






Meckel diverticulum (MD) is a common malformation of the digestive tract, often accompanied by serious complications. It is important to find safe and effective diagnostic methods for screening MD. The aim of this study was to evaluate the effectiveness of a technetium-99m (Tc-99m) scan for pediatric bleeding MD.
MethodsThe authors conducted a systematic review of studies published in PubMed, Embase, and Web of Science before 1 January 2023. Studies based on PICOS were included in this systematic review. The flow chart was made by PRISMA software. The quality of included studies was assessed by RevMan5 software (QUADAS-2: Quality Assessment of Diagnostic Accuracy Studies-2). The sensitivity, specificity, and other measurements of accuracy were pooled using Stata/SE 12.0 software.
ResultsSixteen studies with 1115 children were included in this systematic review. A randomized-effects model was used for the meta-analysis because of significant heterogeneity. The combined sensitivity and specificity were 0.80 [Confidence Interval (95% CI, 0.73-0.86) and 0.95 (95% CI, 0.86-0.98)], respectively. The area under the curve (AUC) was 0.88 (95% CI, 0.85-0.90). Publication bias (Begg's test p = 0.053) was observed.
ConclusionTc-99m scan has high specificity, but moderate sensitivity, which is always influenced by some factors. Hence, the Tc-99m scan has some limitations in the diagnosis of pediatric bleeding MD.
Meckel diverticulum (MD) has an incidence rate of 1-3% in the population. It is an embryonic residue after incomplete closure of the umbilical mesenteric canal 1 Only 25-40% of the cases have clinical symptoms,2 but 80% of the patients under 15 years of age have clinical symptoms.3 About 20% of MD cases have ectopic gastric mucosal (EGM) disease.4,5 EGM is a type of pathological tissue, most often located in MD, and is the most common cause of lower gastrointestinal bleeding in children, typically before two years of age.6 So early diagnosis of MD is important.
Although the diagnosis of a symptomatic MD is often difficult, Technetium-99m (Tc-99m) scanning can be performed in ectopic gastric mucosa. Approximately 90% of bleeding MDs contain heterotopic mucosa, which prompted the development of the Tc-99m scan.7,8
Tc-99m is helpful in the diagnosis of ectopic gastric mucosa because it compares other sites with relatively low radiographic findings.9-13 Moreover, the Tc-99m scan is a non-invasive test with a low radiation burden and simple operation. However, specialized expertise is necessary to acquire and interpret the images, and appropriate guidelines to perform a high-quality scan have been published.14 The aim of this study was to assess the utility of a Tc-99m scan in the diagnostic workup of pediatric patients with MD.
Materials and methodsThis meta-analysis and systematic review were completed in accordance with the PRISMA guidelines.
Literature searchThe PubMed, Embase, and Cochrane Library were searched to identify relevant studies published from inception to 1 January 2023. The search strategy consisted of the following keywords: (Meckel diverticulum) AND (Tc-99m scan). The authors contacted the original authors of the relevant studies to obtain additional information if required.
Study selectionStudies were included when the following criteria were met: (1) children; (2) Tc-99m scan was used as the test method; (3) surgical pathology examination was used as the reference standard; (4) randomized controlled trial (RCT), cohort study or case-control study.
Studies were excluded when the following criteria were met: (1) review, conference records, case reports, and animal experiments; (2) multiple studies based on the same data; (3) non-English studies.
Study screening and data extractionBased on the inclusion and exclusion criteria, two researchers screened the literature, extracted data, and cross-checked the information. In case of discrepancies, the author of the original article was contacted for clarification. The following basic characteristics were extracted: country, experimental design, and original experimental data [the number of cases of TP (true positive), TN (true negative), FP (false positive), and FN (false negative)]. The authors defined a positive Tc-99m scan with negative results for both surgical exploration and Meckel diverticulum ultrasound as an "FP" and a negative Tc-99m scan, Meckel diverticulum ultrasound, and surgical exploration as a "TN".
