
To estimate the association between maternal socioeconomic factors and the occurrence of nutritional outcomes in children under five years of age in a representative sample of the Brazilian population.
MethodsThis was a cross-sectional study that evaluated data from the latest National Survey of Children and Women's Demographics and Health, carried out in Brazil in 2006–2007. Maternal employment and maternal level of schooling were the main exposures. The following nutritional outcomes in children were considered: height/age <−2 standard deviations (SD) for short stature and BMI/age >2SD for overweight. Generalized estimating equations (GEE) were utilized as the regression method.
ResultsAfter adjustments, it was observed that children whose mothers had low level of schooling had a higher chance of having short stature (OR=3.97, 95% CI, 1.23–12.80) and children whose mothers worked outside the home were more likely to have excess weight (OR=1.57, 95% CI, 1.02–2.42). Maternal employment was not associated with short stature in children (OR=1.09, 95% CI, 0.67–1.77).
ConclusionMaternal level of schooling was associated with short stature in children and maternal employment with overweight, indicating the need to take into account the socioeconomic factors when proposing programs and strategies aimed at health and nutrition improvement of children, considering inter-sectoral interventions.
Estimar a associação entre fatores socioeconômicos maternos e a ocorrência de desfechos nutricionais nas crianças menores de cinco anos em uma amostra representativa da população brasileira.
MétodosTrata-se de um estudo transversal que avaliou dados da última Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher, realizada no Brasil em 2006-2007. Trabalho materno e escolaridade materna foram as exposições principais. Considerou os seguintes desfechos nutricionais nas crianças: estatura/idade <−2 desvios padrão (DP) para baixa estatura e IMC/idade >2DP para excesso de peso. Utilizou-se o método regressão de equações de estimação generalizadas (GEE).
ResultadosApós ajustes, observou-se que crianças cujas mães possuíam baixa escolaridade tiveram maiores chances de baixa estatura (OR=3,97; IC 95% 1,23-12,80) e crianças cujas mães trabalhavam fora de casa apresentaram maior chance de excesso de peso (OR=1,57; IC 95% 1,02-2,42). O trabalho materno não se associou a baixa estatura em crianças (OR=1,09; IC 95% 0,67-1,77).
ConclusãoEscolaridade materna associou-se à baixa estatura nas crianças e trabalho materno ao excesso de peso, indicando a necessidade de se levar em conta os fatores socioeconômicos na proposta de programas e estratégias de melhorias da saúde e nutrição das crianças, tendo em vista intervenções intersetoriais.
The increasing prevalence of childhood excess weight is a global public health problem, a recent phenomenon that has occurred over the past three decades and can affect children's health in the short and long term.1,2 In 2010, the number of overweight children worldwide was 42 million; it increased around 10–40% in most developing countries over the last 10 years, being more prevalent in the age group of five and six years of age.3 A population-based survey performed in Brazil estimated that 7.3% of children under five years of age were overweight, with a higher prevalence in the South of Brazil (9.7%).4
On the other hand, short stature is also a public health problem in Brazil5 and in most developing countries, often associated with childhood morbimortality.6–8 In Brazil, there has been a significant reduction in its prevalence, which was attributed to improved sanitation, increased maternal level of schooling, greater access to health care and consumer goods, and the decline in fertility.9
Among the factors jointly attributed to malnutrition in the long-term and childhood excess weight, one may cite weight gain during pregnancy, inadequate child nutrition, single mother, parental overweight, pre-pregnancy weight, physical inactivity, lack of breastfeeding, and greater inclusion of women in the labor market.3,8–10
Maternal employment affects the mother–child relationship and family dynamics, as it makes it difficult to conciliate time for household chores, work outside the home, and care for the children.11 In low- and middle-income countries, economic crisis exercises greater pressure toward the participation of women in the labor market as a source of supplemental family income. Additionally, low social investments and the lack of infrastructure for child care in these countries overburden women, who are responsible for domestic and economic activities of the family. Such a situation can result in harm to the child, such as less contact with the mother and impaired growth and development.12
The association between maternal employment and childhood excess weight has been observed mainly in populations of developed countries. Studies have shown that maternal employment is associated with an increased risk of weight gain in children2,13,14; on the other hand, the association between maternal employment with nutritional deficit in the long term has been demonstrated in populations from South Asia and Africa.15,16
In addition to maternal employment, maternal level of schooling is one of the main factors that can influence children's growth and development.17,18 For instance, a population-based study in Brazilian children younger than five years found a higher prevalence of excess weight as there was an increase in the number of years of schooling of their mothers.19
Although different studies have confirmed the association between socioeconomic factors and nutritional outcomes in children, they have done so in restricted population groups with low population representativeness, having limited external validity. Therefore, this study aimed to estimate the association between maternal socioeconomic factors (maternal employment and maternal level of schooling) and the occurrence of nutritional outcomes (short stature and excess weight) in children under five years of age from a representative sample of the Brazilian population.
