

To perform the construct validity and the internal consistency of the Maternal Breastfeeding Evaluation Scale tool, aiming at its application in the Brazilian population.
MethodsCross-sectional study that applied the tool to 287 Brazilian women 30 days after childbirth. Main component analysis with varimax rotation was used for the factor analysis, verifying the number of subscales and the maintenance or extraction of the components. Four hypotheses were tested using the unpaired Student's t-test for construct validation. The reliability analysis was performed using Cronbach's alpha coefficient.
ResultsThe exploratory factor analysis identified the need to exclude an item and to reformulate the subscales. The results of the construct validity showed that all hypotheses proposed were confirmed: women who were breastfeeding, those who were exclusively breastfeeding, those who did not have problems related to breastfeeding, and those who intended to breastfeed for at least 12 months achieved significantly higher mean values in the scale. The tool showed adequate internal consistency (Cronbach's alpha=0.88, 95% CI: 0.86–0.90), as did the pleasure and fulfillment of the maternal role subscales (0.92, 95% CI: 0.91–0.93%); child growth, development, and satisfaction (0.70; 95% CI: 0.65–0.75); and maternal physical, social, and emotional aspects (0.75, 95% CI: 0.70–0.79).
ConclusionsThe validation process of the Brazilian version of the Maternal Breastfeeding Evaluation Scale tool showed that it is valid and reliable tool to be applied to the Brazilian population.
Realizar a validação de constructo e avaliar a consistência interna do instrumento Maternal Breastfeeding Evaluation Scale, visando à sua aplicação na população brasileira.
MétodosEstudo transversal com aplicação do instrumento a 287 mulheres brasileiras após 30 dias do nascimento da criança. Para a análise fatorial utilizou-se a análise de componentes principais com rotação varimax, verificando o número de subescalas e a manutenção ou extração dos componentes. Para a validação de constructo quatro hipóteses foram testadas pelo teste T-student não pareado. A análise de confiabilidade foi realizada utilizando o coeficiente de alfa de Cronbach.
ResultadosA análise fatorial exploratória identificou a necessidade de exclusão de um item e a reformulação das subescalas. Os resultados da validade de constructo mostraram que todas as hipóteses propostas foram confirmadas: as mulheres que estavam amamentando, as que estavam em amamentação exclusiva, as que não apresentavam problemas relacionados à amamentação e aquelas com intenção de amamentar por pelo menos 12 meses apresentaram valores médios significativamente superiores na escala. O instrumento apresentou consistência interna adequada (alfa de Cronbach=0,88; IC95%: 0,86-0,90), assim como as subescalas prazer e realização do papel materno (0,92; IC95%: 0,91-0,93), crescimento, desenvolvimento e satisfação infantil (0,70; IC95%: 0,65-0,75) e aspectos físico, social e emocional materno (0,75; IC95%: 0,70-0,79).
ConclusõesO processo de validação do instrumento Maternal Breastfeeding Evaluation Scale/BRASIL constatou que ele é válido e confiável para ser aplicado à população brasileira.
The impact of breastfeeding (BF) on child health is widely known: protection against respiratory infections, diarrhea, dental malocclusion, improved cognitive development, and decreased chances of excess weight and diabetes in the future.1 Additionally, it protects women against breast and ovarian cancer and type 2 diabetes, and increases the interval between deliveries.1,2
The World Health Organization recommends exclusive breastfeeding (EBF) in the first 6 months of life and supplemented breastfeeding up to 2 years or more.3 Regardless of this, the prevalence of breastfeeding worldwide and especially in Brazil is low. The latest national survey estimated that only 37% of children under 6 months are exclusively breastfed, 45% between 12 and 15 months, and 32% between 20 and 23 months.4
In recent years, emphasis has been placed on breastfeeding duration as the indicator of success for this practice. However, for many mothers, breastfeeding success is related not only to its duration, but also to the mutual satisfaction of the mother's and the infant's needs, creating a stronger bond between them and increasing maternal confidence, with a direct impact on breastfeeding duration.5–8
There are very few studies dedicated to the assessment of the degree of women's satisfaction with breastfeeding and little is known about its determinants. Maternal satisfaction with breastfeeding has been high, with more than 75% of postpartum women being satisfied at different moments during breastfeeding and in different countries.7,9,10 In recent studies, early skin-to-skin contact, incentive to on demand feeding in the maternity hospital,11 breastfeeding problems,6 expected and effectively practiced duration,10 and maternal self-esteem7 have been associated with satisfaction.
