


To assess the frequency of baked egg tolerance in IgE-mediated egg allergy patients through the oral food challenge and to assess the tolerance predictability of different skin prick tests, as well as specific serum IgE measurement to egg proteins.
MethodsIn this cross-sectional study, 42 patients with a diagnosis of egg allergy were submitted to different skin prick tests with egg (in natura, boiled, muffin, ovalbumin, and ovomucoid), and specific IgE to egg white, ovalbumin, and ovomucoid; as well as to the oral food challenge with food containing egg, extensively baked in a wheat matrix.
ResultsOf the total, 66.6% of patients tolerated the ingestion of egg-containing foods in the oral food challenge. A comparative analysis with positive and negative oral food challenge found no significant differences regarding age, gender, other food allergies, or even specific skin prick tests and IgE values between the groups.
ConclusionsThe study demonstrated an elevated frequency of baked egg food-tolerant individuals among egg allergy patients. None of the tested markers, skin prick tests, or specific IgE, were shown to be good predictors for identifying baked egg-tolerant patients. The oral food challenge with egg baked in a matrix is central to demonstrate tolerance and the early introduction of baked foods, improving patients’ and families’ quality of life and nutrient intake.
Avaliar a frequência de tolerância a alimentos assados com ovo em pacientes com alergia ao ovo mediada por IgE por meio do teste de provocação oral e verificar a capacidade de predição de tolerância ao ovo por meio de teste cutâneo de leitura imediata (Skin Prick Test ou SPT) e de dosagem sérica de IgE específica para componentes do ovo.
MétodosEstudo transversal, 42 pacientes com diagnóstico de alergia ao ovo foram submetidos a SPT com ovo (in natura, cozido, bolinho, ovoalbumina e ovomucoide), IgE específica para clara de ovo, ovoalbumina e ovomucoide e ao teste de provocação oral com alimento com ovo extensamente assado em matriz de trigo.
ResultadosDos pacientes, 66,6% toleraram a ingestão do alimento com ovo durante o teste de provocação oral. Não encontramos diferenças em relação a idade, gênero, outras alergias alimentares ou mesmo entre os valores dos SPT e IgE específicas na análise comparativa entre os grupos com teste de provocação oral positivo e teste de provocação oral negativo.
ConclusõesFoi demonstrada uma elevada frequência de indivíduos tolerantes a ingestão de alimentos assados com ovo entre os pacientes com alergia a ovo mediada por IgE. Nenhum dos marcadores testados, SPT ou IgE específica, demonstrou ser bom preditor para identificar os pacientes tolerantes. Consideramos que os testes de provocação oral com alimentos com ovo assado sejam fundamentais para a introdução desses assados, melhorar a qualidade de vida e a ingestão de nutrientes dos pacientes e famílias.
Cases of food allergy (FA) have increased significantly over the past decade, becoming a public health problem in several regions of the world, associated with a negative impact on the quality of life of individuals and of the whole family.1,2
In early childhood, the most common allergens are cow's milk and chicken egg, with an estimated prevalence ranging from 2% to 3% in different countries.3,4 Regarding egg-mediated IgE, a previous study in Brazil demonstrated that 1% of infants and preschoolers had this egg allergy pattern confirmed in the oral food challenge (OFC).5 In contrast, an Australian study reported a prevalence of IgE-mediated egg allergy in 8.9% of children in early childhood, a figure much higher than in Brazil, Europe, or the United States.6,7
The main allergenic proteins identified in the egg have different physicochemical characteristics and different allergenic potentials; therefore, the thermal heat processing and digestibility have a different impact on the allergenic capacity of these proteins.8
Different tests have been developed to detect egg protein-specific IgE; however, the ability of these tests to predict a patient’s risk of developing a reaction or the severity of this contact with the egg is still extremely low. Therefore, in the clinical practice of egg allergy management, total allergen elimination diet remains the recommendation of the main treatment guidelines.1,9,10
There is a possibility that these patients can ingest foods with processed egg protein (baked/cooked in a matrix such as wheat, corn, or tapioca starch). Considering that this type of food is widely used in many countries, this ingestion would result in greater freedom, more options, higher nutrient intake and quality of life for the patients and their families.2,11 Data on the frequency of patients with egg allergy who are tolerant to processed egg-containing products, the correlation of allergic testing with this tolerance profile, as well as the effects of baked food ingestion on the time and evolution of egg allergy are still scarce and require more studies.
