


Secretory phospholipase A2 (sPLA2) enzyme activity is a potential inflammatory biomarker for cardiovascular disease. We examined the tracking, or persistence, of sPLA2 enzyme activity levels from childhood to adulthood, and identify potentially modifiable factors affecting tracking.
MethodProspective cohort of 1735 children (45% females) who had serum sPLA2 enzyme activity levels and other cardiovascular disease risk factors measured in 1980 that were followed-up in 2001.
ResultssPLA2 activity tracked from childhood to adulthood for males (r=0.39) and females (r=0.45). Those who decreased body mass index relative to their peers were more likely to resolve elevated childhood sPLA2 levels than have persistent elevated sPLA2 levels in childhood and adulthood. Those who consumed less fruit, and gained more body mass index relative to their peers, began smoking or were a persistent smoker between childhood and adulthood were more likely to develop incident elevated sPLA2 levels than those with persistent not elevated sPLA2 levels.
ConclusionsChildhood sPLA2 enzyme activity levels associate with adult sPLA2 levels 21 years later. Healthful changes in modifiable risk factors that occur between childhood and adulthood might prevent children from developing elevated sPLA2 levels in adulthood.
A atividade da enzima fosfolipase A2 secretória (sPLA2) é um possível biomarcador inflamatório de doença cardiovascular. Examinamos o monitoramento, ou a persistência, dos níveis de atividade da enzima sPLA2 da infância à vida adulta e identificamos fatores possivelmente modificáveis que afetam o monitoramento.
MétodoCoorte prospectiva de 1.735 crianças (45% do sexo feminino) cujos níveis de atividade da enzima sPLA2 no soro e outros fatores de risco para doença cardiovascular foram medidos em 1980 e acompanhados até 2011.
ResultadosAtividade da enzima sPLA2 monitorada da infância à vida adulta para indivíduos do sexo masculino (r = 0,39) e sexo feminino (r = 0,45). Aqueles que diminuíram seus índices de massa corporal com relação a seus pares foram mais propensos à redução dos níveis elevados de sPLA2 na infância do que a manter níveis persistentemente elevados de sPLA2 na infância e vida adulta. Aqueles que consumiram menos frutas e ganharam mais índice de massa corporal com relação a seus pares, que começaram a fumar ou foram fumantes persistentes entre a infância e vida adulta foram mais propensos a desenvolver níveis de sPLA2 elevados do que aqueles com níveis de sPLA2 não elevados persistentes.
ConclusõesOs níveis de atividade da enzima sPLA2 na infância estão associados aos níveis de sPLA2 na vida adulta, 21 anos mais tarde. As mudanças saudáveis nos fatores de risco modificáveis que ocorrem entre a infância e a vida adulta podem evitar que as crianças desenvolvam níveis elevados de sPLA2 na vida adulta.
Inflammatory biomarkers have been observed in all stages of atherosclerosis development.1 Research into secretory phospholipase A2 (sPLA2) enzyme activity has gained interest over other inflammatory biomarkers owing to its increased specificity to the vasculature.2
sPLA2 belongs to a superfamily of enzymes known as the phospholipase A2s. These enzymes are responsible for catalysing the hydrolysis of fatty acid from the sn-2 position of membrane phospholipids, the release of polyunsaturated fatty acids, and host defence against bacterial infection.3 Release of sPLA2 promotes production of many eicosanoids and bioactive lipid mediators.4 The effect of sPLA2 on lipoproteins releases several lipid mediators at the place of lipoprotein retention within the wall of the artery, triggering local inflammatory cellular responses.5 sPLA2 also has direct action on low-density lipoprotein (LDL) particles, inducing them to have a more atherogenic effect.5 These sPLA2-induced changes are thought to contribute to atherosclerosis development,6,7 sparking interest as a potential target for intervention. Although early phase clinical trials have supported the efficacy of sPLA2 inhibition using pharmacological intervention,8–10 the only phase III trial conducted revealed contrary results,11 and results from Mendelian randomisation studies have been equivocal of a causal role for sPLA2 enzyme activity in cardiovascular disease (CVD) outcomes.12,13
Vessel changes favouring atherosclerosis begin in childhood14 and traditional CVD risk factors (lipoproteins, blood pressure, adiposity) track, or persist, from childhood to adulthood.15 However, no studies have examined if sPLA2 enzyme activity levels track from childhood to adulthood. Using data from the 21-year follow up of the Cardiovascular Risk in Young Finns Study, we examined if sPLA2 enzyme activity levels track from childhood to adulthood, and the potentially modifiable lifestyle-related factors that affect tracking over this period.
