

To analyze the available evidence regarding the efficacy of using therapeutic play on behavior and anxiety in children undergoing invasive procedures.
Data sourceThe systematic review search was performed in the MEDLINE, LILACS, CENTRAL and CINAHL databases. There was no limitation on the year or language.
Synthesis of dataThe literature search found 1892 articles and selected 22 for full reading. Eight articles were excluded, as they did not address the objectives assessed in this review. Twelve studies, representing 14 articles, were included. The studies were conducted between 1983 and 2015, five in Brazil, one in the United States, five in China, one in Lebanon, one in Taiwan, and one in Iran. Most studies showed that intervention with therapeutic play promotes reduction in the level of anxiety and promotes collaborative behavior and acceptance of the invasive procedure.
ConclusionsEvidence related to the use of therapeutic play on anxiety and behavior of children undergoing invasive procedures is still questionable. The absence, in most studies, of the creation of a random sequence to assign the subjects to either the control or the experimental group, as well as allocation concealment, are factors that contribute to these questions. Another issue that characterizes an important source of bias is the absence of blinded evaluators. It is necessary to perform further studies that will take into account greater methodological stringency.
Revisar, de forma sistemática, as evidências em relação a eficácia da utilização do brinquedo terapêutico sobre o comportamento e a ansiedade de crianças submetidas a procedimentos invasivos.
Fontes dos dadosA busca da revisão sistemática foi efetuada nas bases MedLine, Lilacs, CENTRAL e CINAHL. Não houve limitação quanto ao ano ou idioma.
Síntese dos dadosNa busca de literatura foram encontrados 1892 artigos e selecionados 22 para leitura integral. Foram excluídos 8 artigos que não respondiam aos objetivos avaliados nesta revisão. Foram incluídos 12 estudos, correspondentes a 14 artigos. Os estudos foram conduzidos entre 1983 e 2015, cinco no Brasil, um nos Estados Unidos, cinco na China, um no Líbano, um em Taiwan e um no Irã. A maioria dos estudos mostrou que a intervenção com brinquedo terapêutico promove redução no nível de ansiedade e favorece um comportamento de colaboração e aceitação do procedimento invasivo.
ConclusõesAs evidências relacionadas ao uso do brinquedo terapêutico sobre a ansiedade e comportamento de crianças submetidas a procedimentos invasivos ainda são questionáveis. A ausência, na maioria dos estudos, de uma geração de sequência aleatória para direcionamento dos sujeitos para os grupos controle ou experimental e do sigilo de alocação são fatores que contribuem para este questionamento. Uma outra questão que caracteriza importante fonte de viés é o não cegamento dos avaliadores. Se faz necessário a realização de novas pesquisas que levem em consideração um maior rigor metodológico.
The degree of the children's understanding about the procedure to which they will be submitted may be related to the period of stress and insecurity that they will experience. Their behavior may vary according to age, environment, the presence of strangers, and invasive procedures experienced by the children or observed in others. These factors contribute to the development of unpleasant reactions such as fear, anxiety, and resistance to the procedures that will be performed. Hospitalization means attacking their playful and magical realm, and therefore requires that the assisting professional understands their childhood world.1,2
Excessive stress and anxiety experienced by children can affect their physical and physiological health, hinder their ability to deal with medical procedures, cause changes in their behavior, and affect their recovery from illness. Therefore, there is an urgent need for clinical researchers to develop, implement, and evaluate interventions that can minimize the children's anxiety level and improve their ability to handle the stress of hospitalization and invasive procedures.3
Over the past decades, several studies that addressed children's health care have discussed different methods of educational interventions for children before or during hospitalization, when surgical and invasive medical procedures are performed.4–9
The need to play is not eliminated when children become ill or are hospitalized; on the contrary, children who can play may feel safer during the transoperative period, even in a strange environment.10 One aspect of such activities is therapeutic play, which provides a structured play activity, follows the principles of play therapy, and has specific objectives to be achieved. Its use brings relief from anxiety caused by atypical experiences for age that tend to appear as threatening, requiring an intervention that will help the child/family to cope while undergoing a highly complex invasive procedure.11
Studies have shown the benefits of therapeutic play in reducing anxiety and postoperative pain in hospitalized children.12 Clinical trials have shown the positive effects of therapeutic play intervention on perioperative anxiety, postoperative pain, and negative behavior in children submitted to surgical procedures.7,9
Thus, with the objective of contributing to the knowledge about the use of therapeutic play, which is an important strategy to be used in childcare, this review aimed to systematically assess the evidence regarding the efficacy of using therapeutic play on the behavior and anxiety in children undergoing invasive procedures.