Currently, to the best of the authors’ knowledge, only one tool is available in the literature to assess the maternal perception of breastfeeding success, the Maternal Breastfeeding Evaluation Scale (MBFES), proposed by Leff, Jefferis and Gagne, in 1994.5 The tool was published in English and validated in the USA,5,12,13 also being used in Canada,14,15 Australia,6,8,16 and Scotland.17 It has been translated and validated in Japan,18,19 Portugal,7,20,21 and Spain.22 To date, there is no record of validation of this tool for the Brazilian population, limiting its use in Brazil.23 Based on the assumption that the women's satisfaction with breastfeeding is very important for its success, although little studied, this study aims to perform the construct validation and evaluate the internal consistency of the tool, aiming at its application in the Brazilian population, thus allowing studies to be carried out that will identify the level of satisfaction of Brazilian women, as well as its determinants.
MethodsA cross-sectional study was carried out with women who delivered their children in maternity hospitals located in Porto Alegre, Brazil, from January to August 2016. One of the institutions, Hospital de Clínicas de Porto Alegre (HCPA), is a school hospital that attends, almost in its entirely, users of the Brazilian Unified Health System (SUS). The other institution, Hospital Moinhos de Vento (HMV), is a private hospital. They are both referral hospitals for typical-risk and high-risk pregnancies.
A simple random sample was selected in the maternity hospitals, including women who had a singleton-pregnancy, live birth newborn with ≥37 weeks of gestational age, living in Porto Alegre, and who had started breastfeeding. Daily, one postpartum woman in the private maternity hospital and two in the public one were randomly selected among the eligible ones, approximately 24h after childbirth. A first contact was made at the maternity hospital to obtain the mother's informed consent and to schedule an appointment after the child completed 30 days of life at her home or another place of preference. Some data were obtained from the medical records.
Two mother-infant pairs with severe obstetric and/or neonatal complications that resulted in death or hospitalization in the Intensive Therapy Unit were excluded, as well as those with health problems that significantly interfered with breastfeeding, such as metabolic diseases or malformations.
The tool was self-administered by the women during visits carried out by trained interviewers, between 31 and 37 days after delivery, together with a questionnaire containing sociodemographic, gestational, postpartum, and child feeding questions in the first 30 days.
The sample size calculation for the validation process followed the recommendation that stipulates the need of seven individuals for each question to be validated.24 Thus, a minimum sample of 210 women was estimated.
Original MBFES versionThe MBFES is a self-administered tool developed to measure the woman's self-perception regarding her satisfaction with breastfeeding. This scale includes items on positive and negative experiences and emotions related to breastfeeding, and consists of 30 self-reported Likert-type items ranging from “strongly disagree” (1 point) to “strongly agree” (5 points). Among the items, 19 are positive affirmations scored as mentioned; and 11 are negative affirmations, with inverse scores (items 3, 5, 8, 13, 14, 15, 19, 22, 27, 28, and 29). It has three dimensions: child satisfaction and growth (3, 4, 7, 10, 15, 19, 24, and 28); maternal lifestyle and body image (5, 8, 13, 14, 22, 26, 27, and 29); and pleasure and fulfillment of the maternal role (1, 2, 6, 9, 11, 12, 16, 17, 18, 20, 21, 23, 25, and 30).5,12 The total score ranges from 30 to 150 points, where higher scores indicate positive evaluation of the breastfeeding experience, expressing greater satisfaction. The MBFES has shown good validity and reliability.5,12
Validation processThe validation process of the Brazilian version of the MBFES was preceded by the authorization of its main creator, Ellen W. Leff.5 For this process, we used the translated and validated version for Portuguese in Portugal.7,20
The next step consisted in applying the tool available in Portuguese to women one month after childbirth. During the application, the researchers were available for the clarification of doubts, should they arise, without interfering in the response. The terms “burden,” “eager,” “high,” and “cow,” showed doubts. The words “heavy,” “avidly,” “fulfillment,” and “milk-producing animal” were used as synonyms in the explanations, respectively.