Therefore, the aim of the present study was to assess the frequency of baked egg food tolerance and to investigate processed allergen tolerance markers using skin-prick tests (SPT) for immediate reading and egg-specific IgE components and the clinical reactivity observed for the performed OFC with extensively baked egg protein in children with IgE-mediated egg allergy.
MethodsThis was a cross-sectional study carried out at the Pediatric Allergy and Immunology Outpatient Clinic of Hospital de Clínicas of Universidade Federal de Uberlândia, from July 2014 to June 2017. The study included children between 0 and 12 years of age, registered at the clinic, diagnosed with IgE-mediated chicken egg food allergy and history of previous allergic reaction in the last six months, with recommendation of elimination diet by the team. The project was carried out in accordance with the Declaration of Helsinki, approved by the local Ethics Committee under protocol number 32030714.4.0000.5152, and the legal guardian and/or patient signed an informed consent for and/or assent form for the patient's participation in the study.
During the study period, 98 patients were evaluated at the outpatient clinic and had a diagnosis of chicken egg protein allergy. Of this total, ten patients were excluded because they did not have classic IgE-mediated symptoms and 12 were excluded because they did not consent to all study steps, resulting in a final sample of 76 patients. The initial clinical data were collected from medical records and subsequently submitted to an extensive food frequency questionnaire applied by the researchers at the time of the OFC. It was found that 34 participants sporadically or regularly consumed baked foods containing egg protein, without any symptoms. In total, 42 participants undergoing total elimination diet were admitted to the study and underwent the OFC, SPT with immediate reading, and egg component-specific IgE measurement.
Skin prick testsSPTs were performed by the same researcher on the same day as the OFC, using standardized commercial extracts of ovalbumin (OA) and ovomucoid (OM; IPI-ASAC―São Paulo, Brazil),as well as prick-to-prick testing with “in natura” egg white, boiled egg white (cooked for nine minutes after the boiling point was reached), and baked egg in a muffin according to the rules established by the Brazilian Society of Allergy and Immunology.12 The test was considered positive when the resulting papule diameter was ≥3.0mm (mm) in relation to the negative control; however, all absolute values were used for comparisons.
Specific IgE measurementThe egg protein-specific IgE class antibodies analyzed in the study were for egg white, ovalbumin, and ovomucoid (Immunocap – Phadia, MA, United States), which were collected approximately30 days before the OFC at the clinical analysis laboratory of Hospital de Clínicas; levels ≥ 0,35κu/L were considered positive. All absolute values were used for comparisons between the groups.
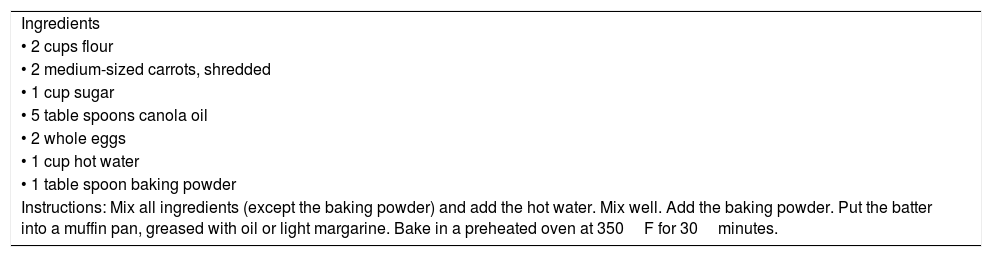
Oral food challengeThe OFC testing performed in the study was openly adapted from the AAAI/EAACI (American Academy of Allergy, Asthma & Immunology/European Academy of Allergy and Clinical Immunology) recommendations.9,10 The caregivers and the children were instructed about the OFC routine, the need to discontinue drugs that might interfere with the SPT and OFC (especially antihistamines and prolonged oral cortico therapy) and the risks of adverse reactions by a member of the multidisciplinary team of the Pediatric Allergy and Immunology outpatient clinic. For the oral food challenge test with the extensively baked egg protein, a recipe developed by the unit’s nutrition team was used in the form of a “muffin” (using a wheat matrix), with approximately 2.2g of egg protein and 12.5% total fat, baked at 350F for 30min (Table 1), with 1/4 of the unit (1 muffin) being offered every 20min (0, 20, 40, and 60min). After completing the OFC, the patient remained under observation at the clinic for at least 2h to evaluate objective symptoms. The participant was only released after this period if there were no objective symptoms related to food allergy. Subjective symptoms, according to the protocol used, did not prevent the test progression and did not interfere with its completion. The OFC was discontinued and considered positive if the child showed objective signs of allergic reaction, such as urticaria, angioedema, pruritus, wheezing, dyspnea, coughing, vomiting, diarrhea, hypotension, or fainting.9,10 The families of patients who underwent the testing without reactions at the OFC were instructed to maintain the daily consumption of at least a similar portion from different recipes to avoid food monotony.
