

To translate and culturally adapt the Pediatric Eosinophilic Esophagitis Symptom Score (version 2.0), a tool used to assess pediatric eosinophilic esophagitis symptoms reported by patients and/or their parents/caregivers.
MethodsThe Pediatric Eosinophilic Esophagitis Symptom Score was translated through the following stages: initial translation, back-translation, and consensus of independent reviewers through the Delphi technique. The pre-final version of the Pediatric Eosinophilic Esophagitis Symptom Score was applied to five 8-to-18-year-old patients and to ten parents of two-to-18-year-old patients from an outpatient pediatric gastroenterology service (pre-test).
ResultsDuring the translation process, no translations presenting with difficult consensus in the review process or grammar inconsistencies were observed. During the pre-test, difficulties in comprehension of some unconventional terms, e.g., “náusea”, were observed. Adverbs of frequency, such as “quase nunca” were also identified as being of difficult understanding by patients and parents, and the substitution by the term “raramente” was suggested. Such difficulties may be inherent to the pediatric age group. Age 8 years or above should be considered adequate for the self-reporting of symptoms.
ConclusionsThe study presents the Brazilian version of the Pediatric Eosinophilic Esophagitis Symptom Score, which is adapted to the Brazilian culture. This version may be introduced as a clinical and research tool for the assessment of patients with esophagic disease symptoms. The Pediatric Eosinophilic Esophagitis Symptom Score is a breakthrough in the evaluation of symptoms of pediatric eosinophilic esophagitis, since it reinforces the importance of self-reporting by patients who experience this disease.
Traduzir e adaptar culturalmente a Pediatric Eosinophilic Esophagitis Symptom Score (versão 2.0), um instrumento usado para identificar os sintomas relatados pelos pacientes ou seus pais/responsáveis para a avaliação da esofagite eosinofílica pediátrica.
MétodoRealizamos o processo de tradução a partir da tradução inicial, retrotradução, seguida da etapa de obtenção de consenso por revisores independentes por meio da técnica Delphi. Aplicamos a versão pré-final a cinco pacientes de 8 a 18 anos e dez pais de pacientes de 2 a 18 anos, no Serviço de Gastroenterologia Pediátrica (pré-teste).
ResultadosNo processo de tradução, não encontramos traduções de difícil consenso no processo de revisão ou discordâncias gramaticais. No pré-teste, identificamos dificuldades de entendimento de termos pouco convencionais, como “náusea”, com sugestão de substituição para o termo “enjoo”. Outra dificuldade encontrada relacionou-se aos advérbios de frequência da escala, como, por exemplo, “quase nunca”, sendo sugerida a substituição pelo termo “raramente”. Essas dificuldades podem ser inerentes à faixa etária pediátrica. A idade dos pacientes a partir de oito anos deve ser considerada adequada para o uso de escores de autorrelato.
ConclusõesA tradução do escore de sintomas da esofagite eosinofílica pediátrica produziu uma escala adaptada à cultura brasileira, que poderá ser introduzida como instrumento de investigação clínica e de pesquisa em pacientes com sintomas sugestivos de doenças esofágicas. É um importante avanço na avaliação dos sintomas, já que valoriza o relato dos próprios pacientes que convivem com essa doença.
Eosinophilic esophagitis (EoE) is a clinical and pathological entity mediated by immune and antigenic mechanisms that is an important cause of morbidity of the upper gastrointestinal tract, with a significant increase in its incidence and prevalence in the last decades.1,2 The disease is histologically defined by the predominance of an eosinophilic inflammatory process and clinically defined by symptoms of esophageal dysfunction.1,3,4 The symptoms are non-specific, especially in infants and preschool children, manifesting as nausea, vomiting, abdominal pain, growth deficit, and difficulty in introducing solid foods. Schoolchildren and adolescents may report dysphagia and food impaction in the esophagus, which are more specific and similar to symptoms in adults.2,5 The absence of specificity of EoE symptoms and its similarity to other age-specific pathological conditions, such as gastroesophageal reflux disease (GERD), are a diagnostic challenge for the general pediatrician or specialist. Adequate evaluation of these symptoms through valid and reliable tools becomes essential for diagnostic and therapeutic purposes.6
Tools that evaluate EoE severity have been developed for assisting in the diagnosis and treatment of the disease.7,8 However, few questionnaires consider the patient's own perception of the severity of their symptoms or response to treatment. Patient-reported outcomes (PRO) have been recognized as key measures for assessing the treatment of chronic diseases over the last decade. Although there are other published scales to evaluate the symptoms of EoE, only one validated tool that takes into account the symptoms reported by the patients or their parents/guardians for the assessment of pediatric EoE was retrieved in the literature, the Pediatric Eosinophilic Esophagitis Symptom Score (PEESS version 2.0).
PEESS v2.0™ was developed in the United States, based on focal and cognitive interviews, using the perceptions of patients and their parents, with the frequency and severity of EoE-related symptoms as the focus for the questions. Based on the responses and descriptions of patients with EoE and their relatives, as well as on the FDA guidelines, PEESS v2.0 was the first validated symptom score6,9 to be used by pediatric patients with symptoms of esophageal diseases and/or their parents.
