

To describe the challenges faced by families caring for children with autism spectrum disorder (ASD) in Brazil and the coping strategies employed.
SourcesSystematic review of articles published until September of 2013, without language restrictions, using quality appraisal (AMSTAR and CASP/Oxford instruments).
Summary of the findingsThe literature shows parental emotional overload as one of the main challenges faced by families, especially mothers. The main stressors were diagnostic postponement, difficulty dealing with the diagnosis and associated symptoms, and poor access to health services and social support. The predominant coping strategies found included information exchange between affected families and integrated healthcare network for patient and family support.
ConclusionASD exerts strong influence on family dynamics, resulting in caregiver overload, especially in mothers. The Brazilian Unified Health System needs to provide comprehensive, continuous, and coordinated care to strengthen the patient-family dyad and promote the full development and societal inclusion of children with ASD.
Descrever os desafios encontrados pelas famílias na convivência com crianças portadoras de transtorno do espectro autista (TEA) no Brasil e as estratégias de superação empregadas.
Fonte dos dadosRevisão sistemática da literatura com inclusão de artigos publicados até setembro de 2013, sem restrições de idioma. Os artigos incluídos foram submetidos à avaliação de qualidade metodológica através do AMSTAR e CASP/Oxford.
Síntese dos dadosInclui-se estudos provenientes de São Paulo e Rio Grande do Sul com alta e moderada qualidade metodológica. A literatura mostra sobrecarga emocional dos pais como um dos principais desafios encontrados pelas famílias, inclusive com grande tensão sobre as mães. Dentre os fatores relacionados ao estresse estão: postergação diagnóstica, dificuldade de lidar com o diagnóstico e com os sintomas associados, acesso precário ao serviço de saúde e suporte social. Dentre as estratégias de superação destacaram-se: troca de informações entre as famílias afetadas e assistência integralizada da rede de saúde no atendimento do paciente e suporte à família.
ConclusãoObservou-se que o TEA exerce forte influência na dinâmica familiar com sobrecarga dos cuidadores, geralmente da mãe. O Sistema Único de Saúde necessita prover cuidado integral, longitudinal e coordenado visando o fortalecimento do binômio paciente-família e o pleno desenvolvimento e inserção destas crianças na sociedade.
Autistic spectrum disorder (ASD) is a neuropsychiatric syndrome characterized by behavioral manifestations accompanied by deficits in social interaction and communication, repetitive and stereotyped behavior patterns, and a restricted repertoire of interests and activities.1 Developmental abnormalities are also characteristic of autism, which can be detected in the first three years of life and persist into adulthood.2 Despite its importance, the etiology of ASD remains unknown. It is believed to be multifactorial, associated with genetic and neurobiological factors, i.e., physiological or anatomical abnormality of the central nervous system, innate constitutional problems, and interaction between multiple genes.2,3
Autism represents a pervasive developmental disorder of utmost importance due to its high prevalence. Worldwide epidemiological data estimate that one in every 88 live births has ASD, affecting more male than female individuals. In Brazil, in 2010, it was estimated that approximately 500,000 individuals had autism.3
The diagnosis of ASD is essentially clinical, attained based on observations of the child, parental interviews, and application of specific tools. The criteria used to diagnose ASD are described in the Diagnostic and Statistical Manual of the American Psychiatric Association (DSM).4 These criteria have evolved over the years. The DSM-V, launched in May of 2013, is the newest tool to guide medical diagnosis of individuals with ASD.1,5 In addition to the DSM-V, there are other screening tests for ASD, such as the Childhood Autism Rating Scale (CARS), the Clinical Risk Indicators for Early Childhood Development, and the Modified Checklist for Autism in Toddlers.3,6
Childhood autism involves severe and early changes in the areas of socialization, communication, and cognition. The resulting scenarios are usually severe and persistent, with large individual variations, but often requiring extensive care and permanent commitments from the families.7
Parents of children with ASD are faced with a new situation that requires family adjustment. The fantasized desire of pregnancy must be adjusted to the individual who is born, and who has his/her own characteristics.8 Children diagnosed with ASD often exhibit a greater degree of cognitive impairment and difficulty in interpersonal relations. Consequently, they require special care, including adaptations in formal education and upbringing as a whole.