MethodThe protocol of this review is registered at the international database for systematic reviews, PROSPERO, under number CRD42016035878, and can be accessed at (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016035878). This article was written according to PRISMA recommendations for systematic reviews.13
A systematic review of the literature was carried out between November 2015 and February 2016, through a search in the MEDLINE, LILACS, CENTRAL, and CINAHL databases.
A specific strategy crossing the descriptors or keywords for retrieving subjects from scientific literature was created for each search portal.
In MEDLINE, through the PubMed search portal, the search strategy was performed using the syntax: ((“Child, Preschool”[Mesh] OR “Child, Hospitalized”[Mesh] OR “Child”[Mesh] OR “Children”[Mesh]) AND (“Play and Playthings”[Mesh] OR “Play Therapy”[Mesh] OR “Therapeutic Play”[Mesh]) AND (“Nurses”[Mesh] OR “Speech”[Mesh] OR “Pediatric Nurse Practitioners”[Mesh] OR “Pain Management”[Mesh] OR “Child Behavior”[Mesh] OR “Psychology, Child”[Mesh] OR “Surgery”[Mesh] OR “Pediatric surgery procedure”[Mesh] OR “Preoperative Care”[Mesh])).
In Lilacs, the strategy used was: “CHILD” OR “PRESCHOOLER” AND (play and playthings) OR (Play Therapy through) OR (Therapeutic play) AND (perioperative Nursing) OR (Humanization of assistance) OR Communication OR (Pediatric Nursing) OR (Pain Intervention) OR (Child Behavior) OR (Child Psychology) OR (Pre-Operative Care) OR (Clinical Procedures) OR (Surgery) OR (Pediatric Surgery) OR (Play Therapy)., however, search strategy in Lilacs, was performed with terms in Portuguese.
In the CENTRAL and CINAHL databases: ((“Child, Preschool” OR “Child, Hospitalized” OR “Child” OR “Children”) AND (“Play and Playthings” OR “Play Therapy” OR “Therapeutic Play”) AND (“Nurses” OR “Speech” OR “Pediatric Nurse Practitioners” OR “Pain Management” OR “Child Behavior” OR “Psychology, Child” OR “Surgery” OR “Pediatric surgery procedure” OR “Preoperative Care”)).
After the articles were located, the eligibility, selection, and exclusion criteria were applied. The following were considered eligible: original articles (clinical trials and quasi-experimental studies) that had preschoolers and school-aged children as the study population and that used therapeutic play as the intervention to prepare children submitted to invasive procedures. Annals from congresses were excluded, as well as theses, dissertations, letters to the editor, and articles not consistent with the study question. There was no limitation regarding the year or language of publication.
Initially the article titles were read and, after excluding those that did not meet the eligibility criteria, their abstracts were analyzed according to the same criteria. These steps were performed independently by two authors of this systematic review. In case of disagreement regarding the exclusion of the abstracts, the articles were read in full.
After the articles were read in full, a new exclusion was carried out, according to the same study selection criteria. Disagreements were resolved by consensus or after consulting a third reviewer. A standard form prepared by the authors was used for data extraction.