In Brazil, there are no validated tools for the diagnosis of EoE based on the patients’ perception. In order to use the PEESS v2.0 in the Brazilian context, the translation and cultural adaptation, according to the methodological accuracy recommended in international guidelines, are paramount.10 The items should not only be translated into the linguistic form, but should also be culturally adapted to maintain the content validity of the tool for different cultures, on a conceptual basis, maintaining the equivalence between the original tool and the target version.10 This study aimed to translate and culturally adapt the PEESS v2.0 to obtain a Brazilian version with conceptual, semantic, and cultural equivalence to the original scale.
MethodsThis was a methodological study of translation and cultural adaptation, approved by the Research Ethics Committee of Universidade Federal de Uberlândia (UFU) (Protocol CEP/UFU 048050/2015).
After authorization to use the PEESS v2.0 by the Mapi Research Trust (http://mapigroup.com/tag/mapi-research-trust/), the authors performed the score translation into the Brazilian Portuguese language, using the translation and cultural adaptation methodologies, according to international translation standards for tools10,11 for linguistic validation, in seven stages (Fig. 1).

In the third stage of translation, the research coordinators compared the back-translation with the original scale, aiming to identify items with inappropriate translations or with greater difficulty of consensus during the translation and reconciliation stages. These items were selected for the independent reviewers’ process (fourth stage). The reviewers jointly analyzed the translations, the reconciliation, and the original version, using the modified Delphi technique,12–14 with the main purpose of evaluating the semantic, idiomatic, experimental, and conceptual equivalence between the original score and the back-translation. The modified Delphi technique (decision-making technique by means of electronic rounds) was based on the creation of a questionnaire consisting of all stages of the translation and the original scale and by qualitative and quantitative questions related to items requiring review.12
The questionnaire links were e-mailed to the reviewers, who were asked to answer the form within twenty days. Response data were immediately forwarded to the research coordinator by email, through a freely accessible website, and the respondents’ anonymity was maintained (http://armstrong.wharton.upenn.edu/delphi2/admin/reset_pw.php?ac=1rlaxC).
In the first round, reviewers chose the best translation (FW1 and FW2) and reconciliation (REC) options, or suggested another option, according to their knowledge. Each round was followed by the statistical representation of result distribution, by means of the percentage of agreement between the reviewers and the feedback of the group's responses for re-evaluation at the subsequent stage.15 The second stage consisted in the analysis of the first stage results, to identify convergence and change in the respondents’ decisions and opinions. The reviewers had free access to the statistical representation of the results distribution, in order to direct the group's consensus. The process was finished, according to the criteria previously established by the researchers, with a minimum consensus of 80% agreement between the reviewers.
After the score pre-final review stage, carried out by the language coordinator, the pre-final version was applied by the main investigator to 17 respondents after they signed the informed consent form. The pretest sample was defined according to the translation guidelines of the company responsible for the score copyright11: six patients between 8 and 18 years old, five parents of patients aged between 2 and 8 years old, and six parents of patients between 8 and 18 years, followed-up at the Pediatric Gastroenterology Outpatient Clinic of Uberlândia Federal University Hospital (UFU) for EoE diagnostic investigation or clinical follow-up. Illiterate parents or patients were excluded from the study. This stage aimed to identify and correct possible difficulties in understanding items and suggestions for improving the translation.
The qualitative analysis was performed by the main investigator through two brief oral interviews, the retrospective and cognitive interviews. During the retrospective interview, subjects were asked about the symptom score comprehension, the importance of the items, and on whether they had suggestions to improve the score comprehension.
The cognitive interview aimed to identify whether the meaning of each item given by the score's author was understood in the same manner by the interviewee. The subjects identified translation problems and gave translation suggestions for each item. The observations of patients and their parents were considered to determine the cultural adaptation of the translated version. Items reported as difficult to understand, as well as the suggestions made by patients and their parents, were incorporated into a new reading test by the language reviewer. After the final grammatical review, the version was sent for final approval by the company that holds the copyright of the score.
QuestionnairesSociodemographic questionnaireData such as age, gender, and level of schooling of the patients and their parents who participated in the pre-test were collected through an oral interview, before the cognitive and retrospective interviews.