Data analysisDescriptive data analyses that characterized the sample were carried out according to sociodemographic characteristics,25 and those related to childbirth and breastfeeding (mean and standard deviation for MBFES scores, and absolute and relative frequencies for the other variables). The Kaiser-Meyer-Olkin and Bartlett sphericity tests were performed to evaluate the sample adequacy for the factor analysis.
As part of the validation tests, the exploratory factor analysis of the items was performed, through the analysis of the main components with varimax rotation, to verify the number of subscales and maintenance or extraction of the components. Only items with values >0.4 remained in the tool.26
The construct validation informs whether the tool scores agree with other measures consistent with the theoretical hypotheses known for the topic of interest.24,27 This validation evaluated associations between the MBFES score and the pattern of breastfeeding, weaning, intent regarding duration of breastfeeding, and problems related to breastfeeding in the first month. For this purpose, the unpaired Student's t-test was used for four hypotheses: (1) women who were exclusively breastfeeding in the first month would have higher scores in MBFES than women who were partially breastfeeding; (2) women who were breastfeeding in the first month would have higher scores than women who were not breastfeeding; (3) women intending to breastfeed longer (>12 months) would have higher scores than those who intended to breastfeed for less time (<12 months); (4) women who did not have problems during breastfeeding in the first month would have higher scores than those who did.
To perform these analyses, the authors considered the following: EBF when the child did not receive any food rather than breastmilk, including water, at 30 days; mixed BF when the child received, in addition to breastmilk, another type of milk; and breastfeeding problems when one or more of the following conditions occurred in the first month: breast engorgement, cracked nipple, mastitis, difficulty in getting the baby to latch, insufficient milk supply, and anatomical nipple problems.
For the reliability analysis, the measure of the degree to which the items on the scale (or subscale) of a tool are correlated by measuring the same concept, Cronbach's alpha coefficient was used to verify the internal consistency of the tool and the domains.24 Cronbach's alpha values between 0.70 and 0.95 are considered indicative of positivity for internal consistency.24
The analyses were performed using the software SPSS (IBM SPSS Statistics for Windows, version 21.0, NY, USA).
Ethical aspectsThis study is in compliance with the standards for studies with human subjects28 and was submitted to analysis by the Research Ethics Committees of the HCPA and HMV, being approved under reports No. 1,288,088 and 1,204,288, respectively, in 2015. The participants were included in the study after signing the informed consent.
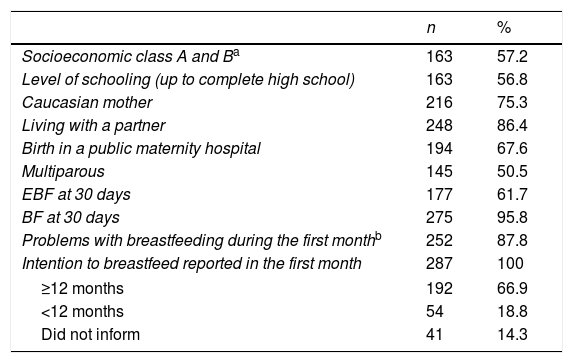
ResultsThe sample consisted of 287 women aged between 16 and 45 years, with a mean of 29±6.6 years. Sociodemographic characteristics and those related to childbirth and breastfeeding are described in Table 1. The prevalence of EBF and BF at the maternity hospital discharge was 81.9% and 98.3%, respectively; and at the end of the first month, 61.7% and 95.8%, respectively.
Sociodemographic characteristics of the sample, and those related to childbirth and breastfeeding, Porto Alegre, RS, Brazil, 2016 (n=287).
| n | % | |
|---|---|---|
| Socioeconomic class A and Ba | 163 | 57.2 |
| Level of schooling (up to complete high school) | 163 | 56.8 |
| Caucasian mother | 216 | 75.3 |
| Living with a partner | 248 | 86.4 |
| Birth in a public maternity hospital | 194 | 67.6 |
| Multiparous | 145 | 50.5 |
| EBF at 30 days | 177 | 61.7 |
| BF at 30 days | 275 | 95.8 |
| Problems with breastfeeding during the first monthb | 252 | 87.8 |
| Intention to breastfeed reported in the first month | 287 | 100 |
| ≥12 months | 192 | 66.9 |
| <12 months | 54 | 18.8 |
| Did not inform | 41 | 14.3 |
The definition of social classes (A, B1, B2, C1, C2, and DE) was carried out using the scoring system used by the Brazilian Association of Research Companies (ABEP) in Critério Brasil 2015, considering the possession of luxury items, potable water at home, street pavement, and level of schooling of the head of the family. Classes A and B represent families with the highest socioeconomic status.25 Two of the women did not report data for classification (missing data).