The decision regarding the risk of bias was performed in two steps. The first was related to the description of what was reported in each study, in sufficient details so that the decision was made based on this information. The second part consisted of a decision regarding the risk of bias for each of the analyzed parameters, which were classified into three categories: low risk of bias, high risk of bias, and uncertain bias, according to the recommendations of the tool developed by the Cochrane Collaboration for bias risk assessment in randomized clinical trials.14,15
ResultsA total of 1892 articles were found: 1052 in MEDLINE, 95 in CENTRAL, 722 in CINAHL, and 23 in LILACS. Of these, 1861 were excluded for not meeting the eligibility criteria and 10 were excluded because they were duplicates. After reading the 21 articles in full, the final sample of this review comprised 12 studies, corresponding to 14 articles, taking into account that one of the studies generated three publications. Fig. 1 shows the process of article selection.

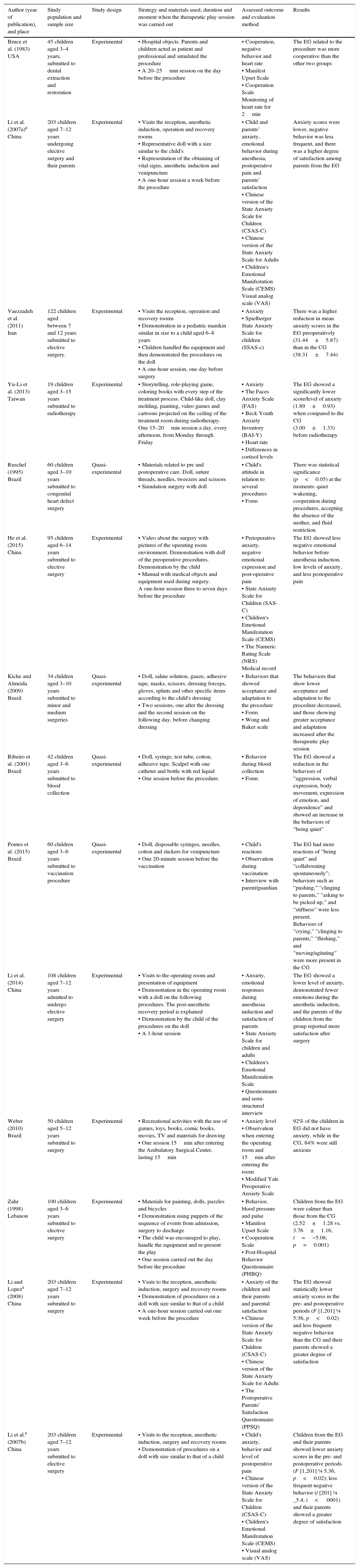
Of the 14 articles, ten were randomized controlled trials and four were quasi-experimental studies. The studies were carried out between 1983 and 2015 in the following countries: five in Brazil, one in the United States, five in China, one in Lebanon, one in Taiwan, and one in Iran. The studies were conducted in large and small hospitals. The participants were aged between 3 and 15 years (938 participants). Detailed information regarding the articles included in this review is shown in Table 1.
Synthesis of the articles.