PEESS v2.0PEESS is a score that assesses the frequency and intensity of EoE-related symptoms. It consists of twenty items, eleven of which are related to the frequency and nine, to the intensity of the symptoms. The answers to each item are distributed on a scale with scores ranging from 0 to 4. In items referring to frequency, 0 corresponds to “never” and 4 corresponds to “almost always” (two or more times a day). In items referring to intensity, 0 corresponds to “not bad” and 4 corresponds to “very bad”. The scores are transformed into a scale from zero to 100, as follows: 0=0; 1=25; 2=50; 3=75; and 4=100. The higher the score, the greater the severity and frequency of symptoms. There are two self-administered scores, one for patients aged 8 to 18 and another for parents or guardians of children aged 2 to 18 years.6,16
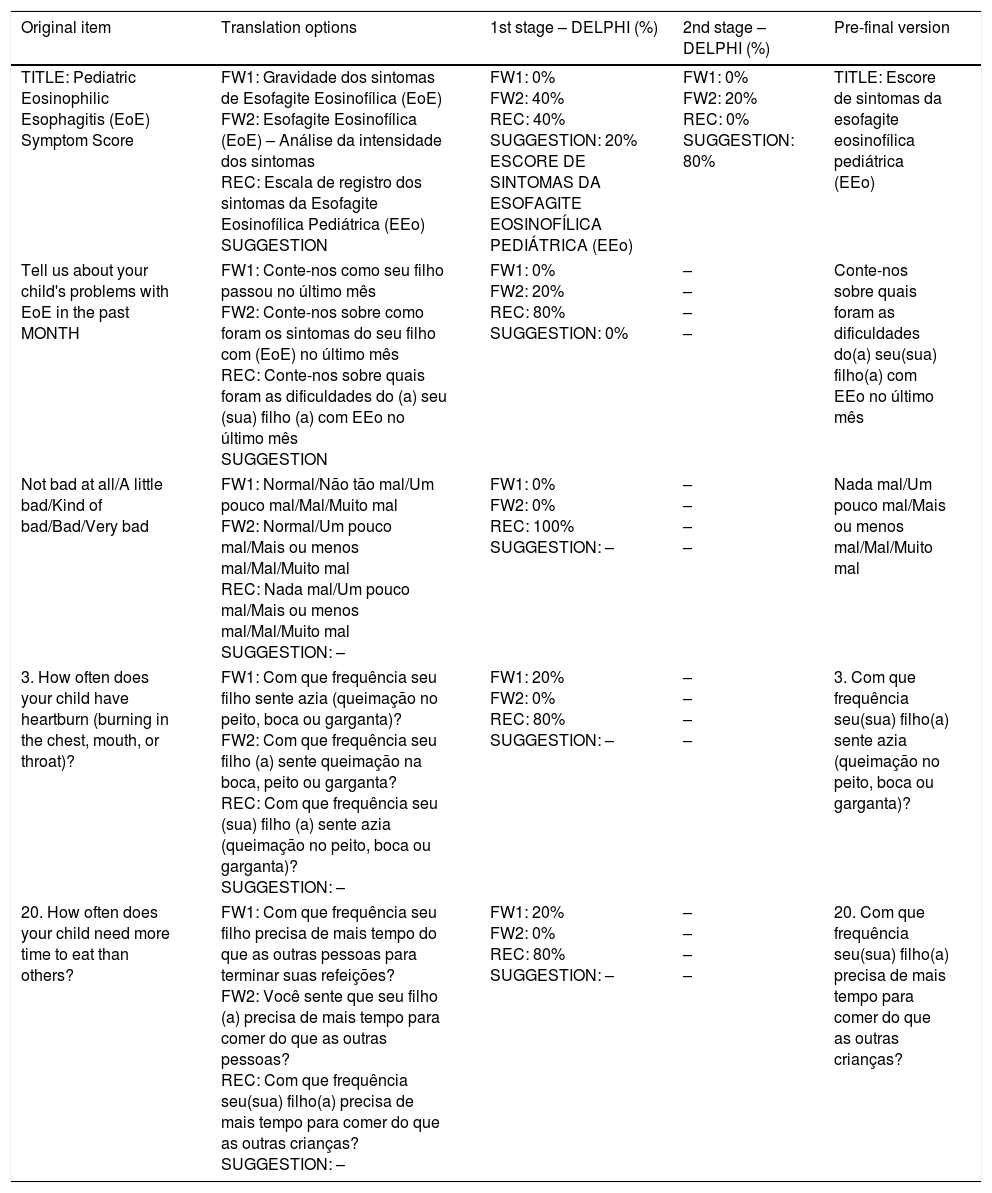
ResultsAfter the initial translation, reconciliation, and back-translation process, the title, score guidelines, severity response categories, and two items (items 3 and 20) were submitted to review and consensus-building using the Delphi technique. Only the score title was sent to a second round, when it reached 80% agreement among reviewers. The reviewers chose the reconciled version in the score guidelines, severity response categories, and in items 3 and 20 (80%; Table 1).