These particularities lead to changes in family dynamics, requiring careful and prolonged care by all family members who live with a child with ASD. Thus, increased levels of stress are frequently reported, which can impact the quality of life of all family members.9,10 The child's special condition requires that parents face the loss of the idealized child and develop coping strategies to deal with the new reality. The interaction of parents with specific manifestations of ASD in their children can often lead to the family's marginalization regarding social life.8
In 2013, the Brazilian Ministry of Health published the Guidelines for the Care and Rehabilitation of Individuals with ASD, in order to guide health professionals as well as family members in the early identification of autism in children as young as 3 years of age.11
Despite the relevance of this topic, the number of scientific publications on the care of children with ASD from the perspective of their family members is still scarce.4 Velloso,12 in a systematic review, observed that only 93 Brazilian scientific articles on ASD were produced between 2002 and 2009; among these, only 21 articles made reference to the communication skills of children with ASD and their interaction with their families. This same study demonstrated that the Brazilian scientific production on ASD does not meet the country's demand.
Considering the psychodynamic conceptualization of ASD and recognizing the complexity of the family situation, the present study consists of a systematic review of scientific literature on the challenges experienced by families of children with ASD in Brazil and the strategies used to overcome these challenges.
MethodsThis study performed a systematic review of scientific literature on the challenges faced by families living with and caring for children with ASD in Brazil, and their coping strategies. The authors performed searches of systematic and non-systematic reviews in the literature, quantitative-qualitative and qualitative studies, and case reports published until September of 2013 in Portal BVS (Virtual Health Library), SciELO (Scientific Electronic Library Online), Cochrane Database, CAPES journals (Coordination of Improvement of Higher Education Personnel), scientific journals of the area, websites of the Brazilian Ministry of Health, DATASUS (Department of Informatics the Health System), IBGE (Brazilian Institute of Geography and Statistics), and the references of the included articles.
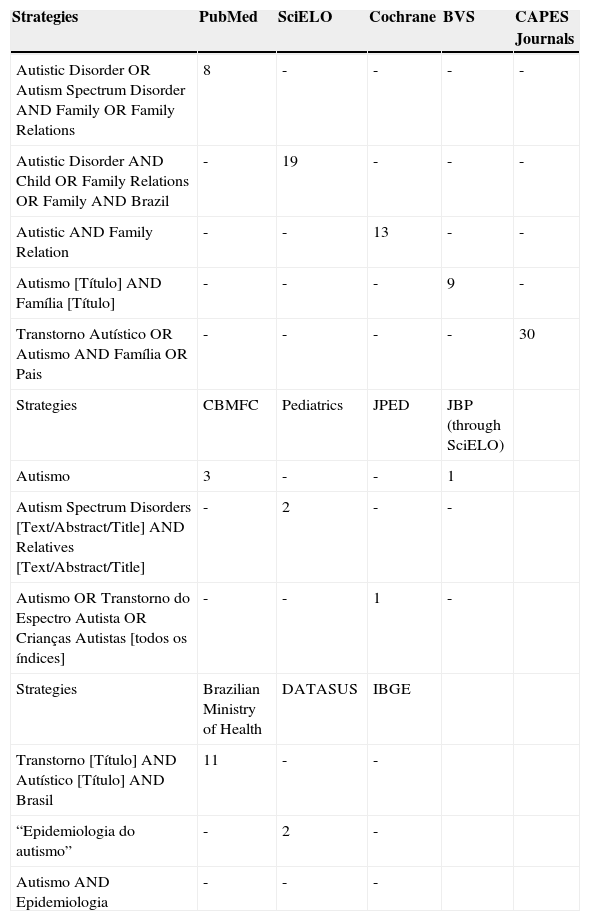
A PICO (acronym for Patient, Intervention, Comparison and Outcomes) model was used for the formulation of the research question, namely: “what are the challenges faced by families of children with ASD and their coping strategies in Brazil?”. The following health descriptors for research and related terms were derived from DeCS and used to construct search strategies applicable at Portal BHS and SciELO: Transtorno Autístico, Autismo, Família, Pais, Transtorno do Espectro Autista, Crianças Autistas, Epidemiologia do Autismo, Epidemiologia. The following descriptors were derived from MeSH and comprised the search strategy at MEDLINE (via PubMed): Autistic Disorder, Autism Spectrum Disorder, Family, Family Relations, Child, Autistic, Autism Spectrum Disorders, Relatives. The descriptors found in MeSH and DeCS comprised the search strategies used in the CAPES Portal, in the annals of the Brazilian Congress of Family and Community Medicine (CBMFC), and specific journals and publications such as O Jornal de Pediatria (JPED), Pediatrics, and the Brazilian Journal of Psychiatry (JBP) via SciELO (Table 1).