| Author (year of publication), and place | Study population and sample size | Study design | Strategy and materials used, duration and moment when the therapeutic play session was carried out | Assessed outcome and evaluation method | Results |
|---|---|---|---|---|---|
| Bruce et al. (1983) USA | 45 children aged 3–4 years, submitted to dental extraction and restoration | Experimental | • Hospital objects. Parents and children acted as patient and professional and simulated the procedure • A 20–25min session on the day before the procedure | • Cooperation, negative behavior and heart rate • Manifest Upset Scale • Cooperation Scale Monitoring of heart rate for 2min | The EG related to the procedure was more cooperative than the other two groups |
| Li et al. (2007a)a China | 203 children aged 7–12 years undergoing elective surgery and their parents | Experimental | • Visits the reception, anesthetic induction, operation and recovery rooms • Representative doll with a size similar to the child's • Representation of the obtaining of vital signs, anesthetic induction and venipuncture • A one-hour session a week before the procedure | • Child and parents’ anxiety, emotional behavior during anesthesia, postoperative pain and parents’ satisfaction • Chinese version of the State Anxiety Scale for Children (CSAS-C) • Chinese version of the State Anxiety Scale for Adults • Children's Emotional Manifestation Scale (CEMS) Visual analog scale (VAS) | Anxiety scores were lower, negative behavior was less frequent, and there was a higher degree of satisfaction among parents from the EG |
| Vaezzadeh et al. (2011) Iran | 122 children aged between 7 and 12 years submitted to elective surgery. | Experimental | • Visits the reception, operation and recovery rooms • Demonstration in a pediatric manikin similar in size to a child aged 6–8 years • Children handled the equipment and then demonstrated the procedures on the doll • A one-hour session, one day before surgery | • Anxiety • Spielberger State Anxiety Scale for children (SSAS-c) | There was a higher reduction in mean anxiety scores in the EG preoperatively (31.44±5.87) than in the CG (38.31±7.44) |
| Yu-Li et al. (2013) Taiwan | 19 children aged 3–15 years submitted to radiotherapy | Experimental | • Storytelling, role-playing game, coloring books with every step of the treatment process. Child-like doll, clay molding, painting, video games and cartoons projected on the ceiling of the treatment room during radiotherapy. One 15–20min session a day, every afternoon, from Monday through Friday | • Anxiety • The Faces Anxiety Scale (FAS) • Beck Youth Anxiety Inventory (BAI-Y) • Heart rate • Differences in cortisol levels | The EG showed a significantly lower score/level of anxiety (1.89±0.93) when compared to the CG (3.00±1.33) before radiotherapy |
| Ruschel (1995) Brazil | 60 children aged 3–10 years submitted to congenital heart defect surgery | Quasi-experimental | • Materials related to pre and postoperative care. Doll, suture threads, needles, tweezers and scissors • Simulation surgery with doll | • Child's attitude in relation to several procedures • Form | There was statistical significance (p<0.05) at the moments: quiet wakening, cooperation during procedures, accepting the absence of the mother, and fluid restriction |
| He et al. (2015) China | 95 children aged 6–14 years submitted to elective surgery | Experimental | • Video about the surgery with pictures of the operating room environment. Demonstration with doll of the preoperative procedures. Demonstration by the child • Manual with medical objects and equipment used during surgery. A one-hour session three to seven days before the procedure | • Perioperative anxiety, negative emotional expression and post-operative pain • State Anxiety Scale for Children (SAS-C) • Children's Emotional Manifestation Scale (CEMS) • The Numeric Rating Scale (NRS) Medical record | The EG showed less negative emotional behavior before anesthesia induction, low levels of anxiety, and less postoperative pain |
| Kiche and Almeida (2009) Brazil | 34 children aged 3–10 years submitted to minor and medium surgeries | Quasi-experimental | • Doll, saline solution, gauze, adhesive tape, masks, scissors, dressing forceps, gloves, splints and other specific items according to the child's dressing • Two sessions, one after the dressing and the second session on the following day, before changing dressing | • Behaviors that showed acceptance and adaptation to the procedure • Form • Wong and Baker scale | The behaviors that show lower acceptance and adaptation to the procedure decreased, and those showing greater acceptance and adaptation increased after the therapeutic play session |