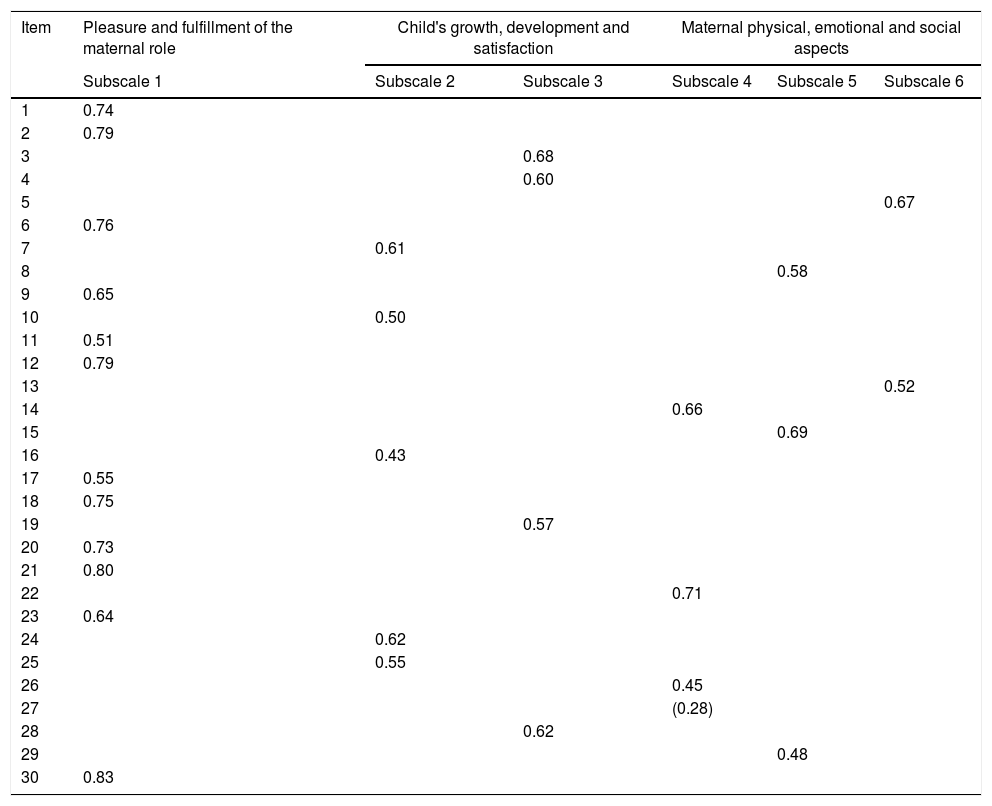
The value of the Kaiser-Meyer-Olkin measure for sample adequacy was 0.91, above that suggested as the minimum required for factor analysis (0.60).29 The result of Bartlett's sphericity test was χ2 (df.435)=4.047.053; p<0.001, indicating that the factor analysis was appropriate. This analysis showed the existence of six domains that explained 58.8% of the tool variability. Since this subdivision had no practical or clinical implications, it was decided to group the subscales by similar subjects, as in the original tool, resulting in the creation of three subscales: pleasure and fulfillment of the maternal role; child growth, development and satisfaction; and maternal physical, social, and emotional aspects.
