adjusted effect of height catch-up effect at school-age on adolescent bone mass, São Luis, MA, 2017.
| Non-adjusted | Adjusted | |||||
|---|---|---|---|---|---|---|
| Coeff. | CI (95%) | p-Value | Coeff. | CI (95%) | p-Value | |
| Catch-up | 0.351 | 0.085–0.617 | 0.010 | 0.598 | −0.117 to 1.313 | 0.101 |
Coeff., coefficient; CI, confidence interval.
Note: propensity score matching technique.
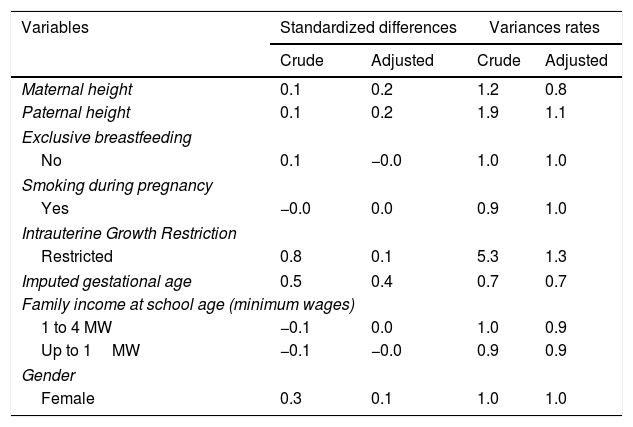
After propensity score matching for the variables proposed by the theoretical DAG models no effect was observed between height catch-up in age and bone mass (Coeff=0.598, 95% CI: −0.116 to 1.313, p=0.101) (Table 2). This suggests that after the matching and removing the differences regarding paternal and maternal height, imputed gestational age, intrauterine growth restriction, child's gender, smoking during pregnancy, and family income at school age it seems there is no effect of height catch-up in childhood on lumbar spine bone mass in young adulthood. The balancing between the groups was evaluated (Table 3).
Standardized differences and crude and adjusted variance rates in group balancing, São Luís, MA, 2017.
| Variables | Standardized differences | Variances rates | ||
|---|---|---|---|---|
| Crude | Adjusted | Crude | Adjusted | |
| Maternal height | 0.1 | 0.2 | 1.2 | 0.8 |
| Paternal height | 0.1 | 0.2 | 1.9 | 1.1 |
| Exclusive breastfeeding | ||||
| No | 0.1 | −0.0 | 1.0 | 1.0 |
| Smoking during pregnancy | ||||
| Yes | −0.0 | 0.0 | 0.9 | 1.0 |
| Intrauterine Growth Restriction | ||||
| Restricted | 0.8 | 0.1 | 5.3 | 1.3 |
| Imputed gestational age | 0.5 | 0.4 | 0.7 | 0.7 |
| Family income at school age (minimum wages) | ||||
| 1 to 4 MW | −0.1 | 0.0 | 1.0 | 0.9 |
| Up to 1MW | −0.1 | −0.0 | 0.9 | 0.9 |
| Gender | ||||
| Female | 0.3 | 0.1 | 1.0 | 1.0 |
MW, minimum wages.
In the present study, data analysis showed that there is probably no height catch-up effect on adolescents’ bone mass (p=0.101). It is believed that this result at the significance threshold is due to the sample size, especially in the treated group (73 participants). Another possible explanation would be the fact that a young sample was analyzed, thus making it difficult to perceive possible effects. However, although young, 16 (5.39%) participants were considered as individuals with bone mass below the expected for age, reaching a z-score of −2.9 in the lumbar spine.
Despite the loss at follow-up, the use of propensity-score matching was considered a strength of this study by promoting the reduction of biases associated with differences in covariate distributions in the treated and nontreated groups using the causal inference technique.
It is also worth noting that bone mass was evaluated by DXA, which is considered the gold standard. Additionally, bone health during the first years of life as well as in puberty is an important determinant of bone mass at more advanced ages, and this early assessment was possible in this study.
Studies associating adolescence and bone health have increasingly gained prominence in international research. The childhood and adolescence periods are characterized by a very important bone formation rate, with a predominance of formation over resorption; in adulthood, these processes stabilize; from the age of 45 to 50, there is a predominance of bone resorption, especially in females.23
Although studies indicate an association between catch-up in childhood and adverse outcomes in adulthood,24 the present study in a sample of adolescents obtained results that are in agreement with those obtained by Leunissen et al.8 in a cohort of 312 young adults, who have also not found an association between height catch-up and bone mass in adulthood. Using linear regression, the authors demonstrated that individuals born small for gestational age (SGA), with subsequent catch-up resulting in normal height in adulthood, did not show any differences in bone mass parameters when compared to the individuals born appropriate for gestational age (AGA) who reached normal height (controls).
Ay et al.25 also found no association between height catch-up and bone mass of the whole body (OR=0.7, 95% CI: 0.25–1.76) and the lumbar spine (OR=0.7, 95% CI: 0.26–1.81) in a cohort study carried out in the Netherlands, which aimed to assess the association between characteristics of the family, birth, postnatal period and growth patterns in fetal life and childhood with bone mass measured through DXA in 252 children for 6 months.
However, Fewtrell et al.,7 when studying growth, bone mineral content and bone mineral density, showed an association of the significant height growth between the birth and follow-up of preterm newborns with greater bone mass. They also showed that length is a strong predictor of bone mass, suggesting that optimization of early linear growth may be beneficial for bone health. With similar results, Mikkola et al.,26 when assessing the bone area, bone mineral content and bone mineral density in 178 adult women in a Helsinki cohort, showed through linear regression models that growth in height before 7 years of age was associated with bone mineral content in the femoral neck (p<0.01) as well as bone mineral content in the spinal column (p<0.05), concluding that height optimization in girls is important to achieve a bigger skeleton and, consequently, greater bone mass.
Results such as those reinforce the hypothesis raised in this study that the improvement of linear growth in children may be important to maximize bone mass. Although we did not investigate hormonal measurements, it is possible that growth hormone (GH) and insulin-like growth factor type 1 (IGF-1) hormone, which are important for bone mass maintenance and determinants of longitudinal bone growth, skeletal maturation, and bone mass acquisition during childhood, adolescence and in adulthood,27–30 may also participate in this process through their action on chondrocyte proliferation and differentiation in the long bone growth plate,31 a process that would lead to catch-up.
Even though osteoporosis is a disease of adulthood, it should nevertheless be prevented and monitored through the promotion of bone health throughout childhood and adolescence. The pediatrician should advise on the importance of healthy living habits and physical activity, with the purpose of ensuring that the child and the adolescent develop adequate bone mass, preventing diseases.32 Although there was no significant effect of height catch-up in childhood on the lumbar spine bone mass in a sample of adolescents from the Northeast of the country, it is noteworthy that this is one of the first Brazilian studies to investigate this issue, thus suggesting that further studies must be carried out.
FundingThis work was supported by Fundação de Pesquisa do Estado do Maranhão (FAPEMA) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Rodrigues LS, Batista RF, Simões VM, Rodrigues MR, Barbieri MA, Bettiol H, et al. Does height catch-up in schoolchildren have an effect on bone mass in adolescents? Analysis in a Brazilian birth cohort. J Pediatr (Rio J). 2019;95:607–13.
Study carried out at the Department of Public Health, Universidade Federal do Maranhão, São Luís, MA, Brazil.




