

to describe the secular trends in overweight among preschool children in the years 1989, 1996, and 2006, and to identify risk factors associated with this condition in 2006.
Methodsanthropometric data from three surveys (1989, 1996, and 2006) with a representative sample of the population were analyzed. Overweight was defined as the weight-for-height Z-score. The multivariable models of overweight association with risk factors were generated by Poisson regression, and the estimates were shown as prevalence ratios with their respective 95% confidence intervals (PR [95% CI]).
Resultsthroughout the 17-year period studied, the relative prevalence of overweight in preschoolers increased by 160% in Brazil, representing an increase of 9.4% per year. Based on data from the National Survey on Demography and Health of Women and Children - 2006/07, four multivariable models were created (macro-environmental, maternal, individual, and final model) assuming hierarchy among the risk factors. In the final model, only the following remained associated with overweight: regions South/Southeast (1.55 [1.17 to 2.06]), middle-class (1.35 [1.02 to 1.77]), maternal obesity (1.66 [1.22 to 2.27]), birth weight ≥ 3.9kg (1.87 [1.31 to 2.67]), and being an only child or having only one sibling (1.81 [1.31 to 2.49]).
Conclusionthe prevalence of overweight among preschool children in Brazil has increased dramatically over the past 17 years, and it was higher in the 1996-2006 period. Future strategies for prevention and control of overweight in public health should focus or intensify actions in communities that are characterized by the presence of the risks identified in the present study.
descrever a tendência secular do excesso de peso (EP) entre pré-escolares nos anos de 1989, 1996 e 2006 e identificar os fatores de risco associados a esta condição em 2006.
Métodosanálise dos dados de três inquéritos antropométricos (1989, 1996 e 2006) com amostra representativa da população brasileira. O EP foi definido como o escore-Z de peso-para-altura >+2. Os modelos multivariáveis de associação do EP com os fatores de risco foram gerados por meio da regressão de Poisson e as estimativas apresentadas como razão de prevalência com seus respectivos intervalos de confiança de 95% (RP [IC 95%]).
Resultadosno período de 17 anos estudado, a prevalência relativa do EP em pré-escolares aumentou em 160% no Brasil, representando incremento de 9,4% ao ano. A partir dos dados da Pesquisa Nacional de Demografia e Saúde da Mulher e da Criança-2006/07 criamos quatro modelos multivariáveis (macroambiental, materno, individual, modelo final) assumindo hierarquia entre os fatores de risco. No modelo final, permaneceram como fatores associados ao EP: as macrorregiões Sul/Sudeste (1,55 [1,17-2,06]), a classe média (1,35 [1,02-1,77]), a obesidade materna (1,66 [1,22-2,27]), o peso ao nascer > 3,9kg (1,87 [1,31-2,67]) e ser filho único ou possuir um irmão (1,81 [1,31-2,49]).
Conclusãoa prevalência de EP entre pré-escolares no Brasil aumentou drasticamente nos últimos 17 anos, sendo mais intenso no intervalo de 1996-2006. Futuras estratégias de prevenção e controle do EP em saúde pública devem considerar em seu escopo, ou intensificar suas ações, nas coletividades que se caracterizem pela presença dos riscos identificados neste trabalho.