Study search strategies.
| Strategies | PubMed | SciELO | Cochrane | BVS | CAPES Journals |
|---|---|---|---|---|---|
| Autistic Disorder OR Autism Spectrum Disorder AND Family OR Family Relations | 8 | - | - | - | - |
| Autistic Disorder AND Child OR Family Relations OR Family AND Brazil | - | 19 | - | - | - |
| Autistic AND Family Relation | - | - | 13 | - | - |
| Autismo [Título] AND Família [Título] | - | - | - | 9 | - |
| Transtorno Autístico OR Autismo AND Família OR Pais | - | - | - | - | 30 |
| Strategies | CBMFC | Pediatrics | JPED | JBP (through SciELO) | |
| Autismo | 3 | - | - | 1 | |
| Autism Spectrum Disorders [Text/Abstract/Title] AND Relatives [Text/Abstract/Title] | - | 2 | - | - | |
| Autismo OR Transtorno do Espectro Autista OR Crianças Autistas [todos os índices] | - | - | 1 | - | |
| Strategies | Brazilian Ministry of Health | DATASUS | IBGE | ||
| Transtorno [Título] AND Autístico [Título] AND Brasil | 11 | - | - | ||
| “Epidemiologia do autismo” | - | 2 | - | ||
| Autismo AND Epidemiologia | - | - | - |
After data tabulation, relevant articles were selected by reading the titles and abstracts, based on the following inclusion criteria: Brazilian studies on children with ASD diagnosis and/or that addressed family interaction with these children. The exclusion criteria included studies involving children with neurological/psychiatric diagnoses other than ASD and studies conducted in countries other than Brazil. When the reading of the title and abstract was not sufficient to determine its inclusion, the article was read in full (Fig. 1).

Initially, the search was performed in the abovementioned databases, resulting in 71 articles, including four in duplicate, and thus 67 articles remained. At a second selection phase, the titles and abstracts of the remaining 67 articles were read, resulting in the exclusion of 42 articles, yielding 25 articles. At the third and final selection phase, the inclusion and exclusion criteria were applied to the full text of the remaining 25 articles and eight articles were selected. One article found by searching the reference lists of the previously included articles was added. Finally, one article indicated by an expert was added to the others, totaling ten articles.
The search, selection, and extraction of data from the included articles were performed by two independent investigators who resolved disagreements by consensus and, when necessary, a third investigator's opinion was requested. The CASP/Oxford13 (Critical Appraisal Skills Programme) and AMSTAR14 tools (Assessment of Multiple Systematic Reviews) were used to assess the methodological quality of qualitative and qualitative-quantitative studies, and systematic reviews, respectively. Case reports and non-systematic reviews were not assessed for methodological rigor, due to the lack of valid tools for this purpose.
ResultsThis review included ten articles published in Portuguese, English, and Spanish, consisting of a systematic review and a non-systematic review, seven qualitative-quantitative and qualitative studies, and one case report. The articles included the participation of siblings, fathers, and mothers of children with ASD. Of the ten articles included, all were carried out in the South and Southeast regions, with four performed in Rio Grande do Sul, and the others in the state of São Paulo.