| Ribeiro et al. (2001) Brazil | 42 children aged 3–6 years submitted to blood collection | Quasi-experimental | • Doll, syringe, test tube, cotton, adhesive tape. Scalpel with one catheter and bottle with red liquid • One session before the procedure. | • Behavior during blood collection • Form | The EG showed a reduction in the behaviors of “aggression, verbal expression, body movement, expression of emotion, and dependence” and showed an increase in the behaviors of “being quiet” |
| Pontes et al. (2015) Brazil | 60 children aged 3–6 years submitted to vaccination procedure | Quasi-experimental | • Doll, disposable syringes, needles, cotton and stickers for venipuncture • One 20-minute session before the vaccination | • Child's reactions • Observation during vaccination • Interview with parent/guardian | The EG had more reactions of “being quiet” and “collaborating spontaneously”; behaviors such as “pushing,” “clinging to parents,” “asking to be picked up,” and “stiffness” were less present. Behaviors of “crying,” “clinging to parents,” “flushing,” and “moving/agitating” were more present in the CG |
| Li et al. (2014) China | 108 children aged 7–12 years admitted to undergo elective surgery | Experimental | • Visits to the operating room and presentation of equipment • Demonstration in the operating room with a doll on the following procedures. The post-anesthetic recovery period is explained • Demonstration by the child of the procedures on the doll • A 1-hour session | • Anxiety, emotional responses during anesthesia induction and satisfaction of parents • State Anxiety Scale for children and adults • Children's Emotional Manifestation Scale • Questionnaire and semi-structured interview | The EG showed a lower level of anxiety, demonstrated fewer emotions during the anesthetic induction, and the parents of the children from the group reported more satisfaction after surgery |
| Weber (2010) Brazil | 50 children aged 5–12 years submitted to surgery | Experimental | • Recreational activities with the use of games, toys, books, comic books, movies, TV and materials for drawing • One session 15min after entering the Ambulatory Surgical Center, lasting 15min | • Anxiety level • Observation when entering the operating room and 15min after entering the room • Modified Yale Preoperative Anxiety Scale | 92% of the children in EG did not have anxiety, while in the CG, 84% were still anxious |
| Zahr (1998) Lebanon | 100 children aged 3–6 years submitted to elective surgery | Experimental | • Materials for painting, dolls, puzzles and bicycles • Demonstration using puppets of the sequence of events from admission, surgery to discharge • The child was encouraged to play, handle the equipment and re-present the play • One session carried out the day before the procedure | • Behavior, blood pressure and pulse • Manifest Upset Scale • Cooperation Scale • Post-Hospital Behavior Questionnaire (PHBQ) | Children from the EG were calmer than those from the CG (2.52±1.28 vs. 3.76±1.16, t=−5.08; p=0.001) |
| Li and Lopeza (2008) China | 203 children aged 7–12 years submitted to surgery | Experimental | • Visits to the reception, anesthetic induction, surgery and recovery rooms • Demonstration of procedures on a doll with size similar to that of a child • A one-hour session carried out one week before the procedure | • Anxiety of the children and their parents and parental satisfaction • Chinese version of the State Anxiety Scale for Children (CSAS-C) • Chinese version of the State Anxiety Scale for Adults • The Postoperative Parents’ Satisfaction Questionnaire (PPSQ) | The EG showed statistically lower anxiety scores in the pre- and postoperative periods (F [1,201] ¼ 5:36, p<0.02) and less frequent negative behavior than the CG and their parents showed a greater degree of satisfaction |
| Li et al.a (2007b) China | 203 children aged 7–12 years submitted to elective surgery | Experimental | • Visits to the reception, anesthetic induction, surgery and recovery rooms • Demonstration of procedures on a doll with size similar to that of a child | • Child's anxiety, behavior and level of postoperative pain • Chinese version of the State Anxiety Scale for Children (CSAS-C) • Children's Emotional Manifestation Scale (CEMS) • Visual analog scale (VAS) | Children from the EG and their parents showed lower anxiety scores in the pre- and postoperative periods (F [1,201] ¼ 5.36, p<0.02); less frequent negative behavior (t [201] ¼ _5.4, i<.0001) and their parents showed a greater degree of satisfaction |
EG, experimental group; CG, control group.