Muffin recipe (yields 12 units).
| Ingredients |
| • 2 cups flour |
| • 2 medium-sized carrots, shredded |
| • 1 cup sugar |
| • 5 table spoons canola oil |
| • 2 whole eggs |
| • 1 cup hot water |
| • 1 table spoon baking powder |
| Instructions: Mix all ingredients (except the baking powder) and add the hot water. Mix well. Add the baking powder. Put the batter into a muffin pan, greased with oil or light margarine. Bake in a preheated oven at 350F for 30minutes. |
The Kolmogorov–Smirnov test was used to calculate normality, and the nominal variables were described as frequencies; the Mann–Whitney test was used to analyze the continuous variables, and the chi-squared test for categorical variables. All calculations were performed using the software GraphPad Prism 7.0 (GraphPad Prism version 7.00 for Windows, GraphPad Software, CA, United States).
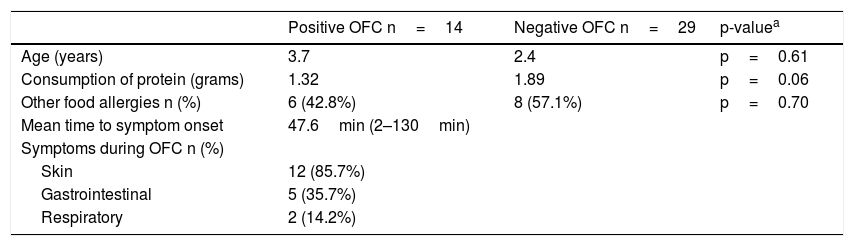
ResultsThe mean age of the group of patients submitted to OFC with the muffin containing baked egg was 3.98 years, ranging from 6 months to 11 years. At the end, 28 (66.66%) of the patients showed no reactions during the OFC and were considered tolerant, while 14 (33.34%) showed objective symptoms during the OFC with processed egg product, being considered positive and required that the test be discontinued and the use of medication. In this group with positive OFC, the median age was 3.78 years (2.46–6.31 years, 95%CI), the mean protein intake was 1.32g (0 to 2.2g), and the mean time between the beginning of ingestion of processed egg and symptom onset was n 47.6min (2 to 130min). No statistically significant differences were observed between patients with positive and negative OFC regarding age, gender, and other food allergies. Comparisons between the groups with positive and negative OFC with baked egg foods are shown in Table 2. Regarding the symptoms exhibited by patients with positive OFC, five patients showed involvement of two systems; however, none of them required adrenaline use. Symptom frequency, stratified by system, is also shown in Table 2.
Characteristics of patients with egg allergy submitted to the OFC, n=42.
| Positive OFC n=14 | Negative OFC n=29 | p-valuea | |
|---|---|---|---|
| Age (years) | 3.7 | 2.4 | p=0.61 |
| Consumption of protein (grams) | 1.32 | 1.89 | p=0.06 |
| Other food allergies n (%) | 6 (42.8%) | 8 (57.1%) | p=0.70 |
| Mean time to symptom onset | 47.6min (2–130min) | ||
| Symptoms during OFC n (%) | |||
| Skin | 12 (85.7%) | ||
| Gastrointestinal | 5 (35.7%) | ||
| Respiratory | 2 (14.2%) |
OFC, oral food challenge; Skin, angioedema, urticaria, rash, pruritus; Gastrointestinal, vomiting or diarrhea; Respiratory, coughing, sneezing or wheezing.
Serum IgE specific values for egg white, OA, and OM varied considerably in both positive and negative OFC groups; the same was observed for the SPT diameters, which showed wide variation in both groups. The medians of the specific IgEs showed no significant difference in the positive and negative OFC groups, respectively: 19.9Ku/L and 11.6Ku/L (p=0.48) for egg white, 12.6Ku/Land 1.6Ku/L (p=0.44) for ovomucoid, and 9.4Ku/L and 5.5Ku/L (p=0.90) for ovalbumin (Fig. 1). The medians of the papule diameters observed in the SPT also showed no significant differences between the groups with positive and negative OFC, respectively: 7.7mm and 6.5mm (p=0.59) for raw egg whites, 4.5mm and 4.00mm (p=0,51) for cooked egg whites, 2.5mm and 0.0mm (p=0.49) for the muffin, 7.5mm and 5.5mm (p=0.19) for OM, and 5.2mm and 5.0mm (p=0.70) for OA (Fig. 2).
 with foods containing processed egg: (A) egg white-specific IgE, (B) ovomucoid IgE, and (C) egg albumin IgE.")
 between groups with positive and negative OFC performed with egg processed products. (A) SPT with raw egg white, (B) SPT with cooked egg white, (C) SPT with muffin, (D) SPT with ovomucoid and (E) SPT with ovalbumin.")