MethodsThis cross-sectional study was performed with data obtained from the latest National Survey of Children and Women's Demographics and Health (PNDS), carried out between 2006 and 2007 in Brazil. This was a nationwide survey that used complex probability sampling, whose main objective was to characterize the female population of childbearing age and children under five years of age, according to demographic, socioeconomic, and cultural factors.6 More information about the detailed sampling plan and on the data collection can be obtained from the PNDS report.5 The manner in which the mother and child databases were correlated and edited has been previously described in detail.20 The anthropometric measurements of mothers and children were carried out following internationally-standardized procedures.21
For the purpose of this study, women who had a valid answer to the questions that addressed maternal employment and maternal level of schooling, mothers with live births from 2001 who were alive at the date of the interview, were living with their mothers, were younger than five years of age, and who had plausible data on z-scores of anthropometric indices were selected. Therefore, of the available sample (n=6724) women who reported failed pregnancies from 2001 (cases of miscarriage and fetal deaths) (n=594), women whose children were older than five years of age (n=1081), had children who died (n=114), who did not live with their mothers at the time of the interview (n=178), with z-score values below and above the standards (−5≤ and >5) for the anthropometric indices (n=68), children with missing anthropometric data (n=7), mothers with invalid answers to the variable “works in addition to domestic activities” (n=2), and maternal level of schooling (and =23) were excluded, resulting in a total of 4356 women with their children under five years of age. It is noteworthy that some individuals did not have complete data for all other variables used in the analyses.
Nutritional outcomes of interest were: (a) short stature, as measured by the z-score of the height/age (HAz) indicator and (b) excess weight, as measured by the z-score of the body mass index/age (BMIz) indicator. Short stature was considered when HAz index was less than −2 z-scores22 and excess weight when BMIz index was greater than 2 z-scores.22 These z-scores were calculated using the standard reference curves of the World Health Organization.22
Paid maternal employment and maternal level of schooling were defined as the main exposures of interest for this study and characterized as follows: maternal employment (categorized as zero, if the mother did not work in addition to domestic activities, and 1 if the mother worked in addition to the domestic activities) and maternal level of schooling (categorized as 0–8, 9–11, 12 or more years of study).
To identify potentially confounding variables, two criteria were used: the theoretical, based on the literature on which this study is founded, and the statistical one. Therefore, to be included in the model, these variables should disclose an association both in the outcome and in the main exposure at a significance level of 0.20 (p≤0.20),23 such as maternal age (categorized as 15–19; 20–29; 30–39; 40–49 years), marital status (married, single, widowed/divorced), breastfeeding (mother breastfed her child, yes or no), area of residence (urban or rural), number of children (1, 2, or ≥3), maternal BMI (categorized as normal weight, malnourished, overweight, and obesity) and region of residence (categorized as Southeast, South, North, Northeast, and Midwest).
When the data analysis was performed, a descriptive analysis was first carried out, which calculated absolute and relative frequencies of the study variables. Then, to assess the association between exposures of interest and nutritional outcomes, a regression analysis method of generalized estimating equations (GEE) was used, which considers the potential correlation between observations of children born to the same mother.24
Multivariate models were estimated for each outcome, which included the exposures of interest and confounding variables. For the GEE models, the binomial error distribution, logit link function, and uniform correlation matrix were used, indicating a correlation structure that is equal between the observations of children born to the same mother, considering the sample weight of the PNDS. In each model, the odds ratios and the standard errors were calculated, which were used for the construction of 95% confidence intervals and level of significance <5% (p<0.05). Data were processed and analyzed using the Statistical Software for Professionals (SPSS for Windows, version 12.1, SPSS Inc, Stata Corp, USA).