In this review, all studies used therapeutic play to prepare children who would be submitted to invasive procedures. The materials and strategies used during the sessions were varied: representative dolls with size similar to the child,9,16–19 dolls,20–22 hospital objects,20–25 storytelling, role playing, coloring books with all steps of the treatment, clay molding, painting, video games and cartoons projected on the ceiling of the treatment room during the procedure,26 videos about the surgery with pictures of the operating room environment, play activities with the use of toys, games, books, comics, movies, television and drawing materials,7,27 and demonstration with the use of puppets.7 One study also asked the children to take their favorite doll.26 The duration of each therapeutic play session ranged from 15minutes to one hour.
Additionally, some studies also included a visit to the reception, anesthetic induction, operation, and recovery rooms, mimicking the entire treatment process, from the child's admission into the hospital to the operating room.9,16–19 In ten articles, the children were submitted to elective surgery7,9,16–20,24,25,27 and the other procedures consisted of radiotherapy,26 vaccination,22 blood collection,21 and dental treatment.23
In this review, the outcomes of interest were the child's anxiety and behavior when submitted to an invasive procedure; of the 14 articles found, four analyzed only anxiety,17,19,26,27 while another six analyzed behavior,4,7,20–22,24 and four analyzed both outcomes.9,16,18,25
Other analyzed outcomes concerned the effect of therapeutic play through the analysis of physiological indicators such as heart rate,23,26 blood pressure and pulse,7 and salivary cortisol level.26 Additionally, the level of postoperative pain was evaluated in three articles,9,18,25 and the parents’ satisfaction and anxiety were also verified.9,16,19
Several tools were used to analyze the level of anxiety, which were mostly scales, including the Chinese version of the State Anxiety Scale for Children (CSAS-C),9,16,18,19 the Spielberger State Anxiety Scale for children (SSAS-c),17 the Face Anxiety Scale (FAS), the Beck Youth Anxiety Inventory (BAI-Y),26 the State Anxiety Scale for Children (SAS-C),25 and the modified Yale Preoperative Anxiety Scale (YPAS).27
The timing of outcome verification varied in the 12 studies. Most verified the outcome before and after surgery. Other studies verified it at admission and during the preoperative anesthetic injection. One study assessed it two weeks later.7 Other moments were during venipuncture, when the wound dressings were being performed, during anesthetic induction, at the removal of pacemaker wires, and at physical examination, among others.
The following tools were used to analyze behavior: the Cooperation Scale and Manifest Upset Scale,7,23 the Children's Emotional Manifestation Scale,9,16,18,25 a form created by the researcher,20,21,24 the Wong and Baker Scale,20 and interview with a parent/guardian.22
As for the methodological quality of the articles, only one study generated the allocation sequence in the groups in a truly random fashion, by using a software program Research Randomizer (Urbaniak. G.C., & Plous. S. (2013). Research Randomizer (Version 4.0) from http://www.randomizer.org/) and protected concealment by using opaque envelopes of the same size within a box, with participant instruction conducted by telephone.25 Four articles used a simple randomization method by drawing lots, using balls: one identified with the experimental group and the other with the control group – one ball was taken for each child and was then put back into the bag.9,16,17,19 The others that carried out clinical trials did not report the method used for the randomization.
There was no blinding of the participants in any of the studies, as it was not necessary, considering the characteristic of the intervention (therapeutic play). However, the evaluator was blinded in five studies.7,16,17,23,25 Regarding sample loss, only one study indicated that18 and used the appropriate statistical analysis in a clear manner. Similarly, only one showed protocol publication regarding the research, available online.25
AnxietyIn this review, the articles that analyzed the effectiveness of therapeutic play on the perioperative anxiety level of children undergoing invasive medical procedures used different measurement tools. In the four articles that proposed to verify the effect only on anxiety, this assessment was conducted by measuring it before and after surgery.9,16,17,19 Another study performed it at admission and during the preoperative anesthetic injection.7
Studies show that after the intervention with the use of therapeutic play the children in the experimental group had lower levels of anxiety when compared to the control group (p<0.05).19,26,27 Even in a study in which play activities were used at the moment prior to the surgery in a recreation room during a short 15-minute period, it found that 92% of children in the experimental group did not display anxiety.27
When analyzing the effect of time on anxiety levels, a statistically significant variation (F=3.260, p<0.05) was observed in both groups, while there was no statistically significant group effect (F=0.637, p>0.05) and interaction effect (F=0.368, p>0.05), which was confirmed by repeated measurements, after adjusting for possible confounding factors such as gender, age, type of surgery, body weight, duration of surgery, and pain medication use.