The new subscales were quite similar to the original ones, differing only in questions 15, 16, 25, and 27. Question 15 “While breastfeeding, I worried about my baby gaining enough weight,” changed subscale, probably because the expression “worried” is not an objective evaluation parameter of the baby's weight gain, but because it represents a maternal feeling of concern regarding this weight gain, being much more related to the maternal emotional aspects; thus, it was included in the new subscale of maternal physical, emotional, and social aspects and no longer in the child satisfaction and growth subscale. Items 16 “Breastfeeding was soothing when my baby was upset or crying” and 25 “Breastfeeding made my baby feel more secure,” which belonged to the subscale pleasure and fulfillment of the maternal role in the original version, changed subscale, becoming part of the child growth, development, and satisfaction subscale, as “soothed my baby” and “felt more secure” are expressions related to baby satisfaction and not to maternal pleasure aspects. Question 27 of the tool, “Breastfeeding made me feel like a cow” had a factor load of 0.28, below the acceptable level, and was excluded from the Brazilian version of the tool (Table 2). Thus the Brazilian version of the MBFES (Supplementary Table 1) resulted in 29 items, with some of them depicting explanations of the terms that generated doubts during the application (5, 7, and 17). The new values for the Brazilian version of the MBFES are shown in Table 3.
New domains and factorial analysis values per major components with varimax rotation of the Brazilian Maternal Breastfeeding Evaluation Scale.
| Item | Pleasure and fulfillment of the maternal role | Child's growth, development and satisfaction | Maternal physical, emotional and social aspects | |||
|---|---|---|---|---|---|---|
| Subscale 1 | Subscale 2 | Subscale 3 | Subscale 4 | Subscale 5 | Subscale 6 | |
| 1 | 0.74 | |||||
| 2 | 0.79 | |||||
| 3 | 0.68 | |||||
| 4 | 0.60 | |||||
| 5 | 0.67 | |||||
| 6 | 0.76 | |||||
| 7 | 0.61 | |||||
| 8 | 0.58 | |||||
| 9 | 0.65 | |||||
| 10 | 0.50 | |||||
| 11 | 0.51 | |||||
| 12 | 0.79 | |||||
| 13 | 0.52 | |||||
| 14 | 0.66 | |||||
| 15 | 0.69 | |||||
| 16 | 0.43 | |||||
| 17 | 0.55 | |||||
| 18 | 0.75 | |||||
| 19 | 0.57 | |||||
| 20 | 0.73 | |||||
| 21 | 0.80 | |||||
| 22 | 0.71 | |||||
| 23 | 0.64 | |||||
| 24 | 0.62 | |||||
| 25 | 0.55 | |||||
| 26 | 0.45 | |||||
| 27 | (0.28) | |||||
| 28 | 0.62 | |||||
| 29 | 0.48 | |||||
| 30 | 0.83 | |||||
Characteristics of the Brazilian Maternal Breastfeeding Evaluation Scale.
| Number of items | Score variation | Mean (SD) | Median | |
|---|---|---|---|---|
| Total score MBFES/BRASIL | 29 | 29–145 | 120.92±13.98 | 124 |
| Subscale: Pleasure and fulfillment of the maternal role | 12 | 12–60 | 53.36±6.96 | 56 |
| Subscale: Maternal physical, emotional and social aspects | 8 | 8–40 | 28.21±5.77 | 29 |
| Subscale: Child's growth, development and satisfaction | 9 | 9–45 | 39.35±4.99 | 40 |
SD, standard deviation.
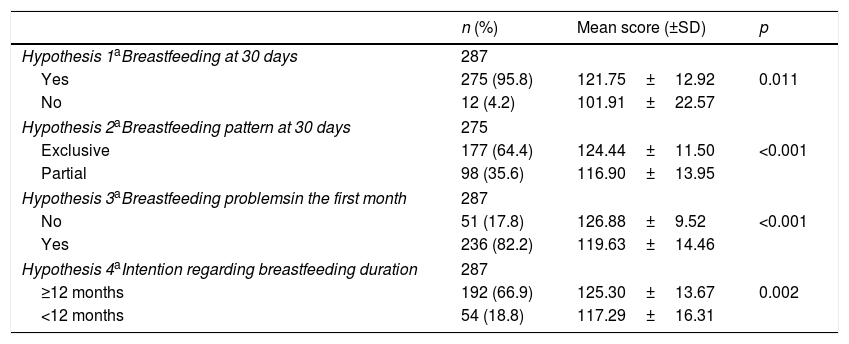
The results of the construct validity analysis showed that the hypotheses were confirmed: mothers who exclusively breastfed their infants in the first month, those who were breastfeeding in the first month, those who intended to breastfeed longer, and those who did not have problems with breastfeeding showed higher scores in the MBFES (Table 4).