Regarding the ethical aspects, PNDS (2006–2007) was approved by the Research Ethics Committee (CEP) of the STD/AIDS Reference and Training Center of the State Health Secretariat of Sao Paulo (SP). All the individuals who agreed to participate signed the Informed Consent.
ResultsIn the population studied, the mean±standard error (SE) of the children's age was 2 years (±0.03) and 52% (n=2244) were boys. The mean maternal age was 27 years (±0.21). Additionally, 85.0% of the mothers were married or living in a stable relationship, 40% reported working in addition to the domestic activities, and had a mean BMI of 25kg/m2 (±0.15) and 8 years (±0.12) of schooling. In relation to nutritional outcomes, the overall means of the indicators height/age (HAz) and BMI/age (BMIz) z-scores were −0.31 (±0.04) and 0.45 (±0.03), respectively (data not shown).
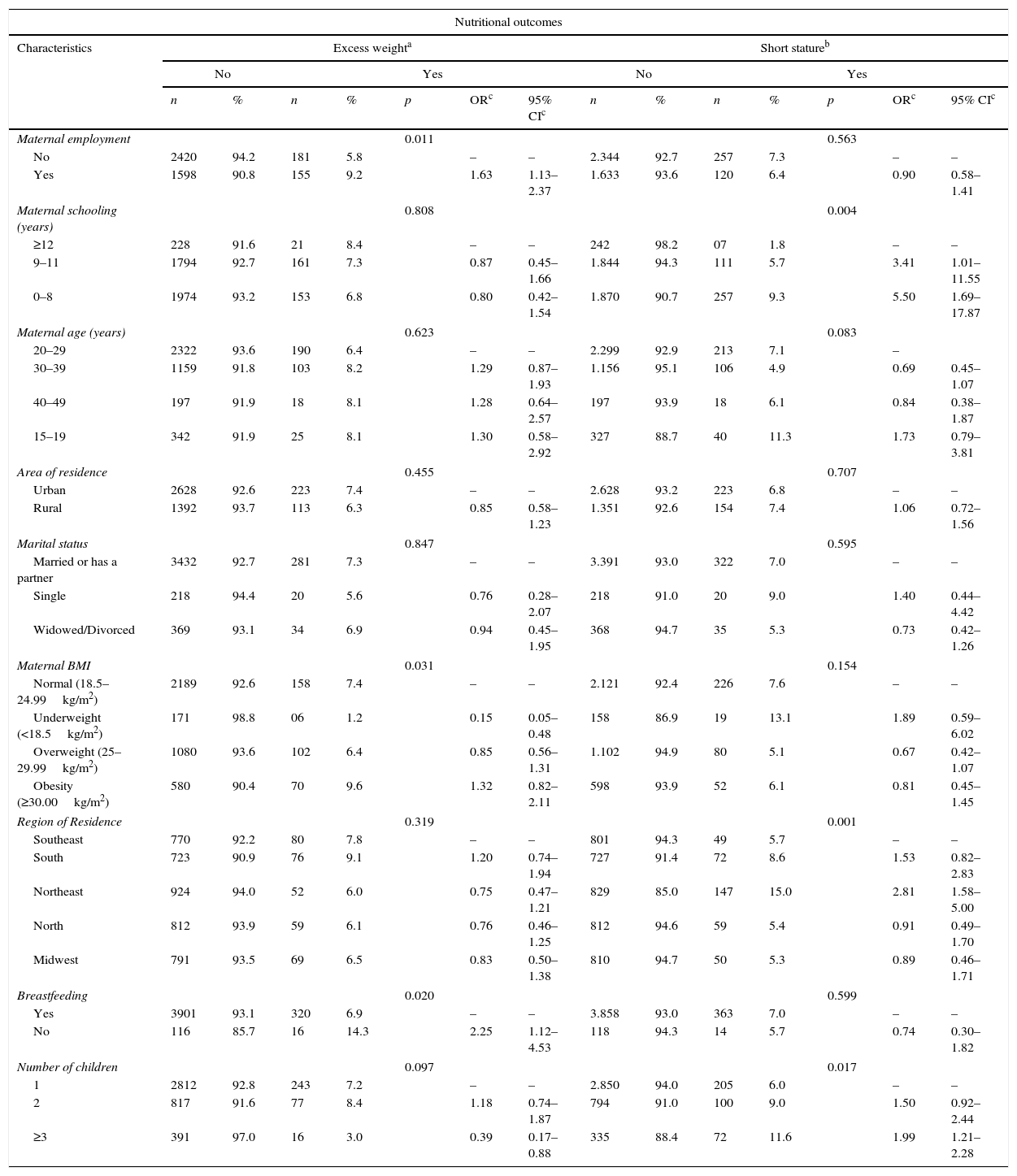
Table 1 describes the proportions of excess weight and short stature in children under five years according to the exposures of interest and covariates, unadjusted odds ratio, and 95% CI of the unadjusted analysis. It was observed that the prevalence of excess weight ranged between 1.2% and 14.3%, lower in the group of mothers considered lean and higher in children whose mothers did not breastfeed. The prevalence of short stature ranged between 1.8% and 15%, lower among children of mothers with higher level of schooling and higher in children living in the Northeast of Brazil (Table 1).
Proportions of excess weight and short stature in children under five years of age according to the exposures of interest and covariates, including unadjusted OR and 95% CI, Brazil, PNDS (2006–2007).
| Nutritional outcomes | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Excess weighta | Short statureb | ||||||||||||
| No | Yes | No | Yes | |||||||||||