MethodsStudy populationThe Cardiovascular Risk in Young Finns Study is a population-based prospective follow-up on 3596 Finnish children and adolescents aged 3–18 years who participated at baseline in 1980. In 2001, 2283 of the baseline participants attended clinics, aged 24–39 years. Measurements of serum sPLA2 were performed on those with available samples from both 1980 and 2001 (n=2245). We excluded participants who had a condition that may predispose them to altered sPLA2 levels: participants with chronic rheumatic disease (n=34; sPLA2 activity 1.80 (1.29–2.22)nmol/min/mL in 2001); females who reported they were pregnant (n=59; sPLA2 activity 1.67 (1.33–2.08)nmol/min/mL in 2001); participants who reported having an infection with fever in the last 2 weeks (n=104; sPLA2 activity 1.65 (1.32–2.08)nmol/min/mL in 2001); females who reported current use of oral contraceptives (n=288; sPLA2 activity 1.78 (1.39–2.28)nmol/min/mL in 2001; n=25; sPLA2 activity 0.52 (0.41–0.97)nmol/min/mL in 1980). After exclusions, data on 1735 participants were left for our primary analyses. The study was conducted according to the Declaration of Helsinki, and local ethics committees approved the study protocols. Written informed consent was obtained from all participants in 2001, and their parents in 1980.
Clinical measurements and risk factorsAt both time-points, height was measured with a Seca anthropometer and weight was measured with Seca scales (Vogel Halke, Hamburg, Germany). Body mass index (BMI, kg/m2) was calculated. Self-report questionnaires administered at baseline and follow-up collected data on smoking, dietary habits, and physical activity.16 Information on smoking habits was only collected amongst participants aged 12–18 years at baseline. Participants who smoked at least weekly at baseline or daily at follow-up were considered smokers. Fruit and vegetable consumption was reported based on six options (1=daily, 2=almost every day, 3=a couple of times per week, 4=about once a week, 5=a couple of times per month, 6=less than a couple of times per month), which was converted into times of consumption per week (1, >9.5; 2, >6.3; 3, >3; 4, >1.2; 5, >0.3; 6, >0.1).17 Physical activity index (range from 5 (low) to 15 (high)), was determined by participant's self-report of duration, intensity, and frequency of physical activity.18 Socioeconomic position (SEP) was based on highest level of parental occupation at baseline (manual, lower-grade non-manual, higher-grade non-manual) and participant occupation at follow-up.19
Serum sPLA2 enzyme activity measurementsIn 1980 and 2001, blood samples were taken from the antecubital vein after participants confirmed they had fasted overnight. Serum sPLA2 enzyme activity was measured in 2006 from 1980 blood samples stored at −20°C, and 2001 samples stored at −80°C.20 Measurement of sPLA2 enzyme activity includes several groups of sPLA2 (IIA, V, X)21 expressed in atherosclerotic lesions from human and animal models.22 Hydrolysis of substrate without plasma was used as the negative control and deduced from sPLA2 activity. Samples were tested in duplicate. Intra- and inter-assay coefficients of variation were <10% and the minimum detectable level of sPLA2 activity was 0.10nmol/min/mL.
Statistical analysesAll analyses were performed using STATA 13.1 (StataCorp, College Station, TX, USA).
DemographicsBaseline and follow-up characteristics are displayed for male and female participants. Continuous variables are displayed as mean (standard deviation) for normally distributed variables and median (25–75th percentiles) for variables with a non-normal distribution. Categorical variables are displayed as N (percent). We also plot age on mean sPLA2 enzyme activity levels by sex.