Score items for parents of children aged two to eighteen years sent to independent reviewers for consensus-building using the DELPHI technique.12
| Original item | Translation options | 1st stage – DELPHI (%) | 2nd stage – DELPHI (%) | Pre-final version |
|---|---|---|---|---|
| TITLE: Pediatric Eosinophilic Esophagitis (EoE) Symptom Score | FW1: Gravidade dos sintomas de Esofagite Eosinofílica (EoE) FW2: Esofagite Eosinofílica (EoE) – Análise da intensidade dos sintomas REC: Escala de registro dos sintomas da Esofagite Eosinofílica Pediátrica (EEo) SUGGESTION | FW1: 0% FW2: 40% REC: 40% SUGGESTION: 20% ESCORE DE SINTOMAS DA ESOFAGITE EOSINOFÍLICA PEDIÁTRICA (EEo) | FW1: 0% FW2: 20% REC: 0% SUGGESTION: 80% | TITLE: Escore de sintomas da esofagite eosinofílica pediátrica (EEo) |
| Tell us about your child's problems with EoE in the past MONTH | FW1: Conte-nos como seu filho passou no último mês FW2: Conte-nos sobre como foram os sintomas do seu filho com (EoE) no último mês REC: Conte-nos sobre quais foram as dificuldades do (a) seu (sua) filho (a) com EEo no último mês SUGGESTION | FW1: 0% FW2: 20% REC: 80% SUGGESTION: 0% | – – – – | Conte-nos sobre quais foram as dificuldades do(a) seu(sua) filho(a) com EEo no último mês |
| Not bad at all/A little bad/Kind of bad/Bad/Very bad | FW1: Normal/Não tão mal/Um pouco mal/Mal/Muito mal FW2: Normal/Um pouco mal/Mais ou menos mal/Mal/Muito mal REC: Nada mal/Um pouco mal/Mais ou menos mal/Mal/Muito mal SUGGESTION: – | FW1: 0% FW2: 0% REC: 100% SUGGESTION: – | – – – – | Nada mal/Um pouco mal/Mais ou menos mal/Mal/Muito mal |
| 3. How often does your child have heartburn (burning in the chest, mouth, or throat)? | FW1: Com que frequência seu filho sente azia (queimação no peito, boca ou garganta)? FW2: Com que frequência seu filho (a) sente queimação na boca, peito ou garganta? REC: Com que frequência seu (sua) filho (a) sente azia (queimação no peito, boca ou garganta)? SUGGESTION: – | FW1: 20% FW2: 0% REC: 80% SUGGESTION: – | – – – – | 3. Com que frequência seu(sua) filho(a) sente azia (queimação no peito, boca ou garganta)? |
| 20. How often does your child need more time to eat than others? | FW1: Com que frequência seu filho precisa de mais tempo do que as outras pessoas para terminar suas refeições? FW2: Você sente que seu filho (a) precisa de mais tempo para comer do que as outras pessoas? REC: Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras crianças? SUGGESTION: – | FW1: 20% FW2: 0% REC: 80% SUGGESTION: – | – – – – | 20. Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras crianças? |
FW1, translator 1; FW2, translator 2; REC, reconciliation.
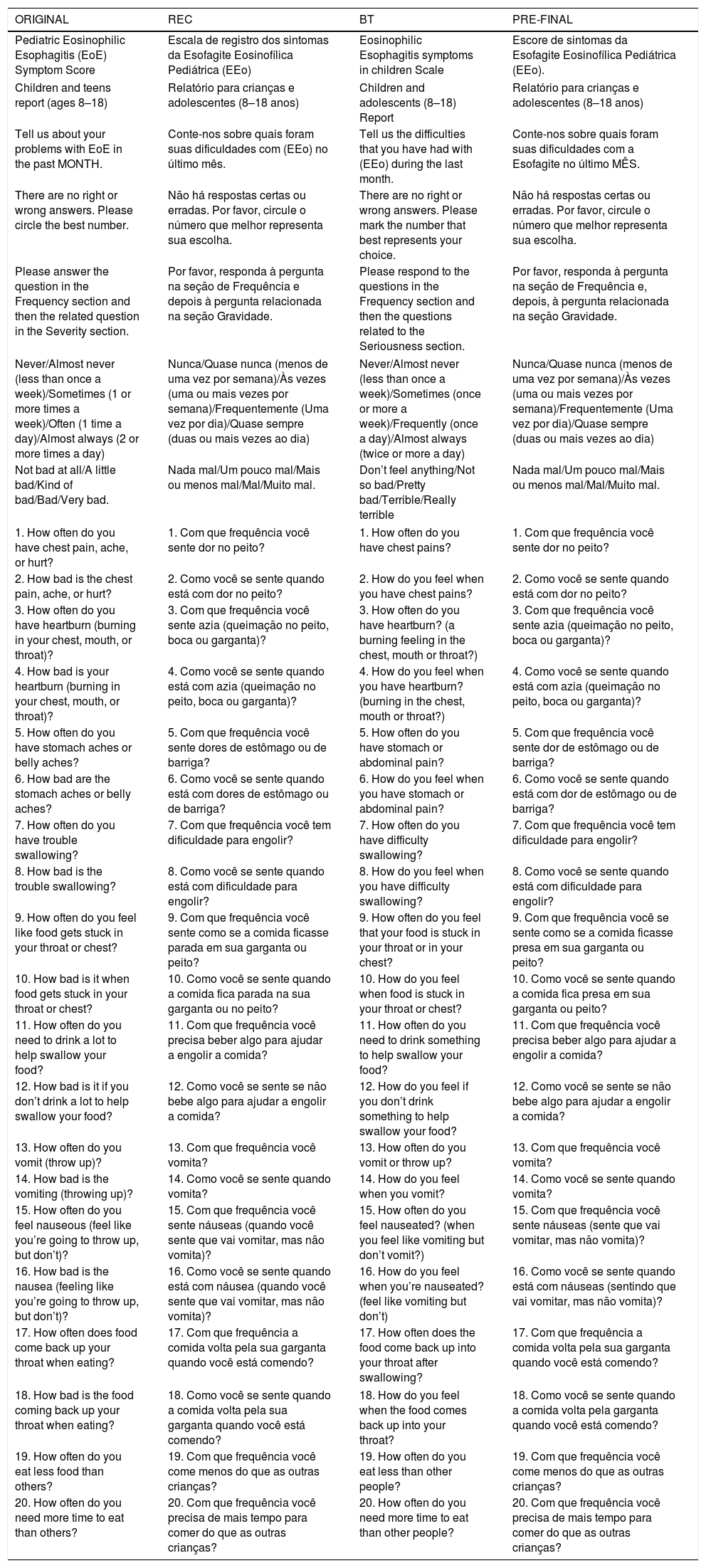
After completing the review stage, the score was submitted for grammatical review. At this stage, items 5 and 6 were corrected in the translation of “stomach aches or belly aches”, initially as “dores de estômago ou de barriga” in the reconciliation, to “dor de estômago ou de barriga” in the corrected version (Table 2).