| n | % | n | % | p | ORc | 95% CIc | n | % | n | % | p | ORc | 95% CIc | |
| Maternal employment | 0.011 | 0.563 | ||||||||||||
| No | 2420 | 94.2 | 181 | 5.8 | – | – | 2.344 | 92.7 | 257 | 7.3 | – | – | ||
| Yes | 1598 | 90.8 | 155 | 9.2 | 1.63 | 1.13–2.37 | 1.633 | 93.6 | 120 | 6.4 | 0.90 | 0.58–1.41 | ||
| Maternal schooling (years) | 0.808 | 0.004 | ||||||||||||
| ≥12 | 228 | 91.6 | 21 | 8.4 | – | – | 242 | 98.2 | 07 | 1.8 | – | – | ||
| 9–11 | 1794 | 92.7 | 161 | 7.3 | 0.87 | 0.45–1.66 | 1.844 | 94.3 | 111 | 5.7 | 3.41 | 1.01–11.55 | ||
| 0–8 | 1974 | 93.2 | 153 | 6.8 | 0.80 | 0.42–1.54 | 1.870 | 90.7 | 257 | 9.3 | 5.50 | 1.69–17.87 | ||
| Maternal age (years) | 0.623 | 0.083 | ||||||||||||
| 20–29 | 2322 | 93.6 | 190 | 6.4 | – | – | 2.299 | 92.9 | 213 | 7.1 | – | |||
| 30–39 | 1159 | 91.8 | 103 | 8.2 | 1.29 | 0.87–1.93 | 1.156 | 95.1 | 106 | 4.9 | 0.69 | 0.45–1.07 | ||
| 40–49 | 197 | 91.9 | 18 | 8.1 | 1.28 | 0.64–2.57 | 197 | 93.9 | 18 | 6.1 | 0.84 | 0.38–1.87 | ||
| 15–19 | 342 | 91.9 | 25 | 8.1 | 1.30 | 0.58–2.92 | 327 | 88.7 | 40 | 11.3 | 1.73 | 0.79–3.81 | ||
| Area of residence | 0.455 | 0.707 | ||||||||||||
| Urban | 2628 | 92.6 | 223 | 7.4 | – | – | 2.628 | 93.2 | 223 | 6.8 | – | – | ||
| Rural | 1392 | 93.7 | 113 | 6.3 | 0.85 | 0.58–1.23 | 1.351 | 92.6 | 154 | 7.4 | 1.06 | 0.72–1.56 | ||
| Marital status | 0.847 | 0.595 | ||||||||||||
| Married or has a partner | 3432 | 92.7 | 281 | 7.3 | – | – | 3.391 | 93.0 | 322 | 7.0 | – | – | ||
| Single | 218 | 94.4 | 20 | 5.6 | 0.76 | 0.28–2.07 | 218 | 91.0 | 20 | 9.0 | 1.40 | 0.44–4.42 | ||
| Widowed/Divorced | 369 | 93.1 | 34 | 6.9 | 0.94 | 0.45–1.95 | 368 | 94.7 | 35 | 5.3 | 0.73 | 0.42–1.26 | ||
| Maternal BMI | 0.031 | 0.154 | ||||||||||||
| Normal (18.5–24.99kg/m2) | 2189 | 92.6 | 158 | 7.4 | – | – | 2.121 | 92.4 | 226 | 7.6 | – | – | ||
| Underweight (<18.5kg/m2) | 171 | 98.8 | 06 | 1.2 | 0.15 | 0.05–0.48 | 158 | 86.9 | 19 | 13.1 | 1.89 | 0.59–6.02 | ||