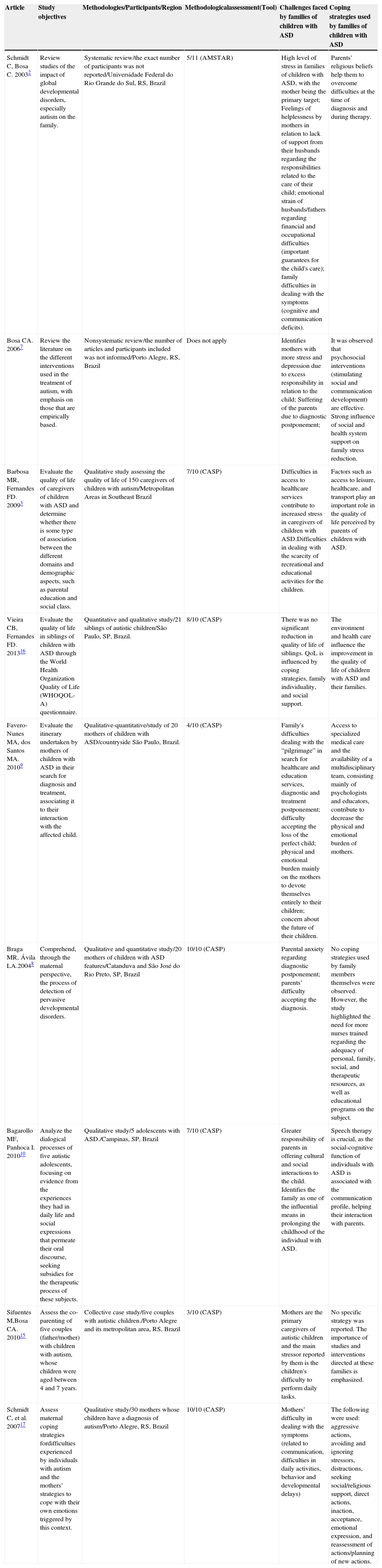
Of the studies assessed using CASP, two9,15 (20%) had scores lower than five (4/10 and 2/10) and five3,8,10,16,17 (50%) had scores higher than five (between 7/10 and 10/10). The systematic review2 received a score of 5/11 by AMSTAR. The main objectives of the studies included were: to assess the quality of life of individuals with ASD, as well as individuals living with them (50% of articles); and to analyze the impact of the search for diagnosis, the diagnosis, and the therapeutic strategies in families of ASD patients (30% of the articles; Table 2).
Main challenges and coping strategies in families of children with ASD.
| Article | Study objectives | Methodologies/Participants/Region | Methodologicalassessment(Tool) | Challenges faced by families of children with ASD | Coping strategies used by families of children with ASD |
|---|---|---|---|---|---|
| Schmidt C, Bosa C. 20032 | Review studies of the impact of global developmental disorders, especially autism on the family. | Systematic review/the exact number of participants was not reported/Universidade Federal do Rio Grande do Sul, RS, Brazil | 5/11 (AMSTAR) | High level of stress in families of children with ASD, with the mother being the primary target; Feelings of helplessness by mothers in relation to lack of support from their husbands regarding the responsibilities related to the care of their child; emotional strain of husbands/fathers regarding financial and occupational difficulties (important guarantees for the child's care); family difficulties in dealing with the symptoms (cognitive and communication deficits). | Parents’ religious beliefs help them to overcome difficulties at the time of diagnosis and during therapy. |
| Bosa CA. 20067 | Review the literature on the different interventions used in the treatment of autism, with emphasis on those that are empirically based. | Nonsystematic review/the number of articles and participants included was not informed/Porto Alegre, RS, Brazil | Does not apply | Identifies mothers with more stress and depression due to excess responsibility in relation to the child; Suffering of the parents due to diagnostic postponement; | It was observed that psychosocial interventions (stimulating social and communication development) are effective. Strong influence of social and health system support on family stress reduction. |
| Barbosa MR, Fernandes FD. 20093 | Evaluate the quality of life of caregivers of children with ASD and determine whether there is some type of association between the different domains and demographic aspects, such as parental education and social class. | Qualitative study assessing the quality of life of 150 caregivers of children with autism/Metropolitan Areas in Southeast Brazil | 7/10 (CASP) | Difficulties in access to healthcare services contribute to increased stress in caregivers of children with ASD.Difficulties in dealing with the scarcity of recreational and educational activities for the children. | Factors such as access to leisure, healthcare, and transport play an important role in the quality of life perceived by parents of children with ASD. |
| Vieira CB, Fernandes FD. 201316 | Evaluate the quality of life in siblings of children with ASD through the World Health Organization Quality of Life (WHOQOL-A) questionnaire. | Quantitative and qualitative study/21 siblings of autistic children/São Paulo, SP, Brazil. | 8/10 (CASP) | There was no significant reduction in quality of life of siblings. QoL is influenced by coping strategies, family individuality, and social support. | The environment and health care influence the improvement in the quality of life of children with ASD and their families. |