Translation process (translation, reconciliation, and back-translation) of the score for patients aged 8–18 years.a
| ORIGINAL | REC | BT | PRE-FINAL |
|---|---|---|---|
| Pediatric Eosinophilic Esophagitis (EoE) Symptom Score | Escala de registro dos sintomas da Esofagite Eosinofílica Pediátrica (EEo) | Eosinophilic Esophagitis symptoms in children Scale | Escore de sintomas da Esofagite Eosinofílica Pediátrica (EEo). |
| Children and teens report (ages 8–18) | Relatório para crianças e adolescentes (8–18 anos) | Children and adolescents (8–18) Report | Relatório para crianças e adolescentes (8–18 anos) |
| Tell us about your problems with EoE in the past MONTH. | Conte-nos sobre quais foram suas dificuldades com (EEo) no último mês. | Tell us the difficulties that you have had with (EEo) during the last month. | Conte-nos sobre quais foram suas dificuldades com a Esofagite no último MÊS. |
| There are no right or wrong answers. Please circle the best number. | Não há respostas certas ou erradas. Por favor, circule o número que melhor representa sua escolha. | There are no right or wrong answers. Please mark the number that best represents your choice. | Não há respostas certas ou erradas. Por favor, circule o número que melhor representa sua escolha. |
| Please answer the question in the Frequency section and then the related question in the Severity section. | Por favor, responda à pergunta na seção de Frequência e depois à pergunta relacionada na seção Gravidade. | Please respond to the questions in the Frequency section and then the questions related to the Seriousness section. | Por favor, responda à pergunta na seção de Frequência e, depois, à pergunta relacionada na seção Gravidade. |
| Never/Almost never (less than once a week)/Sometimes (1 or more times a week)/Often (1 time a day)/Almost always (2 or more times a day) | Nunca/Quase nunca (menos de uma vez por semana)/Às vezes (uma ou mais vezes por semana)/Frequentemente (Uma vez por dia)/Quase sempre (duas ou mais vezes ao dia) | Never/Almost never (less than once a week)/Sometimes (once or more a week)/Frequently (once a day)/Almost always (twice or more a day) | Nunca/Quase nunca (menos de uma vez por semana)/Às vezes (uma ou mais vezes por semana)/Frequentemente (Uma vez por dia)/Quase sempre (duas ou mais vezes ao dia) |
| Not bad at all/A little bad/Kind of bad/Bad/Very bad. | Nada mal/Um pouco mal/Mais ou menos mal/Mal/Muito mal. | Don’t feel anything/Not so bad/Pretty bad/Terrible/Really terrible | Nada mal/Um pouco mal/Mais ou menos mal/Mal/Muito mal. |
| 1. How often do you have chest pain, ache, or hurt? | 1. Com que frequência você sente dor no peito? | 1. How often do you have chest pains? | 1. Com que frequência você sente dor no peito? |
| 2. How bad is the chest pain, ache, or hurt? | 2. Como você se sente quando está com dor no peito? | 2. How do you feel when you have chest pains? | 2. Como você se sente quando está com dor no peito? |
| 3. How often do you have heartburn (burning in your chest, mouth, or throat)? | 3. Com que frequência você sente azia (queimação no peito, boca ou garganta)? | 3. How often do you have heartburn? (a burning feeling in the chest, mouth or throat?) | 3. Com que frequência você sente azia (queimação no peito, boca ou garganta)? |
| 4. How bad is your heartburn (burning in your chest, mouth, or throat)? | 4. Como você se sente quando está com azia (queimação no peito, boca ou garganta)? | 4. How do you feel when you have heartburn? (burning in the chest, mouth or throat?) | 4. Como você se sente quando está com azia (queimação no peito, boca ou garganta)? |
| 5. How often do you have stomach aches or belly aches? | 5. Com que frequência você sente dores de estômago ou de barriga? | 5. How often do you have stomach or abdominal pain? | 5. Com que frequência você sente dor de estômago ou de barriga? |
| 6. How bad are the stomach aches or belly aches? | 6. Como você se sente quando está com dores de estômago ou de barriga? | 6. How do you feel when you have stomach or abdominal pain? | 6. Como você se sente quando está com dor de estômago ou de barriga? |
| 7. How often do you have trouble swallowing? | 7. Com que frequência você tem dificuldade para engolir? | 7. How often do you have difficulty swallowing? | 7. Com que frequência você tem dificuldade para engolir? |