Statistical analysisQuality Assessment of Diagnostic Accuracy Studies-2 (QuadAS-2) was used to evaluate the literature quality. Statistical analysis was performed using RevMan 5.3 (Cochrane Collaboration) and Stata/SE 12.0. A random-effects model was used for the results. I2 value was used to evaluate the degree of heterogeneity. All statistical tests were two-sided, and p < 0.05 was considered statistically significant. Sensitivity analysis was used to determine the source of heterogeneity. Begg's test was used to assess publication bias.
ResultsLiterature search and study selectionA total of 527 studies were initially identified using the literature search criteria. After screening for duplicates, 233 studies were excluded, while 263 studies were excluded after screening the title and abstract. Thereafter, 31 studies were selected for full-text evaluation of eligibility. Based on the study selection criteria, 12 studies were excluded. Finally, 19 studies (one prospective and 18 retrospective studies) were included. The flowchart is shown in Figure 1.
Characteristics of the included studies and quality assessments
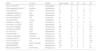
The characteristics and quality assessments of the selected studies are shown in Table 1.12,15-32 A total of 1336 patients were included in the studies.
Characteristics of the studies included in the meta-analysis.
| Study | Country | Design | Total number | TP | FP | FN | TN |
|---|---|---|---|---|---|---|---|
| Rho J H (2013) 15 | Korea | retrospective | 12 | 11 | 0 | 1 | 0 |
| Rerksuppaphol S(2004)16 | Australia | retrospective | 9 | 7 | 0 | 2 | 0 |
| Chen Q(2018)17 | China | retrospective | 78 | 55 | 0 | 23 | 0 |
| Papparella A(2014) 18 | Italy | retrospective | 19 | 11 | 1 | 6 | 1 |
| Shalaby RY(2005)19 | Egypt | retrospective | 7 | 3 | 1 | 2 | 1 |
| Al Janabi M(2014)20 | UK | prospective | 61 | 32 | 18 | 6 | 5 |
| Sancar (2015)21 | Turkey | retrospective | 8 | 4 | 2 | 1 | 1 |
| Swaniker F (1999)12 | USA | retrospective | 43 | 12 | 0 | 8 | 23 |
| Leonidas J C(1974)22 | USA | retrospective | 13 | 3 | 0 | 1 | 9 |
| Cooney D R(1982)23 | USA | retrospective | 266 | 12 | 14 | 2 | 238 |
| Gelfand M J(1978)24 | USA | retrospective | 55 | 7 | 2 | 2 | 44 |
| Ho JE(1975)25 | USA | retrospective | 20 | 3 | 0 | 0 | 17 |
| Fries M(1984) 26 | SWEDEN | retrospective | 22 | 9 | 0 | 3 | 10 |
| Poulsen KA(2000)27 | Denmark | retrospective | 55 | 3 | 1 | 2 | 49 |
| Kong MS(1994) 28 | Taiwan(China) | retrospective | 101 | 39 | 2 | 8 | 52 |
| Sinha CK(2013) 29 | UK | retrospective | 183 | 17 | 5 | 1 | 160 |
| Dolezal J(2008)30 | Czech Republic | retrospective | 80 | 3 | 0 | 0 | 77 |
| Mittal BR(2008)31 | India | retrospective | 105 | 16 | 3 | 0 | 6 |
| McCulley S(1996)32 | South Africa | retrospective | 77 | 4 | 6 | 2 | 65 |
The results of the quality assessment are shown in Figure 2. The overall quality of the 19 articles was relatively high. Ten studies had both a low risk of bias and low concerns regarding applicability. Five of the included studies had high risks.
Combination of effect size
The weights of the studies of Rho JH (2013), Rerksuppaphol S (2004), and Chen Q (2018) were zero, indicating no significance of the research results, so they were excluded. A random-effects model was used due to significant heterogeneity. At last, the effect sizes of sensitivity, specificity, and summary receiver operating characteristic (SROC) were combined to conduct a meta-analysis of 16 studies, including 1115 patients. The combined sensitivity and specificity were 0.80 [Confidence Interval (95% CI, 0.73-0.86) and 0.95 (95% CI, 0.86-0.98)], respectively (Figure 3). The area under the curve (AUC) was 0.88 (95% CI, 0.85-0.90) (Figure 4).