Results of hypothesis testing for construct validity of the Brazilian Maternal Breastfeeding Evaluation Scale.
| n (%) | Mean score (±SD) | p | |
|---|---|---|---|
| Hypothesis 1aBreastfeeding at 30 days | 287 | ||
| Yes | 275 (95.8) | 121.75±12.92 | 0.011 |
| No | 12 (4.2) | 101.91±22.57 | |
| Hypothesis 2aBreastfeeding pattern at 30 days | 275 | ||
| Exclusive | 177 (64.4) | 124.44±11.50 | <0.001 |
| Partial | 98 (35.6) | 116.90±13.95 | |
| Hypothesis 3aBreastfeeding problemsin the first month | 287 | ||
| No | 51 (17.8) | 126.88±9.52 | <0.001 |
| Yes | 236 (82.2) | 119.63±14.46 | |
| Hypothesis 4aIntention regarding breastfeeding duration | 287 | ||
| ≥12 months | 192 (66.9) | 125.30±13.67 | 0.002 |
| <12 months | 54 (18.8) | 117.29±16.31 | |
SD, standard deviation.
The internal consistency of the MBFES was high, with a Cronbach's alpha of 0.88 (95% CI: 0.86–0.90). The subscales showed acceptable values: 0.92 (95% CI: 0.91–0.93) for the pleasure and fulfillment of the maternal role subscale; 0.70 (95% CI: 0.65–0.75) for maternal physical, emotional and social aspects; and 0.75 (95% CI: 0.70–0.79) for child growth, development, and satisfaction.
DiscussionThe psychometric tests for MBFES validation for the Brazilian population disclosed similar subscales when compared to the original ones. However, for the Brazilian version of the MBFES, it was necessary to eliminate an item from the validated scale in Portugal, resulting in 29 of the 30 original items. Question 27, “Breastfeeding made me feel like a cow,” was excluded because of the low factor load. This probably occurred because of feelings that were different from those expected by the original tool (negative ones) perceived by some Brazilian women in relation to the word “cow.” Some women did not interpret it as derogatory or offensive, as suggested by the authors,5 but as a word that qualified them as good producers of milk. This result corroborates the need for validation of the tool when applied in different countries, although these countries share the same language, but not the same culture.
Another change that occurred in the validation process of the MBFES for the Brazilian population was the reallocation of three items (15, 16, and 25) in the subscales. However, this change does not affect the total score.
In a validation study carried out in Japan, the original tool also underwent some changes regarding the number of items and in the subscales, by excluding seven items (3, 5, 13, 15, 19, 26, and 28 of the original version) and reconfiguring new combinations between the subscales, and the maternal satisfaction was the one that underwent fewer changes in both studies. Thus, the Japanese researchers also obtained three subscales: maternal satisfaction, potentially negative aspects, and perceived benefits for the baby,18 although two are quite different from the current study. The larger number of exclusions in the Japanese version probably occurred due to the use of a factor load (>0.5) greater than that used in the present study and by the tool creators (>0.4).5,18 The Portuguese validation study did not perform a factor analysis.7
When creating and validating the MBFES in the United States, the researchers found higher internal consistency values in the total scale (α=0.93 and α=0.94) and in the following domains: pleasure and fulfillment of the maternal role (α=0.93 and α=0.91), child satisfaction and growth (α=0.88 and α=0.83), and maternal lifestyle and body image (α=0.80 and α=0.84), respectively.5,12 In the Japanese validation study, the internal consistency of the total score was acceptable (α=0.91), as well as in the subscales (α=0.91, α=0.77 and α=0.84),18 being slightly higher than those found in the present study. In the Portuguese study, Galvão (2002)7 maintained the original items and Cronbach's alpha values were 0.92 in the total scale and 0.92, 0.76, and 0.76 in the subscales, similar to the values for the Brazilian population (0.88, and 0.92, 0.75, and 0.70). Moreover, in Portugal, the internal consistency variation for the total scale was also similar to that found in the present study (0.90 to 0.93 in the Portuguese study and 0.86 to 0.90 in the present study).20
In the same study, the Cronbach's alpha of the subscales varied from 0.87 to 0.92 (pleasure and fulfillment of the maternal role), from 0.76 to 0.82 (maternal lifestyle and body image), and from 0.70 to 0.76 (child satisfaction and growth), which are lower values than the ones observed in the US, but similar to the current one. Ramalho et al., also in Portugal, found slightly lower values (0.89 to 0.90, and 0.65 to 0.75, 0.66 to 0.74, and 0.88 to 0.90) to those observed in other Portuguese studies and in the present study.7,20,21
Finally, in the validation of the Spanish MBFES, which maintained the 30 items, Cronbach's alpha in the total scale was 0.92, similar to the other studies.22 It is noteworthy that although the Cronbach's alpha values in the present study are slightly lower than those of some validation studies in other countries, they are considered adequate, allowing their use in the Brazilian population.