Tracking of sPLA2 levels from childhood to adulthoodTracking was estimated by two approaches used in previous tracking studies23,24: (1) rank correlations by applying Pearson's correlation to the rank of baseline and follow-up sPLA2 measurements; and (2) the proportion of participants remaining in the upper quarter of age- and sex-specific sPLA2 distributions at both time-points. We report partial correlations adjusted for age when ages are combined, or adjusted age and sex when data for age and sex are combined. sPLA2 measurements at both time-points were ranked prior to correlation analyses owing to a right-skewed distribution. We performed Pearson's correlation on the sPLA2 ranks, as STATA does not have a function to perform partial Spearman's correlations.
Factors affecting sPLA2 levels from child to adulthoodParticipants were divided into four tracking groups based on their sPLA2 enzyme activity status from childhood to adulthood. Participants who remained in the upper quarter of age- and sex-specific sPLA2 distributions at both time-points were classified as persistent elevated; those who were in the upper quarter in childhood but not at follow-up were classified as resolution; those who were not in the upper quarter in childhood but were in adulthood were classified as incident; and those who did not have sPLA2 levels in the upper quarter at both childhood and adulthood were classified as persistent not elevated (Supplemental Fig. 1). This approach has been adopted in other studies examining factors that influence tracking of lipids and blood pressure between childhood and adulthood.23,24
Changes (adult minus child) in continuous variables (BMI, physical activity index, fruit consumption, vegetable consumption) were analysed using age- and sex-specific z-scores at each time-point. As an indicator of change or stability in SEP, we created a categorical social mobility variable25 that considered the highest level of parental (mother or father) occupation at baseline and participant occupation at follow-up.19 This variable has the following categories: persistently low (low at baseline and follow-up), persistently medium (medium at baseline and follow-up), persistently high (high at baseline and follow-up), upwardly mobile (moving from medium at baseline to high at follow-up, or low at baseline to medium or high at follow-up), and downwardly mobile (moving medium at baseline to low at follow-up, or from high at baseline to medium or low at follow-up). Participants were categorised into one of four categories based on their smoking status at both time-points: not smoking at either time-point, stopped smoking (smoking at baseline, not at follow-up), began smoking (did not smoke at baseline, smoked at follow-up), and smoker at both time-points.
Using logistic regression, we compared changes in the lifestyle-related variables of BMI, physical activity index, fruit consumption, vegetable consumption, smoking status, and social mobility between persistent elevated (reference) and resolution sPLA2 tracking groups and between persistent not elevated (reference) and incident sPLA2 tracking groups. As no significant sex interactions were observed, the data are not stratified by sex.
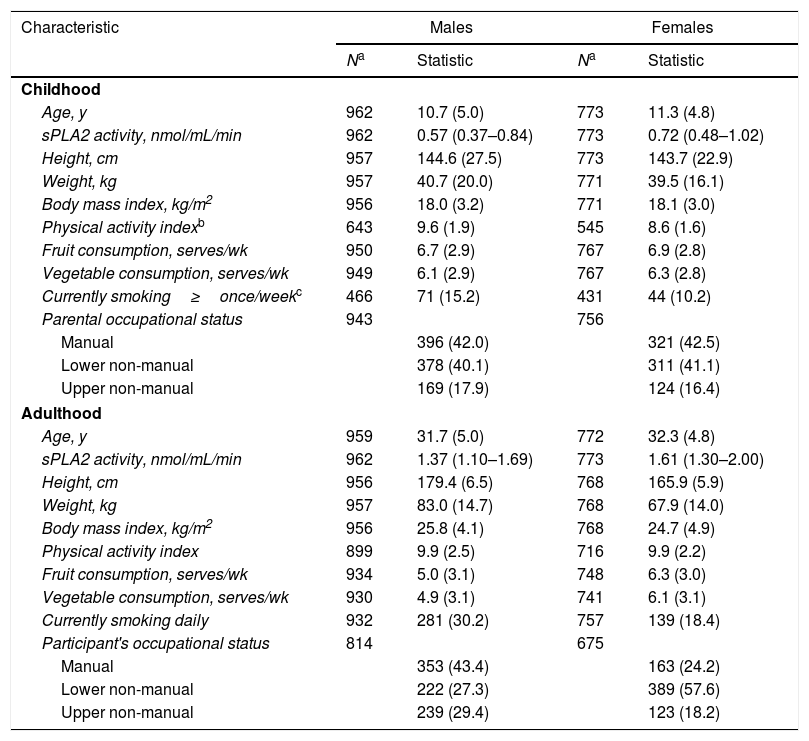
ResultsDemographicsCharacteristics outlining the population are presented in Table 1. At baseline and follow up, females had higher sPLA2 enzyme activity levels compared with males. Fig. 1 displays mean sPLA2 enzyme activity levels as a function of age at both time-points. There was a significant (negative) age trend for boys aged 3–18 years (p<0.001). There were no clear age trends in girls, or in adulthood for males or females.