| Favero-Nunes MA, dos Santos MA. 20109 | Evaluate the itinerary undertaken by mothers of children with ASD in their search for diagnosis and treatment, associating it to their interaction with the affected child. | Qualitative-quantitative/study of 20 mothers of children with ASD/countryside São Paulo, Brazil. | 4/10 (CASP) | Family's difficulties dealing with the “pilgrimage” in search for healthcare and education services, diagnostic and treatment postponement; difficulty accepting the loss of the perfect child; physical and emotional burden mainly on the mothers to devote themselves entirely to their children; concern about the future of their children. | Access to specialized medical care and the availability of a multidisciplinary team, consisting mainly of psychologists and educators, contribute to decrease the physical and emotional burden of mothers. |
| Braga MR, Ávila LA.20048 | Comprehend, through the maternal perspective, the process of detection of pervasive developmental disorders. | Qualitative and quantitative study/20 mothers of children with ASD features/Catanduva and São José do Rio Preto, SP, Brazil | 10/10 (CASP) | Parental anxiety regarding diagnostic postponement; parents’ difficulty accepting the diagnosis. | No coping strategies used by family members themselves were observed. However, the study highlighted the need for more nurses trained regarding the adequacy of personal, family, social, and therapeutic resources, as well as educational programs on the subject. |
| Bagarollo MF, Panhoca I. 201010 | Analyze the dialogical processes of five autistic adolescents, focusing on evidence from the experiences they had in daily life and social expressions that permeate their oral discourse, seeking subsidies for the therapeutic process of these subjects. | Qualitative study/5 adolescents with ASD./Campinas, SP, Brazil | 7/10 (CASP) | Greater responsibility of parents in offering cultural and social interactions to the child. Identifies the family as one of the influential means in prolonging the childhood of the individual with ASD. | Speech therapy is crucial, as the social-cognitive function of individuals with ASD is associated with the communication profile, helping their interaction with parents. |
| Sifuentes M,Bosa CA. 201015 | Assess the co-parenting of five couples (father/mother) with children with autism, whose children were aged between 4 and 7 years. | Collective case study/five couples with autistic children./Porto Alegre and its metropolitan area, RS, Brazil | 3/10 (CASP) | Mothers are the primary caregivers of autistic children and the main stressor reported by them is the children's difficulty to perform daily tasks. | No specific strategy was reported. The importance of studies and interventions directed at these families is emphasized. |
| Schmidt C, et al. 200717 | Assess maternal coping strategies fordifficulties experienced by individuals with autism and the mothers’ strategies to cope with their own emotions triggered by this context. | Qualitative study/30 mothers whose children have a diagnosis of autism/Porto Alegre, RS, Brazil | 10/10 (CASP) | Mothers’ difficulty in dealing with the symptoms (related to communication, difficulties in daily activities, behavior and developmental delays) | The following were used: aggressive actions, avoiding and ignoring stressors, distractions, seeking social/religious support, direct actions, inaction, acceptance, emotional expression, and reassessment of actions/planning of new actions. |
*The tenth article12 was used only for the analysis of the Brazilian scientific literature on ASD and not for data extraction.