BehaviorAll articles assessing behavior showed that children in the experimental group were more collaborative and showed more acceptance reactions to the procedure when compared to the control group. Seven studies express these results with a statistically significant difference (p<0.05).
One study indicated that the therapeutic play intervention significantly reduced the negative emotional behavior of children before anesthetic induction.9 In the study by Zahr in 1998,7 the children in the experimental group showed fewer negative behaviors within two weeks after surgery, with the change in behavior being measured by Post Hospitalization Behavior Questionnaire (PHBQ).
The children in the experimental group were more collaborative; they screamed, demanded, denied, wept, and moved less than those in the control group.21 Regarding the assessment of negative emotional behaviors using the Children's Emotional Manifestation Scale (CEMS), another study found that children in the experimental group had significantly lower mean CEMS scores before anesthetic induction than those in the control group (F=13.452, p<0.01).25
Children who received the therapeutic play intervention exhibited fewer emotions at the anesthetic induction, with a large effect size for the intervention.18 Children who received the intervention exhibited significantly less negative emotional behavior before the anesthetic induction (t [201] ¼ –5.4, p<0.001).9
DiscussionChildren submitted to invasive medical procedures undergo all types of psychological and physical stress, as do their families. Very often, the hospital environment to which the child is exposed is quite frightening, where this child's anxiety and behavioral cycle is altered.28 Thus, it is essential to understand the best ways to mitigate the negative alterations in these factors.
This is the first systematic review on therapeutic play intervention in children submitted to several invasive procedures, with no time limit for the publication of studies, considering that a previously published review on this topic had a population of children undergoing elective surgery only and included articles published between 1995 and 2012, in addition to also restricting the publication language.29
The studies included in this review were carried out in developed and developing countries, large and small hospitals, with children's ages within a wide range, submitted to several invasive procedures such as elective surgery, vaccination, blood collection, and dental treatment. This demonstrates the use of therapeutic play in different scenarios, supporting effective communication with the child, seeking to reduce the probability of developing trauma, as well as promoting collaborative behavior before an invasive procedure is performed.
Several materials and strategies were used during the therapeutic play sessions. However, of the 14 articles, 13 used a doll and hospital objects to show the children the procedure to which they would be submitted.
The use of these tools is in accordance with the statement that, from the pre-operational stage, the child starts to develop the ability to think about objects and events that are not present in her immediate environment and begins to represent them through mental figures, sounds, images, words, or other forms. This new ability allows them to exceed the limits of the “here and now” and begin to understand that a mental image or idea may represent a symbol for an object or a lived experience.30
Five articles9,16–19 used in the experimental group, in addition to therapeutic play, visits to the reception, surgery, anesthesia induction, and recovery rooms in order to promote the child's familiarization with the environment. In these cases, this may be considered a study limitation, because the association of another therapeutic measure may have overestimated the effect of therapeutic play on the children's anxiety level and behavior in these studies.
No standardization exists in the choice of tool to analyze the children's anxiety and behavior. Most studies chose to use validated scales, guaranteeing that their application allows the true measurement of what is to be assessed.31 The use of physiological indicators such as blood pressure, heart rate, and cortisol level is very important to add evidence regarding the impact of therapeutic play use on the child's emotional state; however, these measures have been used in few studies.