Characteristics of up to 1735 participants in the Cardiovascular Risk in Young Finns Study who had secretory phospholipase (sPLA2) enzyme activity measurements in childhood (1980) and adulthood (2001).
| Characteristic | Males | Females | ||
|---|---|---|---|---|
| Na | Statistic | Na | Statistic | |
| Childhood | ||||
| Age, y | 962 | 10.7 (5.0) | 773 | 11.3 (4.8) |
| sPLA2 activity, nmol/mL/min | 962 | 0.57 (0.37–0.84) | 773 | 0.72 (0.48–1.02) |
| Height, cm | 957 | 144.6 (27.5) | 773 | 143.7 (22.9) |
| Weight, kg | 957 | 40.7 (20.0) | 771 | 39.5 (16.1) |
| Body mass index, kg/m2 | 956 | 18.0 (3.2) | 771 | 18.1 (3.0) |
| Physical activity indexb | 643 | 9.6 (1.9) | 545 | 8.6 (1.6) |
| Fruit consumption, serves/wk | 950 | 6.7 (2.9) | 767 | 6.9 (2.8) |
| Vegetable consumption, serves/wk | 949 | 6.1 (2.9) | 767 | 6.3 (2.8) |
| Currently smoking≥once/weekc | 466 | 71 (15.2) | 431 | 44 (10.2) |
| Parental occupational status | 943 | 756 | ||
| Manual | 396 (42.0) | 321 (42.5) | ||
| Lower non-manual | 378 (40.1) | 311 (41.1) | ||
| Upper non-manual | 169 (17.9) | 124 (16.4) | ||
| Adulthood | ||||
| Age, y | 959 | 31.7 (5.0) | 772 | 32.3 (4.8) |
| sPLA2 activity, nmol/mL/min | 962 | 1.37 (1.10–1.69) | 773 | 1.61 (1.30–2.00) |
| Height, cm | 956 | 179.4 (6.5) | 768 | 165.9 (5.9) |
| Weight, kg | 957 | 83.0 (14.7) | 768 | 67.9 (14.0) |
| Body mass index, kg/m2 | 956 | 25.8 (4.1) | 768 | 24.7 (4.9) |
| Physical activity index | 899 | 9.9 (2.5) | 716 | 9.9 (2.2) |
| Fruit consumption, serves/wk | 934 | 5.0 (3.1) | 748 | 6.3 (3.0) |
| Vegetable consumption, serves/wk | 930 | 4.9 (3.1) | 741 | 6.1 (3.1) |
| Currently smoking daily | 932 | 281 (30.2) | 757 | 139 (18.4) |
| Participant's occupational status | 814 | 675 | ||
| Manual | 353 (43.4) | 163 (24.2) | ||
| Lower non-manual | 222 (27.3) | 389 (57.6) | ||
| Upper non-manual | 239 (29.4) | 123 (18.2) | ||
Statistics are mean (SD) or median (25th, 75th percentiles) for continuous variables or N (percent) for categorical variables.
 enzyme activity levels as a function of age in males and females. Data for males indicated by black circles; data for females indicated by white circles. Sample sizes for each age and sex sub-group were: 3-years/24-years (males, n=150; females, n=82); 6-years/27-years (males, n=137; females, n=114); 9-years/30-years (males, n=175; females, n=129); 12-years/33-years (males, n=165; females, n=158); 15-years/36-years (males, n=175; females, n=156); 18-years/39-years (males, n=160; females, n=134).")
Estimated means and 95% confidence intervals for secretory phospholipase (sPLA2) enzyme activity levels as a function of age in males and females. Data for males indicated by black circles; data for females indicated by white circles. Sample sizes for each age and sex sub-group were: 3-years/24-years (males, n=150; females, n=82); 6-years/27-years (males, n=137; females, n=114); 9-years/30-years (males, n=175; females, n=129); 12-years/33-years (males, n=165; females, n=158); 15-years/36-years (males, n=175; females, n=156); 18-years/39-years (males, n=160; females, n=134).