The literature describes the emotional overload experienced by parents as one of the major challenges faced by families with children diagnosed with ASD.8 It is noteworthy that five (50%) articles showed greater physical and psychological stress on the part of the mothers. The main factors responsible for increased parental emotional overload were classified into six categories, namely:
Diagnostic postponementThe authors observed the families’ pilgrimage to hospitals and visits to countless health care professionals to obtain the diagnosis. In Brazil, ASD diagnosis during the preschool years is still very rare. However, at 3 years of age, children tend to meet the criteria for autism.7,11 It is worth mentioning that early diagnosis and intervention result in more adequate intervention and treatment plans that will allow a better quality of life for children diagnosed with ASD until they reach adulthood.1 According to the 2013 Brazilian Care Guidelines for Rehabilitation of Individuals with ASD, therapeutic responses are more significant when treatment is started earlier. To assist in the early identification of ASD, the Ministry of Health developed a table with child development indicators and early warning signs.11 Nevertheless, it is observed that the therapeutic decision and diagnostic postponement are still sources of stress for family members and caregivers of children with ASD, and induce parents’ feelings of helplessness and hopelessness.9 Three studies (30%), including one with high methodological quality,8 indicated diagnostic postponement as a triggering factor of family stress.7–9
Difficulty dealing with the diagnosis and symptomsThe diagnosis of ASD triggers feelings of worthlessness by the parents for the loss of the healthy child.18 Three (30%) studies, including one with high methodological quality,17 showed that behavior, insufficient communication, and cognitive deficits are the symptoms more often related to parental stress.2,15,17
Poor access to health services and social supportPoor access to health care services and social support emerged in three (30%) articles, including one with moderate methodological quality,3 as contributing factors to increased stress and decreased quality of life of caregivers of children with ASD.3,7,9
Scarcity of leisure and educational activitiesParents reported in two studies3,9 (20%), including one with moderate methodological quality,3 the lack of leisure and education activities available to their children as factors impairing the caregivers’ quality of life, as the caregivers become the main providers of education and social relations for their children.
Financial situationAn increase in parents’ working hours to meet financial needs is observed.19 In addition to increased expenses with therapy and education aimed at the autistic child, caregivers must also rely on their employer's understanding of the child's needs.1 Moreover, two2,19 (20%) studies, including one with moderate methodological quality,2 demonstrated that some mothers gave up their professional careers to care for the child, resulting in a reduction of their financial contribution to the household. When they do not stop working, they may receive 35% less in comparison to mothers of children with other health limitations and up to 56% less than mothers of children with no health limitations.19
Concerns about the futureOne (10%) article,9 with moderate methodological quality, indicated obvious parental concern about the future of these children, due to their limitations in providing their own support.9
When the diagnosis and treatment plans are established, families feel comforted.9 For a therapeutic plan to be well developed, suggestions from the health care team and family decisions are necessary, in addition to the well-established diagnosis.11 However, there is a demand for easier access to health care, aiming at better quality of life and less anxiety for the parents.
It is necessary that the care is performed at the three levels of the health care system by professionals trained to identify and evaluate early symptoms in children with ASD. Human resources (training and sensitization of health professionals,8 such as nurses,8 psychologists,9 audiologists,10 specialized clinicians and other professionals,9,16 all working in interdisciplinary teams; as well as social groups coordinated by professionals to assist parents7 and better prepared teachers7 at schools) and material resources (investment in research for the validation and creation of more specific diagnostic tools7 and taking into account the child's health care records)8 must be spent to meet the needs of these children and families that seek their child's diagnosis and treatment.
The start of the family's interaction with a child diagnosed with ASD forces them to face a reality that it is still unknown,20 indicating the challenge of adjusting their plans and expectations for the future, in addition to the need to adapt to the intense dedication and care required by the child's specific needs.2
According to the Brazilian Ministry of Health,11 treatment plans are developed to meet not only the needs of the children with ASD, but also the demands and interests of their families. The articles included showed strategies that help families to live with the symptoms exhibited by children with ASD, aiming to enhance the quality of life of parents and family members and optimize the diagnostic formulation. Among them are: adequate and multidisciplinary medical care,9,10,16 search for social support7,9,17 (such as joining support groups for parents,21 access to leisure, and entertainment activities,3 and religious beliefs).1,10
In high-income countries, families of children with ASD are evaluated, and when necessary, interventions are performed. According to the specific needs of caregivers or family members of children with ASD, they are offered the following: personal, social, and emotional support for their role as caregivers (including rest and emergency plans); planning of future interventions; information; and advice from several support groups.22 However, effective interventions for early detection still need to be confirmed.23
In Brazil, the Ministry of Health provides therapeutic options at Care Units of the Health Care Network for Individuals with Disability, which are part of the public health care network. They offer individual consultations for rehabilitation/habilitation with medical and dental care, as well as language, behavioral, emotional, and practical life activity interventions.