Food allergy has an impact on the quality of life of both children and the entire family, interfering with activities of daily life, including school and social activities, due to the risk of potentially severe allergic reactions, such as anaphylaxis.1,13 FAs also lead to the search for alternative foods; particularly, the exclusion of milk and eggs is associated with inadequate micronutrient intake and higher household costs due to the need to purchase alternative and usually more expensive foods. In this context, the possibility of introducing baked foods containing eggs may result in benefits to the patient from the nutritional standpoint, as well as those aspects related to the perception of quality of life and lower financial cost to the families.
To date, few studies have evaluated patients allergic to eggs who are tolerant to baked foods through the OFC with foods containing processed eggs. Over the past decade, these studies have described that most patients undergoing open OFC showed egg tolerance from 63% to 73%, similar to that found in the present cohort who underwent the OFC.6,14–18 Considering the initial group of 76 patients with egg allergy and those who inadvertently ingested foods containing baked eggs without symptoms, this percentage of tolerant patients rises to 81.57%.
The wide variation of specific IgE values egg for different egg proteins in the positive and negative OFC groups demonstrated that no specific IgE was able to predict the reaction to foods containing processed eggs. Regardless of the studied IgE, the present study observed the existence of tolerant patients with very high values, as well as patients with low values and reactive during the OFC test with the baked foods. Statistically, a larger sample size could indicate some difference between the medians, but it would still not be possible to reach a specific value to guide the pediatrician’s or allergist’s decision regarding whether or not to introduce the baked foods. A previous study conducted an OFC test with muffins in 169 patients and found a statistically significant difference for egg-white IgE (1.3κu/L and 6.0κu/L, p<0.001) and OM (<0.35κu/L and 0.76κu/L, p=0.003).8 Another group described similar data, indicating a median IgE for egg white of 2.81κu/L and 5.85κu/L (p=0.001) in the groups with positive and negative processed egg OFC, respectively.17 These studies, despite their statistical differences, presented great variation of IgE values in the groups, similar to the present findings. Therefore, the few studies available in the literature showed data similar to those found in the present study, demonstrating the low predictive power of specific IgE for egg components and tolerance to egg-containing baked foods in patients with IgE-mediated egg allergy.8,17
Studies using SPT for different forms of egg protein presentation and OFC for baked foods are very scarce in the medical literature. As with the specific IgE, the SPT showed a large variation in values in both groups, without statistical difference. The SPT performed with the muffin prepared for the test itself showed a median of 0mm in the OFC-tolerant group; however, other patients in the OFC-reactive group also showed zero mm values and some in the tolerant group showed tests reaching up to 12mm, once again hindering tolerance prediction.
In the literature, a single study (n=143) that evaluated the SPT with the processed egg (muffin) showed results similar to the present findings, where the values for the SPT median values for egg white, with the muffin itself and OM showed 7.7mm, 6.0mm, and 7.5mm, respectively.15 Similarly to IgE, a single previous study using SPT found results that were similar to those of the present study, also demonstrating a low predictive power of SPT for egg components and tolerance to egg-containing baked foods in patients with IgE-mediated egg allergy.15
The present study has limitations, especially the small sample size after excluding those who regularly or sporadically ingested egg-containing foods from the initial sample, which does not invalidate the final results.
In conclusion, the present study demonstrated the high frequency of patients tolerant to foods with baked eggs among those with IgE-mediated egg allergy in Brazil and that SPT, specific IgE, and none of the markers tested were shown to be good predictors for identifying tolerant or intolerant patients. The authors that the performance of OFC with foods containing eggs baked in a matrix is crucial for the introduction of these foods, improving the quality of life and nutrient intake of patients and their families.
FundingHospital de Clínicas of Universidade Federal de Uberlândia and Postgraduate Program in Health Sciences of Universidade Federal de Uberlândia, only for the specific IgE tests and materials required for SPT and OFC.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Vilar LK, Rolins Neto PR, Abdo MA, Cheik MF, Afonso CP, Segundo GR. Baked egg tolerance: is it possible to predict? J Pediatr (Rio J). 2020;96:725–31.