Correlations between childhood and adult sPLA2 activity levels (range, males: r=0.31–0.44; females: r=0.25–0.58) were observed across both sexes and for all age groups (Supplemental Table 1). 42.3% of males and 35.8% of females who were in the highest quarter for sPLA2 levels in childhood remained in the highest quarter in adulthood (Supplemental Table 2). The proportion of participants in the lower quarter at both time-points was 41.2% for males and 48.4% for females. For the entire cohort, the rank-correlation for tracking of sPLA2 enzyme activity was r=0.41, upper quarter tracking was 39.4%, and lower quarter tracking was 44.3%. Fig. 2 displays rank correlations and proportion remaining in the upper quarter at both time-points for each age- and sex-stratum.

Pearson's correlation coefficients by baseline age for tracking of secretory phospholipase (sPLA2) enzyme activity between childhood and adulthood (upper figure portion); and percent remaining in the extreme quarter of the sample distribution for sPLA2 enzyme activity between childhood and adulthood by baseline age (lower figure portion). Data for males indicated by black line and bars; data for females indicated by grey line and bars.
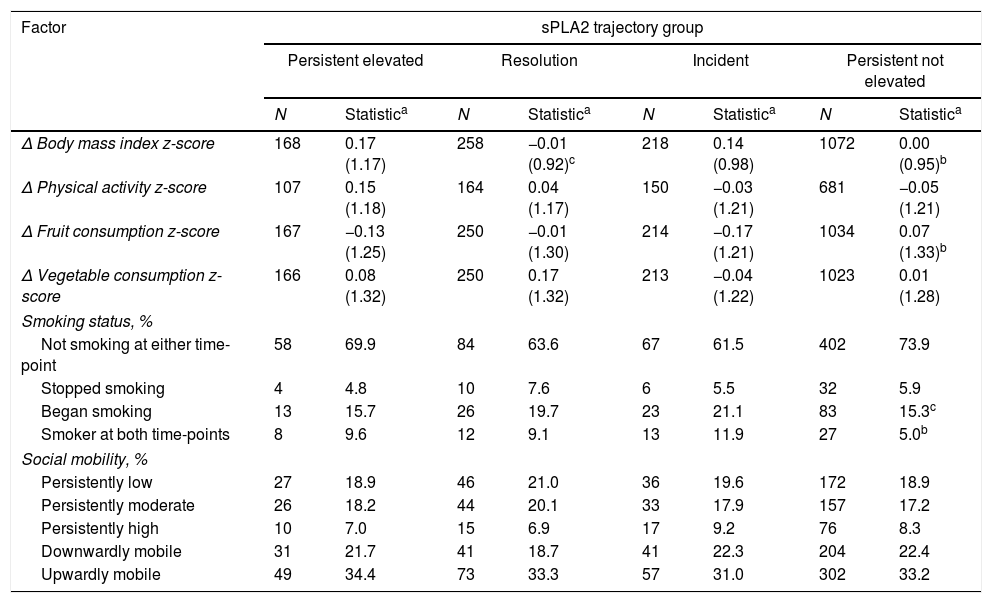
Table 2 shows the association of changes in different lifestyle factors on the tracking of sPLA2 enzyme activity groups. Compared with those in the persistent elevated group, the resolution group had decreased their BMI relative to peers who had experienced a relative increase in BMI.
Factors affecting tracking of secretory phospholipase A2 (sPLA2) enzyme activity from childhood (1980) to adulthood (2001) in the Cardiovascular Risk in Young Finns Study.