In addition to the psychosocial, orthopedic, respiratory, and metabolic comorbidities caused by childhood obesity,1,2 the body of evidence that correlates it to adverse events in adulthood has become increasingly solid. Juonala et al.3 analyzed four cohorts, and verified that individuals at higher risk for type II diabetes, hypertension, hypercholesterolemia, hypertriglyceridemia, and increased intima-media thickness of the carotid artery had been overweight children who remained overweight until adulthood, followed by normal weight children who became obese adults. Recognizing that such outcomes are responsible for a decrease in the productive capacity and early death, it is essential to implement effective overweight prevention and control actions in children in different contexts.4–7
However, to facilitate the planning of these actions, it is crucial that the problem is adequately assessed by anthropometric surveys with national representativeness. These surveys allow for the identification of the health and nutrition profiles of the population and the distribution of their risk factors, making comparisons at national and international levels possible, either cross-sectional or over time, describing the trends of the studied indicators.8–10 In this context, using data from the National Health and Nutrition Survey (Pesquisa Nacional de Saúde e Nutrição - PNSN-1989) and the National Woman and Child Demographic and Health Survey (Pesquisas Nacionais de Demografia e Saúde da Criança e da Mulher - PNDS-1996 and 2006/07), that it was sought to describe the secular trend of overweight exclusively among Brazilian preschool children, identifying risk factors, at different hierarchical levels, associated with this condition in the 2006/07 survey.
MethodsStudy designThis study used public domain data11 from the third PNDS-2006/07 survey, conducted between November of 2006 and May of 2007, and was approved by the Research Ethics Committee of the Universidade Federal de São Paulo (protocol number 1524/10).
The PNDS-2006/07 was a nationally representative cross-sectional survey, conducted by complex probability sampling in two stages (census sectors and households). The research environment consisted of private homes, including slums.12
The data related to the prevalence of overweight in preschoolers in 1989 and 1996 were obtained from the work of Taddei et al.13 The methodologies employed in the PNSN-1989 and the PNDSs of 1996 and 2006/07 are similar, which allows for the analysis of the temporal evolution of overweight in preschoolers.
Eligibility criteria and selectionHouseholds were considered eligible if they had at least one woman of childbearing age (18-45 years). For those who were mothers, a questionnaire was applied to collect specific data for all children younger than 60 months of age. For the purpose of this research, only the preschoolers (24-59 months) living with their mothers in the same household were selected.
Studied variablesIn the analysis of secular trends of overweight, prevalence rates were estimated based on the anthropometric index weight-for-height Z-score (WHZ) defined as WHZ > +2 SD, a cutoff that includes overweight and obese children. The 1989 and 1996 surveys adopted the growth chart of the National Center for Health Statistics (NCHS, 1979), while for the 2006/07 period we used the reference from the World Health Organization (WHO) 2006.14
Anthropometric measurements were performed by pairs of trained interviewers using an electronic scale (precision of 100g) and a portable stadiometer (precision of 1mm). More details are available in the report “Methodological Aspects of PNDS-2006/07”.12
The estimates of this study are shown using dichotomous variables for: gender; area of residence (urban/rural); region (South and Southeast/North, Northeast, and Midwest); maternal age at the child's birth (< 21 years); maternal level of education (< seven years); maternal obesity (BMI > 30kg/m2); economic class (C1-C2/A1-B2, D, and E); birth weight (≥ 3.9kg, cutoff set at the 90th percentile of the sample); number of siblings (≤ one sibling); number of TV sets in the home (> one TV set); duration of exclusive breastfeeding (EBF) (< 150 days); and weekly consumption of soft drinks or artificial juices (≥ four days/week), fried foods (≥ four days/week), and soda or artificial juices and fried foods (≥ four days/week).
Regions were dichotomized in order to contrast the Brazilian development poles; the South and Southeast regions are the most developed. The socioeconomic class was obtained from the Economic Classification Criteria of Brazil (Critério de Classificação Econômica Brasil - CCEB). This is a validated scale that classifies the economic situation of the family in eight categories; each category represents an average household income. The category used as a reference in the present estimates (C1-C2) represents the Brazilian middle class in 2006, with a mean monthly household income income of R$ 849 to R$1,288.15
Food consumption was obtained by trained interviewers using the qualitative food frequency questionnaire (FFQ) found in the “Woman's Questionnaire”, having the following options as answers regarding food: “did not eat”, “once”, “two to three times”, “four to six times”, “every day in the week”, and “does not know”.11
Data analysisThe secular trend in the prevalence of overweight in preschool children was shown for the country and geographical regions, according to the relative percentage variation (Δ% = {[Prevalence t2–Prevalence t1]/Prevalence t1}*100) that occurred between periods 1989-1996, 1996-2006, and 1989-2006, and the annual variation in the 17 years encompassed by the surveys.