| 8. How bad is the trouble swallowing? | 8. Como você se sente quando está com dificuldade para engolir? | 8. How do you feel when you have difficulty swallowing? | 8. Como você se sente quando está com dificuldade para engolir? |
| 9. How often do you feel like food gets stuck in your throat or chest? | 9. Com que frequência você sente como se a comida ficasse parada em sua garganta ou peito? | 9. How often do you feel that your food is stuck in your throat or in your chest? | 9. Com que frequência você se sente como se a comida ficasse presa em sua garganta ou peito? |
| 10. How bad is it when food gets stuck in your throat or chest? | 10. Como você se sente quando a comida fica parada na sua garganta ou no peito? | 10. How do you feel when food is stuck in your throat or chest? | 10. Como você se sente quando a comida fica presa em sua garganta ou peito? |
| 11. How often do you need to drink a lot to help swallow your food? | 11. Com que frequência você precisa beber algo para ajudar a engolir a comida? | 11. How often do you need to drink something to help swallow your food? | 11. Com que frequência você precisa beber algo para ajudar a engolir a comida? |
| 12. How bad is it if you don’t drink a lot to help swallow your food? | 12. Como você se sente se não bebe algo para ajudar a engolir a comida? | 12. How do you feel if you don’t drink something to help swallow your food? | 12. Como você se sente se não bebe algo para ajudar a engolir a comida? |
| 13. How often do you vomit (throw up)? | 13. Com que frequência você vomita? | 13. How often do you vomit or throw up? | 13. Com que frequência você vomita? |
| 14. How bad is the vomiting (throwing up)? | 14. Como você se sente quando vomita? | 14. How do you feel when you vomit? | 14. Como você se sente quando vomita? |
| 15. How often do you feel nauseous (feel like you’re going to throw up, but don’t)? | 15. Com que frequência você sente náuseas (quando você sente que vai vomitar, mas não vomita)? | 15. How often do you feel nauseated? (when you feel like vomiting but don’t vomit?) | 15. Com que frequência você sente náuseas (sente que vai vomitar, mas não vomita)? |
| 16. How bad is the nausea (feeling like you’re going to throw up, but don’t)? | 16. Como você se sente quando está com náusea (quando você sente que vai vomitar, mas não vomita)? | 16. How do you feel when you’re nauseated? (feel like vomiting but don’t) | 16. Como você se sente quando está com náuseas (sentindo que vai vomitar, mas não vomita)? |
| 17. How often does food come back up your throat when eating? | 17. Com que frequência a comida volta pela sua garganta quando você está comendo? | 17. How often does the food come back up into your throat after swallowing? | 17. Com que frequência a comida volta pela sua garganta quando você está comendo? |
| 18. How bad is the food coming back up your throat when eating? | 18. Como você se sente quando a comida volta pela sua garganta quando você está comendo? | 18. How do you feel when the food comes back up into your throat? | 18. Como você se sente quando a comida volta pela garganta quando você está comendo? |
| 19. How often do you eat less food than others? | 19. Com que frequência você come menos do que as outras crianças? | 19. How often do you eat less than other people? | 19. Com que frequência você come menos do que as outras crianças? |
| 20. How often do you need more time to eat than others? | 20. Com que frequência você precisa de mais tempo para comer do que as outras crianças? | 20. How often do you need more time to eat than other people? | 20. Com que frequência você precisa de mais tempo para comer do que as outras crianças? |
One father and one 15-year-old male patient were excluded from the study due to lack of schooling. Thus, the pre-test sample consisted of 15 respondents. The age of the parents or guardians ranged from 28 to 48 years, with 30% males and 70% females. The level of schooling ranged from elementary school to full college/university. Patient age ranged from 10 to 17 years, with 20% females and 80% males, and the level of schooling ranging from elementary to high school. The lack of patients aged 8 to 10 years was considered a limitation.