Most studies have found positive changes in the behavior of children who participated in the therapeutic play session, as well as reduction in anxiety scores after the intervention, when compared to the control group. However, few studies analyzed whether this difference was statistically significant. Some studies showed results only in absolute and relative frequencies, making it difficult to evaluate whether the intervention made a difference regarding the child's anxiety and behavior.
Of the nine articles that assessed anxiety, three9,18,23 did not have enough information on randomization and allocation concealment, which complicates the bias risk analysis in relation to these points, while two studies26,27 did so inadequately. Whatever the assessed intervention or outcome was, one of the fundamental principles for conducting clinical trials is the randomization of subjects to provide the maximum possible homogeneity between groups and allow the inference that the assessed differences may be due to the intervention.32
Four articles showed low risk of bias regarding the generation of the subjects’ sequence and allocation. In this sense, the lack of the adequate generation of sequence and allocation concealment compromises the evidence provided by these studies for this outcome, indicating a certain degree of uncertainty of the findings.
Regarding the behavior outcome, five studies7,20–22,24 did not perform random allocation of subjects, making it impossible for all the participants to have the same chance of being allocated in one of the groups (control and intervention). Also, they did not report on allocation concealment. Two articles18,23 did not have enough information regarding the generation of subject randomization sequence and allocation concealment, which makes it impossible to analyze of the bias risk for these parameters. Therefore, the evidence provided by these studies regarding the effects of the therapeutic play on the behavior of children undergoing invasive procedures is questionable.
In educational interventions such as therapeutic play, it is difficult to blind the participants33 because the experimental group members are aware that the therapeutic play intervention is not part of the usual hospital care. In studies where a group is submitted to an intervention and another to the usual routine care, blinding the researcher or the professional who will perform the procedure is not possible. The lack of blinding of participants does not represent an important source of bias, since it is not expected for children to intentionally change their behavior when they know they are being assessed or because they participated in a certain intervention.
It is possible to blind the evaluator, but this only occurred in the evaluation after the intervention in two studies that assessed only behavior,7,23 one that assessed only anxiety,19 and another that assessed anxiety and behavior.25 The lack of evaluator blinding in most studies represents a risk of high bias, which makes the evidence questionable.
As for incomplete outcomes, most studies showed insufficient information to assess this risk, as they were unclear whether there was a loss of data, except one18 that assessed anxiety and behavior, and recorded the loss of five members from the intervention group and four in the follow-up. However, the reason was not explained and there was no information regarding whether any adjustment was made in the analysis to consider these losses. In 2015, He et al.25 evaluated anxiety and behavior and reported that no losses occurred during the study, which implies low risk of bias. At this point, the analysis of evidence becomes uncertain.
Possible risks to the validity of intervention studies in children have been discussed in the literature, among which are: insufficient statistical power,34 little concern for the reliability and validity of measuring tools,35 insufficient verification of an intervention,36 lack of minimization of attrition bias,37 inability to control observer bias,8 and inability to ensure the integrity and uniformity of treatment.38
ConclusionEvidence related to the use of therapeutic play on anxiety and behavior of children undergoing invasive procedures is still questionable. The absence, in most studies, of the creation of a random sequence to assign the subjects to either the control or the experimental group, as well as allocation concealment, are factors that contribute to these questions. Another issue that characterizes an important source of bias is the absence of blinded evaluators.
Therefore, it is necessary to perform further studies that will take into account greater methodological stringency, especially regarding the allocation of subjects, use of validated tools, and blinded evaluators, so that the risk of bias related to these domains can be minimized.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silva RD, Austregésilo SC, Ithamar L, Lima LS. Therapeutic play to prepare children for invasive procedures: a systematic review. J Pediatr (Rio J). 2017;93:6–16.
Study conducted at Universidade Federal de Pernambuco (UFPE), Recife, PE, Brazil.