| Overweight (25–29.99kg/m2) | 1080 | 93.6 | 102 | 6.4 | 0.85 | 0.56–1.31 | 1.102 | 94.9 | 80 | 5.1 | 0.67 | 0.42–1.07 | ||
| Obesity (≥30.00kg/m2) | 580 | 90.4 | 70 | 9.6 | 1.32 | 0.82–2.11 | 598 | 93.9 | 52 | 6.1 | 0.81 | 0.45–1.45 | ||
| Region of Residence | 0.319 | 0.001 | ||||||||||||
| Southeast | 770 | 92.2 | 80 | 7.8 | – | – | 801 | 94.3 | 49 | 5.7 | – | – | ||
| South | 723 | 90.9 | 76 | 9.1 | 1.20 | 0.74–1.94 | 727 | 91.4 | 72 | 8.6 | 1.53 | 0.82–2.83 | ||
| Northeast | 924 | 94.0 | 52 | 6.0 | 0.75 | 0.47–1.21 | 829 | 85.0 | 147 | 15.0 | 2.81 | 1.58–5.00 | ||
| North | 812 | 93.9 | 59 | 6.1 | 0.76 | 0.46–1.25 | 812 | 94.6 | 59 | 5.4 | 0.91 | 0.49–1.70 | ||
| Midwest | 791 | 93.5 | 69 | 6.5 | 0.83 | 0.50–1.38 | 810 | 94.7 | 50 | 5.3 | 0.89 | 0.46–1.71 | ||
| Breastfeeding | 0.020 | 0.599 | ||||||||||||
| Yes | 3901 | 93.1 | 320 | 6.9 | – | – | 3.858 | 93.0 | 363 | 7.0 | – | – | ||
| No | 116 | 85.7 | 16 | 14.3 | 2.25 | 1.12–4.53 | 118 | 94.3 | 14 | 5.7 | 0.74 | 0.30–1.82 | ||
| Number of children | 0.097 | 0.017 | ||||||||||||
| 1 | 2812 | 92.8 | 243 | 7.2 | – | – | 2.850 | 94.0 | 205 | 6.0 | – | – | ||
| 2 | 817 | 91.6 | 77 | 8.4 | 1.18 | 0.74–1.87 | 794 | 91.0 | 100 | 9.0 | 1.50 | 0.92–2.44 | ||
| ≥3 | 391 | 97.0 | 16 | 3.0 | 0.39 | 0.17–0.88 | 335 | 88.4 | 72 | 11.6 | 1.99 | 1.21–2.28 | ||
The associations of unadjusted analyses observed with excess weight were seen in children of mothers who worked outside the home (OR=1.63, 95% CI, 1.13–2.37) and who breastfed (OR=2.25; 95% CI, 1.12–4.53). Associations with short stature were seen in children whose mothers had low and average levels of schooling (9–11 years: OR=3.41, 95% CI, 1.01–11.55; 0–8 years: OR=5.50; 95% CI, 1.69–17.87), who lived in the Northeast (OR=2.81, 95% CI, 1.58–5.00), and who had more than two children (OR=1.99, 95% CI, 1.21–2.28) (Table 1).