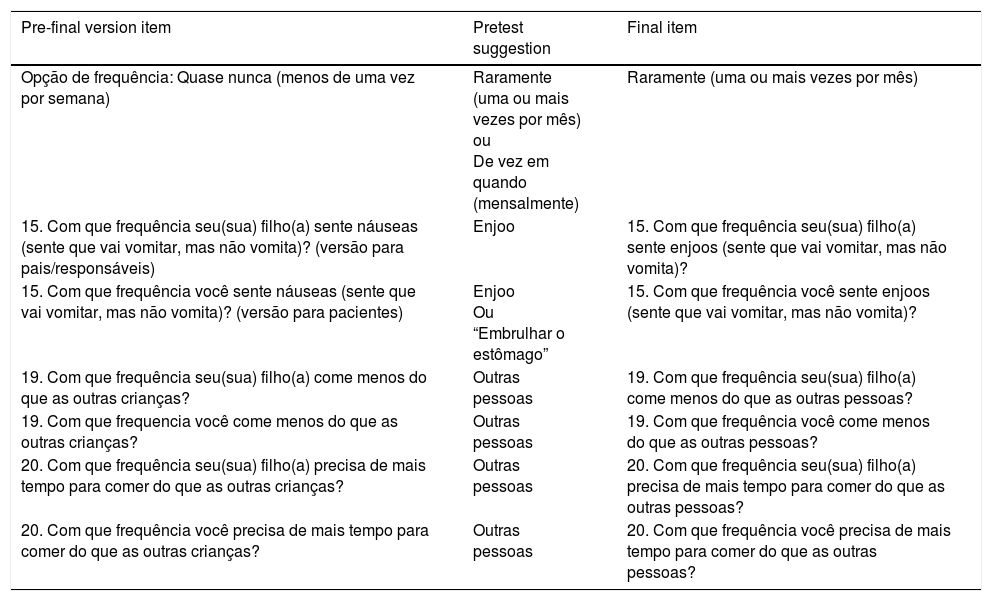
In the retrospective interview, all respondents reported having understood the symptom score, considering its application important. Among the suggestions, five parents of patients aged 2–18 years and two patients aged 8 to 18 years suggested that in the frequency response categories, the option “Quase nunca (menos de uma vez por semana)”, translated from “Almost never (less than once a week)” in the reconciliation stage, should be modified to options such as “Raramente (uma ou mais vezes por mês)” or “De vez em quando (mensalmente)”. Such modification was suggested because of the difficulty to understand the frequency between the categories “Nunca” and “Às vezes (uma ou mais vezes por semana)”. According to the opinion of the language reviewer, the option “Raramente” would be more appropriate for the frequency between “Nunca” and “Às vezes” (Table 3).
Items from the pre-final version, pre-test suggestions, and final version of the score for parents/guardians of patients aged 2–18 years and patients aged 8–18 years.a
| Pre-final version item | Pretest suggestion | Final item |
|---|---|---|
| Opção de frequência: Quase nunca (menos de uma vez por semana) | Raramente (uma ou mais vezes por mês) ou De vez em quando (mensalmente) | Raramente (uma ou mais vezes por mês) |
| 15. Com que frequência seu(sua) filho(a) sente náuseas (sente que vai vomitar, mas não vomita)? (versão para pais/responsáveis) | Enjoo | 15. Com que frequência seu(sua) filho(a) sente enjoos (sente que vai vomitar, mas não vomita)? |
| 15. Com que frequência você sente náuseas (sente que vai vomitar, mas não vomita)? (versão para pacientes) | Enjoo Ou “Embrulhar o estômago” | 15. Com que frequência você sente enjoos (sente que vai vomitar, mas não vomita)? |
| 19. Com que frequência seu(sua) filho(a) come menos do que as outras crianças? | Outras pessoas | 19. Com que frequência seu(sua) filho(a) come menos do que as outras pessoas? |
| 19. Com que frequencia você come menos do que as outras crianças? | Outras pessoas | 19. Com que frequência você come menos do que as outras pessoas? |
| 20. Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras crianças? | Outras pessoas | 20. Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras pessoas? |
| 20. Com que frequência você precisa de mais tempo para comer do que as outras crianças? | Outras pessoas | 20. Com que frequência você precisa de mais tempo para comer do que as outras pessoas? |
In the cognitive interview, the respondents showed comprehension difficulties and suggested changes in five items; however, in only three items (15, 19 and 20), the language and research coordinators considered relevant the comprehension difficulties and suggestions given by the respondents, meeting the criteria for modification (Table 3). Suggestions were made to replace the term “náusea” by “enjoo” or even by the idiomatic expression “embrulhar o estômago”, making the item easier to understand. The coordinators chose the first suggestion, “enjoo”, with no grammatical disagreement, defining the item in the final version as “Com que frequência seu(sua) filho(a) sente enjoos (sente que vai vomitar, mas não vomita)?”
Also during the cognitive interview, two parents and one patient suggested replacing the term “outras crianças” by the term “outras pessoas” in items 19 and 20 (“Com que frequência seu(sua) filho(a) come menos do que as outras crianças?” and “Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras crianças?”). The authors considered that the suggestion would improve the understanding of these items and, therefore, the final translation version consisted of “Com que frequência seu(sua) filho(a) come menos do que as outras pessoas?” and “Com que frequência seu(sua) filho(a) precisa de mais tempo para comer do que as outras pessoas?” (Table 3).
DiscussionThis study translated and culturally adapted the Brazilian version of the PEESS v2.0 for evaluation of EoE symptoms in children and adolescents.