An advantage of the current study was the fact that the tool was applied during home visits, resulting in a high return rate (100%), different from that observed in other studies that sent it through the mail, with a return rate of 72–86%.5,6,12
In the present study, the woman's satisfaction with breastfeeding was evaluated when the child was 1 month old. In the other validation studies, the children were 3–5 months old.7,12,18,22 However, the study that originated the tool does not mention the child's age when the tool was applied5 and it has been used at different moments of breastfeeding, from 2 weeks to 12 months after birth, suggesting that the tool can be used at different ages.6,8,13–15,17,21
The cultural aspects regarding breastfeeding are different in the two populations, including use of terms and expressions. Similar to what happened in some English-speaking countries, such as Australia,6,8,16 Canada,14,15 and Scotland,17 cross-cultural adaptation was not previously performed, which may have been a limitation of this study.
During the validation process of the tool for the Brazilian population, as it was the same language, it was decided to apply the questionnaire in the version translated in Portugal into the Portuguese language,7 with no changes in its structure, and clarify any doubts during the application. Few terms raised doubts, with explanations being added in parentheses to the final version of the Brazilian MBFES. It is important to emphasize that there is no standardization for cross-cultural adaptation when a tool is used in the same language that was applied in another country.30 Moreover, the tool was previously evaluated by breastfeeding experts, who felt that there was no need for modification.
According to the recommendation by Terwee et al.,24 given seven subjects for each item of the tool, the sample size of this study (287) was satisfactory. However, other authors, more recently,26 have suggested ten subjects for each item, which would require 300 participants. This deficit probably did not significantly influence the results because of its small magnitude.
In conclusion, this study verified that the Brazilian version of MBFES is a valid and reliable tool to be applied to the Brazilian population for the assessment of maternal satisfaction with breastfeeding. The validation and application of this tool will demonstrate the level of satisfaction of Brazilian women with breastfeeding, thus allowing health professionals to plan interventions that can increase this degree of satisfaction, consequently resulting in a more direct approach when promoting this practice. Furthermore, the availability of a validated tool for the Brazilian population increases the possibilities of studies, still inexistent, on the determinants of women's satisfaction with breastfeeding and its association with several outcomes, including the duration of this practice.
FundingThis work was funded by CNPq [Universal Notice 448186/2014-4] and CAPES research grants were given to the following authors: Andrea F. K. de Senna, Agnes M. B. L. Bizon, and Ana C. M. Martins. The funding sources did not participate in any stage of the research, preparation, and publication of the article.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank MBFES’ author Ellen Leff for her authorization to validate the tool for the Brazilian population. To Galvão and Graça for the Portuguese version. To all the mothers and babies who made this study possible, to Hospital das Clínicas de Porto Alegre and Hospital Moinhos de Vento for their support in the achievement of this research, to the other members of the team that participated in data collection, and to CAPES and CNPq for their funding of this study.
The following are the supplementary data to this article:
Please cite this article as: Senna AF, Giugliani C, Lago JC, Bizon AM, Martins AC, Oliveira CA, et al. Validation of a tool to evaluate women's satisfaction with maternal breastfeeding for the Brazilian population. J Pediatr (Rio J). 2020;96:84–91.
Study conducted at Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil.