Parents and caregivers are also offered support, guidance, and even specific therapeutic care services, considering the abovementioned stress situation experienced by the families. However, it can be observed that this service is a source of dissatisfaction on the part of assisted families, indicating the need for improved access and quality.11
It is essential that healthcare professionals always assist these families, providing support and guidance for those living with a child diagnosed with ASD, intervening whenever necessary (also by offering complementary and alternative practices),24 as the extensive and/or permanent periods of dedication required by these children, in many cases, result in the decrease of work and leisure activities and even neglect of the health care of the other family members.11
Studies in the literature have demonstrated that the integrated performance of professionals such as psychologists, nurses, physicians, audiologists, and teachers in family dynamics results in improved quality of life and in the capacity of caregivers to cope with the symptoms of patients with ASD. In this sense, the networking, the integrality, and the continuity of health care services may constitute a set of references capable of accommodating these children and their families.
Difficulties in access to health care services and adequate social support contribute to increased levels of stress for caregivers of children diagnosed with ASD.3,8 The exchange of information at the interpersonal level in strategies such as group dynamics2 is able to provide emotional support and help such families to be more resilient in relation to the demand for restructuring and dedication to their children, as well as help them feel socially included and accepted.25–27
The lack of educational and leisure services for children diagnosed with ASD directly affects the quality of life of these children's parents.3 It can be observed that higher investment and provision of services associated with the improvement of the physical space used by children with ASD, such as the availability of specific computerized communication devices for autistic individuals and the creation of spaces for recreation, such as playgrounds and swimming pools in schools for greater interaction with other children,7 may also be helpful in relieving the stress observed in families of children with ASD.
According to the National Institute for Health and Care Excellence (NICE), improving the physical environment of the child with ASD, providing pleasant visual aids such as pictures, words, or symbols, and making adaptations in this environment, considering individual sensory sensitivities to light, noise, and the color of walls and furniture can minimize negative impacts on the children with ASD, improving their quality of life.28–30
In the United Kingdom, children with ASD are followed from infancy to adulthood. Children and adolescents have full access to health and social care services, which consists of trained professionals to deal specifically with children diagnosed with ASD. According to NICE, the ideal treatment to be provided to these children takes into account their individual needs, as well as those of their families. In this sense, among other things, the treatment involves psychosocial interventions and development of skills, aiming to increase the social communication capacity and the insertion of children with ASD into the community, and prevention of behaviors and situations that intimidate them, i.e., the assessment of factors that may cause discomfort to the patient and the treatment of other health problems.28,30
ConclusionChildren with ASD may show early and severe symptoms in the areas of socialization, communication, and cognition. Before the diagnosis, their families live with the challenge of searching for the identification of the disorder, and after the diagnosis, new difficulties arise, such as coping with the symptoms and poor health care, education, and leisure services. The initial interaction with the child with ASD requires the restructuring of family arrangements, which often causes emotional and physical overload to its members, especially to the mother, reducing the quality of life of all family members. The family overload can be mitigated by attaining an effective and timely diagnosis, improving the knowledge about the disease, sharing the establishment of appropriate care plans, and improving the social support network for children with ASD and their families.
As for the health professionals, permanent awareness, training, and updating of pediatricians, family and community doctors and other health professionals on the subject are needed.
Regarding public systems and services, the Brazilian Unified Health System has advanced by publishing its guideline,11 which should direct professional activities and inform the families of children diagnosed with ASD. Its implementation on a national scale, however, requires more from the involved professionals. At the moment, its poor implementation undermines its potential to support individuals with ASD and their caregivers, making family life and the overcoming of the challenges faced by these families even more difficult. In this context, it becomes essential that the Brazilian Unified Health System provide care to patients with ASD, by guiding families and providing strategies for social support by trained professionals, and offering access to leisure and entertainment activities, with consequent gains in the health and quality of life of these individuals.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Rosa Malena Delbone de Faria, José Barbosa Junior, and Kely A. Alves for institutional support for the present research. They thank Mariana Pacelli and Paula C. Caetano for the initial support for the conception of the review.
Please cite this article as: Gomes PT, Lima LH, Bueno MK, Araújo LA, Souza NM. Autism in Brazil: a systematic review of family challenges and coping strategies. J Pediatr (Rio J). 2015;91:111–21.
Study conducted at Universidade José do Rosário Vellano (UNIFENAS), Belo Horizonte, MG, Brazil