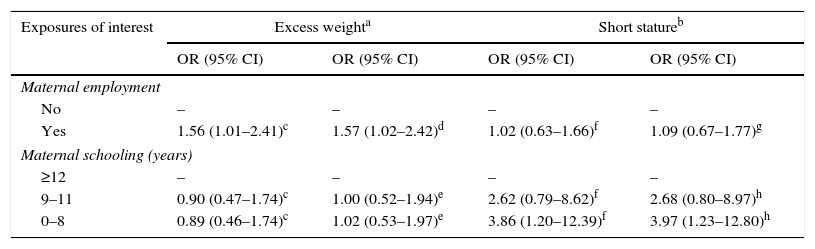
Regarding the multivariate models, a statistically significant association was observed between maternal employment and excess weight in children, after adjusting for maternal age, number of children, breastfeeding, and maternal BMI (OR=1.56, 95% CI, 1.01–2.41). This association remained significant after inclusion of the variable maternal level of schooling in the model (OR=1.57, 95% CI, 1.02–2.42) (Table 2). There was no statistically significant association between maternal level of schooling and excess weight in children.
Adjusted OR and 95% CI for excess weight and short stature in children according to exposures of interest – Brazil, PNDS (2006–2007).
| Exposures of interest | Excess weighta | Short statureb | ||
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Maternal employment | ||||
| No | – | – | – | – |
| Yes | 1.56 (1.01–2.41)c | 1.57 (1.02–2.42)d | 1.02 (0.63–1.66)f | 1.09 (0.67–1.77)g |
| Maternal schooling (years) | ||||
| ≥12 | – | – | – | – |
| 9–11 | 0.90 (0.47–1.74)c | 1.00 (0.52–1.94)e | 2.62 (0.79–8.62)f | 2.68 (0.80–8.97)h |
| 0–8 | 0.89 (0.46–1.74)c | 1.02 (0.53–1.97)e | 3.86 (1.20–12.39)f | 3.97 (1.23–12.80)h |
95% CI, 95% confidence interval; OR, odds ratio.
Model adjusted for maternal age, region of residence, number of children, breastfeeding, and maternal BMI.
Model adjusted for maternal age, region of residence, number of children, breastfeeding, maternal BMI, and maternal education.
Regarding the second outcome of nutritional status, no statistically significant association was observed between maternal employment and short stature (OR=1.09, 95% CI, 0.67–1.77), even after adjustments (Table 2). However, an association was observed between low maternal level of schooling and short stature adjusted for maternal age, region of residence, and number of children (OR=3.86, 95% CI, 1.20–12.39). When maternal employment was included as a potential confounder, the association between maternal level of schooling and short stature remained significant (OR=3.97, 95% CI, 1.23–12.80).