| Factor | sPLA2 trajectory group | |||||||
|---|---|---|---|---|---|---|---|---|
| Persistent elevated | Resolution | Incident | Persistent not elevated | |||||
| N | Statistica | N | Statistica | N | Statistica | N | Statistica | |
| Δ Body mass index z-score | 168 | 0.17 (1.17) | 258 | −0.01 (0.92)c | 218 | 0.14 (0.98) | 1072 | 0.00 (0.95)b |
| Δ Physical activity z-score | 107 | 0.15 (1.18) | 164 | 0.04 (1.17) | 150 | −0.03 (1.21) | 681 | −0.05 (1.21) |
| Δ Fruit consumption z-score | 167 | −0.13 (1.25) | 250 | −0.01 (1.30) | 214 | −0.17 (1.21) | 1034 | 0.07 (1.33)b |
| Δ Vegetable consumption z-score | 166 | 0.08 (1.32) | 250 | 0.17 (1.32) | 213 | −0.04 (1.22) | 1023 | 0.01 (1.28) |
| Smoking status, % | ||||||||
| Not smoking at either time-point | 58 | 69.9 | 84 | 63.6 | 67 | 61.5 | 402 | 73.9 |
| Stopped smoking | 4 | 4.8 | 10 | 7.6 | 6 | 5.5 | 32 | 5.9 |
| Began smoking | 13 | 15.7 | 26 | 19.7 | 23 | 21.1 | 83 | 15.3c |
| Smoker at both time-points | 8 | 9.6 | 12 | 9.1 | 13 | 11.9 | 27 | 5.0b |
| Social mobility, % | ||||||||
| Persistently low | 27 | 18.9 | 46 | 21.0 | 36 | 19.6 | 172 | 18.9 |
| Persistently moderate | 26 | 18.2 | 44 | 20.1 | 33 | 17.9 | 157 | 17.2 |
| Persistently high | 10 | 7.0 | 15 | 6.9 | 17 | 9.2 | 76 | 8.3 |
| Downwardly mobile | 31 | 21.7 | 41 | 18.7 | 41 | 22.3 | 204 | 22.4 |
| Upwardly mobile | 49 | 34.4 | 73 | 33.3 | 57 | 31.0 | 302 | 33.2 |
Totals for percentages may not add to 100 because of rounding.
Comparing incident and persistent not elevated sPLA2 enzyme activity groups, those in the incident group tended to have gained more BMI and decreased fruit consumption compared with those in the persistent not elevated group, who had maintained stable BMI and had increased fruit consumption relative to their peers. Those in the incident group were also more likely to have begun smoking since childhood (21.1% vs. 15.3%), or were a smoker at both time-points (11.9% vs. 5.0%).
DiscussionsPLA2 is a marker of vascular inflammation that might have a role in the pathogenesis of atherosclerosis. Since exposure to risk factors in childhood contributes to atherosclerosis later in life, we examined the ability to predict adult sPLA2 levels from measures collected in childhood (tracking). We showed that sPLA2 enzyme activity in childhood correlates with levels measured 21 years later in adulthood and that approximately 40% of children with high levels maintain this level to adulthood. Furthermore, our findings suggest that healthy improvements in the modifiable risk factors of fruit consumption, smoking status, and BMI have the potential to decrease the development of an elevated sPLA2 level in adulthood.
As no previous studies have examined the tracking of sPLA2 levels spanning childhood to adulthood, we provide comparison with tracking of other CVD risk factors reported in earlier findings from the Cardiovascular Risk in Young Finns Study (Supplemental Table 3).16 On the basis of rank correlations, sPLA2 enzyme activity tracked similarly compared with other established risk factors (lipoproteins, BMI, systolic blood pressure). Of interest, sPLA2 enzyme activity tracked more strongly than high-sensitivity C-reactive protein (hsCRP, r=0.43 vs. r=0.29), an inflammatory biomarker linked to atherosclerosis and CVD.6,16,20 Previously, we have found child lipoproteins, blood pressure, and BMI to predict adult carotid intima-media thickness (cIMT), an established preclinical marker of atherosclerosis, independent of adult levels of the same risk factors.26 However, child hsCRP was not associated with adult cIMT.16 Should a causal role of sPLA2 in preclinical atherosclerosis be confirmed, and if sPLA2 enzyme activity tracks as our data suggest, future studies could examine the utility of child sPLA2 enzyme activity levels to predict adult markers of atherosclerosis independent of other risk factors.