Heterogeneity test and subgroup after sensitivity analysis

The heterogeneity test revealed I2 = 91.3%, p = 0.000, which indicated significant heterogeneity. Subgroup analysis was conducted according to the sensitivity analysis (Figure 5).
Publication bias
A funnel plot was used to determine the publication bias (Figure 6). The funnel plot was symmetric, and Begg's test was not significant (p = 0.053), indicating no publication bias.
Discussion
MD mostly occurs in children under 15 years of age.3 However, the age of the children was not clearly stated in the original literature included, so this meta-analysis could not be conducted by age groups. Some patients experience severe bleeding, which can be life-threatening. In recent years, the Tc-99m scan is the main method for clinical diagnosis of MD, and there are some new studies about the Tc-99m scan. So, the authors conducted a systematic review and meta-analysis of all published articles, to assess the sensitivity and specificity of the Tc-99m scan.
After screening the published studies based on selection criteria, the authors included 19 studies. Three of these studies, Rho JH's study in 2013,15 Rerksuppaphol's study in 200416 and Chen Q's study in 2018,17 were excluded from the analysis because of their zero weights.
Finally, only 16 studies were included. Overall pooled diagnostic indices were as follows: sensitivity and specificity were 0.80 [Confidence Interval (95% CI, 0.73-0.86) and 0.95 (95% CI, 0.86-0.98)], respectively, indicating that most of them can be diagnosed in this way, and once diagnosed, they are confirmed.
However, the sensitivity of our study was much lower than the sensitivity of 92.1% (95% CI, 90.2-93.8) shown by Hosseinnezhad et al.,33 perhaps because the authors included some new articles, which added to the differences between groups. Another reason may be the limitations of the Tc-99m scan itself, which has clinical significance only if patients have obvious clinical symptoms, which may have also resulted in the very high specificity of 0.95 (95% CI, 0.86-0.98) in our study.
The ideal timing of the scan remains controversial. Some studies reported that the scan should be performed when the child is not actively bleeding to prevent rapid dilution of the radioisotope.34 However, other studies suggested that the scan should not be performed when there is no history of rectal bleeding. Hence, the timing of the scan and the method of capturing images are important.24,33,35,36
The sensitivity of the Tc-99m scan is affected by many factors, which is not only significantly related to the detection time in children (whether or not during active bleeding) but also closely related to the use of some drugs, such as H2 antagonists, 5-glutathione and glucagon, which can improve the accuracy of ectopic gastric mucosa detection and therefore affect the accuracy of diagnosis.34,37 For example, the use of H2 antagonists is particularly useful if there are insufficient gastric mucosal masses in the diverticulum or if the intradural imaging activity is diluted due to severe bleeding or excessive intestinal secretion, potentially leading to false negative scans. H2 antagonists such as ranitidine and cimetidine have been shown to improve scanning sensitivity by delaying the release of Tc-99m scan pertechnetate dye from mucosa and parietal cells.36
High heterogeneity was observed in our study. Hence, sensitivity analysis was performed on each data, and then subgroup analysis was performed on the results obtained from the sensitivity analysis. There was no statistically significant publication bias (Begg's test p = 0.053) in our study. This result strongly demonstrates the reliability of our results.
The high heterogeneity was related to each study, including sample size, study design, and the number of included cases. Therefore, more multi-centric prospective randomized controlled studies are needed in the future to demonstrate the clinical effects of the Tc-99m scan. Another possible factor leading to high heterogeneity in our study was the different demographics and characteristics.
The present study overcame many shortcomings of the previous meta-analyses. The authors verified our literature search results and study selection criteria. However, there were several limitations in this study. First, most of the included studies were retrospective. Therefore, these studies are not as representative as prospective randomized controlled studies. Second, the included studies and sample size were limited. Third, there was considerable heterogeneity between studies.
ConclusionTc-99m scan has important diagnostic significance in the clinic. However, given the relatively moderate sensitivity, which is always influenced by some factors, multiple methods should be used to actively diagnose the disease in clinical practice to avoid serious complications.