DiscussionIn the present study, no association was observed between maternal employment and short stature in children, a result that is contrary to a survey carried out in a Brazilian community with high social vulnerability,25 which confirmed the protective effect of maternal employment on the nutritional deficit in the long term. It is also known that maternal work can positively influence the child's growth by increasing income, providing improvements in the acquisition of healthy foods, material goods, access to sanitation, and health care services, which are important factors for adequate child growth.11
However, maternal employment was associated with excess weight in children, confirming findings of previous studies that also found that mothers who worked outside the home increased the likelihood of weight gain in children13,26 and the number of hours worked by the mother, a variable not included in this study, was associated with a higher chance of excess weight in their children.2
Several mechanisms can explain the influence of maternal employment on children's weight gain. Mothers who work outside the home have less time to devote to their children and to the preparation of meals, choosing easily-prepared processed foods, which have high caloric value, and avoiding consumption of healthy foods.11 Another possible explanation would be that mothers who work outside the home spend less time in leisure activities with their children than those who do not work. Thus, less energy expenditure increases the risk of excess weight.13 One must also consider that returning to work soon after the birth of the child can also be a barrier to breastfeeding maintenance, leading to early weaning and the consequent introduction of foods of inadequate quality and quantity, contributing to weight gain in the first year of life.13
The present study showed that children of mothers with low level of schooling (0–8 years of study) were more likely to have short stature, corroborating another study that was nationally representative and controlled for important confounding factors6 and with a study carried out in developed countries.17 In Bangladesh, high maternal level of schooling was also associated with favorable growth in children.18 Mothers with higher levels of education are mostly present in the labor market, improving the family socioeconomic status, which may lead to changes in the child's feeding pattern, including greater access to healthy foods rich in nutrients and vitamins, unlike women with lower schooling, who do not have sufficient financial resources to purchase food and to obtain access to the necessary information for the adequate care of the child.11
The present study did not show a significant association between maternal level of schooling and excess weight, although some studies have pointed out that higher maternal schooling positively contributes to the choice of healthy foods for their children, by granting the parents/guardians the ability to assimilate messages from nutrition education programs and understand the importance of food as a means of promoting health, which would reduce the risk of excess weight in this age group.27
Additionally, mothers with higher level of schooling most often spend more time away from home, which causes children to spend most of their time in front of the television, video games, and computers, contributing to weight gain.28 It is very important to understand that such damage is aggravated by the influence of high-calorie food advertisements and the production of images and shapes that draw attention to the consumption of certain foods that do not provide health benefits.29 Another factor that can influence childhood obesity is the safety of the neighborhood, as an association between violence and childhood obesity has been demonstrated, as fear and exposure of children to unsafe environments also contributes to the children's sedentary lifestyle.30
As limitations of the present study, it is emphasized that the models were not adjusted for potential confounding variables used in international studies, such as parental occupation, physical activity of children, hours of sleep, and screen time, as these data were not obtained by the PNDS (2006–2007). This study did not use data related to the children's birth weight, family income, and breastfeeding time, important predictors of excess weight and short stature at the children's age range, due to the relatively high amount of missing data.
Nonetheless, it is worth mentioning that surveys such as PNDS follow standardized procedures, with a representative sample of the Brazilian population. Moreover, the results observed are consistent, as they generally corroborate other similar studies and were analyzed using appropriate statistical methods. Some methodological aspects that can be interpreted as advantages of the present study should also be noted. The potential violation of independence of observations, because of the correlation structure resulting from children of the same family, has been corrected, as the authors used a regression analysis method of generalized estimating equations (GEE), a more conservative method, which incorporates the potential home cluster. It is also important to note that the study was controlled for possible confounding variables in GEE models to evaluate the association between nutritional outcomes and exposures of interest.
It can be concluded that maternal level of schooling was associated with short stature in children and maternal employment with overweight, indicating the need to take into account the socioeconomic factors when proposing programs and strategies aimed at health and nutrition improvement of children, considering inter-sectoral interventions.
Furthermore, the epidemiological importance of these findings is understood, demonstrating the occurrence of the nutritional transition that has taken place in recent decades, with concomitant changes in demographics and morbimortality, which has intensified in poor and developing countries.
Prevention and nutritional monitoring activities and the active participation of schools together with health professionals are required to implement effective interventions for the prevention of childhood obesity and malnutrition. Moreover, public policies are crucial to ensure the human right to adequate food and, consequently, the design, planning, implementation, and management of these policies should support each other, aiming at the transformation of the social problem of these diseases.
FundingPNDS 2006/07 was funded by the Ministry of Health and performed by Centro Brasileiro de Análise e Planejamento (CEBRAP). The authors received project funding from Fundação de Amparo a Pesquisa de Minas Gerais (FAPEMIG) (APQ-00707-14) and TGH would like to thank Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the PhD scholarship.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Géa-Horta T, Felisbino-Mendes MS, Ortiz RJ, Velasquez-Melendez G. Association between maternal socioeconomic factors and nutritional outcomes in children under 5 years of age. J Pediatr (Rio J). 2016;92:574–80.
Study carried out at the Department of Maternal-Child and Public Health, Escola de Enfermagem, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil.