In the absence of support from clinical trials spanning multiple decades, our data also suggest positive changes made to lifestyle-related risk factors in the time between childhood and adulthood might help individuals to improve or maintain their sPLA2 enzyme activity trajectories. These data align with studies that have assessed the influence of lifestyle-related variables on tracking of other cardiovascular risk factors23,24 and cross-sectional observations in adults that suggested lifestyle factors (not smoking, healthy BMI, higher alcohol and protein intake) were associated with lower lipoprotein-associated phospholipase A2 levels, a family member of sPLA2 purported to have similar pro-atherosclerotic actions.27 Our data reinforce these previous findings by suggesting therapeutic lifestyle guidelines promoted in primary and primordial prevention guidelines for traditional risk factors have potential health benefits also for sPLA2 enzyme activity levels – which may further reduce CVD risk later in life. One potential mechanism underlying the association of healthy improvement in fruit consumption, smoking, BMI with change in sPLA2 levels may be a reduction in the production of proinflammatory cytokines tumour necrosis factor-α and interleukins that enhance synthesis and expression of sPLA2.28
This study had limitations. Serum samples used to assay sPLA2 levels were stored for up to 35 years with baseline and follow-up samples stored at different temperatures. It is not known how stable sPLA2 levels are under different storage temperatures or the rate of degradation over time. The difference in mean values of sPLA2 activity from 18 year olds stored since 1980 compared with those measured in 24 year olds stored since 2001 (Fig. 1) is more than might be expected by a 6-year age differential, which suggests degradation from longer storage. To mitigate this effect, and because all samples from each time-point were kept under the same conditions, our analyses examined tracking using ranks at both time-points rather than use of absolute levels. In addition, the consistent pattern in sPLA2 levels observed across birth cohorts at both time-points (Fig. 1) suggest that those with higher levels did not have greater degradation. As this is the first study to report sPLA2 enzyme activity levels in a population-based sample of children, we are unable to compare our sPLA2 enzyme activity levels with levels in children from similar studies analysed from fresh samples. Data from the self-reported questionnaires (SEP, smoking, diet, physical activity) may lead to recall bias, where participants may have failed to respond accurately. This would have likely resulted in underestimating the true effect, which may explain some instances where we observed non-significant differences between groups. Loss to follow-up from the original cohort is an unavoidable problem in any study conducted over an extended period of time. However, retention of participants is high in this cohort compared with similar studies.29,30 Because participants who remained in the study were more likely to be older and female, but otherwise similar in respect to other baseline variables,30 we believe bias owing to differential loss to follow-up to be limited. A further limitation is that data on sPLA2 levels were only available at two time-points and we cannot determine when changes in sPLA2 levels occurred, nor identify those who underwent multiple changes during the 21-year period. Finally, because the cohort is racially homogenous, these findings can only be generalised to Caucasians in Europe.
This study had several strengths. Due to the storage of samples since childhood, we were able to provide the presented data long before contemporary cohorts could examine similar aims. The large sample size, long duration of follow-up, with participants of different social backgrounds and who are well phenotyped allows our findings to be generalised at a population level and to infer long-term estimates of effect.30
Our findings show that childhood elevations in sPLA2 levels associate with elevated sPLA2 levels in adulthood. Further, our data suggest that intervention and prevention programmes that aim to improve conventional modifiable risk factors for CVD by advocating for not smoking, higher fruit consumption, and reduced excess adiposity in the time between childhood and adulthood might influence whether individuals maintain, develop, or resolve elevated child sPLA2 levels.
FundingThe Cardiovascular Risk in Young Finns Study was financially supported by the Academy of Finland (grants 117787, 121584, 126925, 124282, 129378, 41071), the Social Insurance Institution of Finland, the Turku University Foundation, Kuopio, Tampere and Turku University Hospital Medical Funds, Special Federal Grants for University Hospitals, the Juho Vainio Foundation, Paavo Nurmi Foundation, the Finnish Foundation of Cardiovascular Research, Orion-Farmos Research Foundation, Turku University Foundation, the Finnish Cultural Foundation and the Finnish Centre of Excellence in Cardiovascular and Metabolic Disease. CGM is supported by a National Heart Foundation of Australia Future Leader Fellowship (100849).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Chung O, Juonala M, Mallat Z, Hutri-Kähönen N, Viikari JS, Raitakari OT, et al. Tracking of secretory phospholipase A2 enzyme activity levels from childhood to adulthood: a 21-year cohort. J Pediatr (Rio J). 2019;95:247–54.