The pediatric patient's symptom perception and the parents’ reports are extremely important to evaluate the current therapeutic options for the EoE and the disease evolution.6 Currently, it is known that the histological severity of EoE inflammation, measured by the eosinophil count in the tissue and the presence and intensity of endoscopic signs, may not be directly related to the severity of the symptoms experienced by the patients.17,18 Therefore, the introduction of the PEESS v2.0 as a symptom score reported by parents and/or patients with suspected and diagnosed EoE may represent an important advance in the investigation and research of this disease. In fact, previous results have demonstrated the usefulness of the score in clinical practice as an objective measure of patients’ symptoms and assessment of treatment response.18
During the translation process, no translations of difficult consensus or grammatical disagreements were observed. At the independent reviewers’ stage, the Delphi technique was applied until the second stage to attain consensus related to the score title. This technique provided greater authenticity to the translation process and can be considered a support tool in decision-making, as it allowed the participation of a group of specialists in translation and in pediatric gastroenterology.15
At the grammar review stage, the only suggested adjustment was the translation of “stomach aches or belly aches”, an expression originally translated as “dores de estômago ou de barriga”, into the singular form “dor de estômago ou de barriga”. When considering the syntactic conventionality in translation, the word “dor” in Portuguese has a broad and generalized meaning,19 with its frequency of occurrence being given in the plural form. Moreover, the singular form, considered conventional, that is, “of use or practice, consolidated by use or practice,”20 should be preferred in scales to be used with the population. Syntactic conventionality was also the justification for replacing the word “náusea” by “enjoo,”19 suggested by patients and their parents after the cognitive interview. These words are considered synonymous, but the word “enjoo” was popularly considered to be more easily understood.
Another suggestion provided in the pre-test stage was the replacement of “quase nunca (menos que uma vez por semana)”, the translation of “almost never (less than once a week)”, by the synonymous adverb “raramente (uma ou mais vezes por mês)”. Both are indicators of frequency; however, the suggestion made by patients and parents in the cognitive interview was referred to as more easily understood. These findings indicate the importance of incorporating the respondents’ suggestions into the processes of cultural adaptation of tools and indicate the need for psychometric evaluation of the items in subsequent studies. Also, during the cognitive interview, it was observed that patients aged 10–17 years understood well the frequency indicators used in the score response categories, a fact consistent with previous results.21 The easy comprehension among patients in this age group shows that older children have a good understanding of frequency adverbs and a more developed declarative memory than children under 8 years of age.22 This evidence reinforces the possibility of using self-report scores in children aged 8 years and older.
The group aged 8 years and older was considered a determinant factor for a better understanding of the score items, especially when considering the patients’ reading and comprehension skills; however, it was not possible to apply the pre-test to patients aged between 8 and 10 years, and this fact constitutes a limitation of this study. Children over 8 years of age are able to discuss and express their experiences of illness.23 The methodology care to use specific scales, appropriate to the age group and according to variations in the cognitive development of the respondents, is an important criterion for the score use in both clinical research and practice.24
As for the item “Com que frequência você precisa de mais tempo para comer do que as outras crianças?”, the children understood the meaning of the item, but could not relate to it personally. This was probably due to the fact that they did not have the experience of living in a family environment with other children of the same age, as it is known that eating behavior may vary according to the age group.25 Another possible explanation for these results may be the age of the respondents, who, between the ages of 10 and 17, do not appear to consider themselves as “children”. Other studies also reported similar difficulties in children and adolescents.23,24 Previous experience related to the symptoms or behaviors measured by the item is an important aspect to be considered in later validation processes of the score. The authors consider these comprehension difficulties to be inherent to the age group.
Another difficulty that is inherent to the pediatric age group emerged during the cognitive interview with parents and guardians. The parents reported having some difficulty answering some items. That occurred because they did not know such information about their children or because they failed to observe the child enough to develop a conclusion about the item. This fact was observed mainly in parents of young children, under 5 years old, who have difficulty to express more subjective symptoms such as “heartburn” and “nausea”. Although it is known that the use of reporting by parents or guardians in children is highly reliable and valid,26 the authors call attention to the interpretation of items related to more subjective symptoms, which are more difficult to be expressed by children under 8 years of age.23,24
The translation of the PEESS resulted in a scale adapted to the Brazilian culture, which could be introduced as a tool for clinical investigation and symptom screening in patients with a suspected diagnosis of EoE (Supplementary materials 1 and 2). Subsequent score validation studies should elucidate the psychometric parameters of the items, especially those with greater comprehension difficulty by children, adolescents, and parents/guardians in the pre-test. PEESS is an important advance in the evaluation of EoE symptoms, as it values the report of the patients that live with this disease, in the scenario of a chronic disease, with an invasive diagnosis and follow-up, which requires careful evaluation of symptom evolution for appropriate therapeutic planning.
The translation of the PEESS resulted in a scale adapted to the Brazilian culture, which could be introduced as a tool for clinical investigation and symptom screening in patients with a suspected diagnosis of EoE (Supplementary materials 1 and 2). Subsequent score validation studies should elucidate the psychometric parameters of the items, especially those with greater comprehension difficulty by children, adolescents, and parents/guardians in the pre-test. PEESS is an important advance in the evaluation of EoE symptoms, as it values the report of the patients that live with this disease, in the scenario of a chronic disease, with an invasive diagnosis and follow-up, which requires careful evaluation of symptom evolution for appropriate therapeutic planning.
Conflicts of interestThe authors declare no conflicts of interest.
The following are the supplementary data to this article:
Please cite this article as: Santos MF, Barros CP, Silva CH, Paro HB. Translation and cultural adaptation of the Pediatric Eosinophilic Esophagitis Symptom Score (PEESS v2.0). J Pediatr (Rio J). 2018;94:642–51.