Data analysis was performed in Stata 12/IC software (StataCorp LP - College Station, TX, USA). In order to consider the complex sampling, the svy command was used in all analyses. However, the sample weight was applied only in the descriptive and prevalence analyses, disregarding the inferential analyses. Considering that the data are based on a population sample, the estimates generated in the bivariate and multivariate analyses were reported as prevalence ratio (PR) by Poisson regression.16,17
Associations between body weight in preschoolers and potential risk factors were studied in three hierarchical levels, analyzed by four multivariable models. The first model considered the macro-environmental variables; the second, the maternal variables; and the third, the individual variables adjusted for the duration of EBF (< 150 days) and gender. Finally, a fourth model was generated in which the three levels were grouped, maintaining the adjustment made in model 3.
Variables eligible for the multivariate analysis were those with p < 0.20 in the bivariate analyses, and only those with p < 0.05 remained in the models. In addition to the statistical criteria used in variable selection for the model, the recent findings on risk factors for overweight in children that can be identified in childhood were considered.18 All summary measures are shown with their respective 95% confidence intervals (95% CI).
ResultsSecular trends in overweight: 1989, 1996, and 2006In databases concerning the surveys of 1989, 1996, and 2006 there were, respectively, 4,143, 2,388 and 2,635 children aged 24 to 59 months with complete anthropometric data.
The prevalence of overweight in preschool children in Brazil was 3% (95% CI: 2.2 to 3.9) in 1989, remaining at 3.4% (95% CI: 2.5 to 4.3) in 1996, with a 129% increase (7.8% [95% CI: 6.3 to 9.5]) in 2006. Although the South and North regions presented a small reduction in the prevalence of overweight in the period of 1989-1996, there is a pattern of increased prevalence of overweight in these regions among preschoolers over the last 17 years. The positive variation that occurred in this period represented an increase of 9.4% per year in the prevalence of overweight (Fig. 1).
 estimates of overweight in Brazilian preschool children, with their respective 95% confidence intervals - National Health and Nutrition Survey 1989 and National Woman and Child Demographic and Health Survey - 1996 and 2006/07. *p < 0.05. aAnnual percentage increment of overweight in preschool children.")
Secular trends of national and regional prevalence (%) estimates of overweight in Brazilian preschool children, with their respective 95% confidence intervals - National Health and Nutrition Survey 1989 and National Woman and Child Demographic and Health Survey - 1996 and 2006/07.
*p < 0.05.
aAnnual percentage increment of overweight in preschool children.
This increase in the prevalence of overweight is even more significant in the Southeast and Northeast, increasing from 3.4% (95% CI: 1.7 to 5.2) in 1989 to 7.8% (95% CI: 6.3 to 9.5) in 2006, and from 1.6% (95% CI: 0.8-2.3) in 1989 to 7.2% (95% CI: 5.0 to 10.4) in 2006, respectively. The South appears in all three surveys (1989: 5.4% [95% CI: 3.5 to 7.4]; 1996: 4.1% [95% CI: 1.4 to 6.8]; 2006: 9% [95% CI: 6.2 to 13.0]) as the region with the highest prevalence of overweight among preschoolers, even considering the decrease that occurred between 1989 and 1996. From 1996 onwards, the prevalence in the Southeast region showed a similar evolution to that of the South region.
Due to the slight reduction in the prevalence of overweight that occurred in the North and South in the first period, the variations related to the surveys of 1989 and 2006 were the lowest: 2.5% and 3.9%, respectively. The magnitude of this annual variation increased in the Midwest (6.6%) and even more in the Southeast (9.5%), but the phenomenon that occurred in the Northeast surpasses all other regions, with a recorded annual growth of 20.6%.
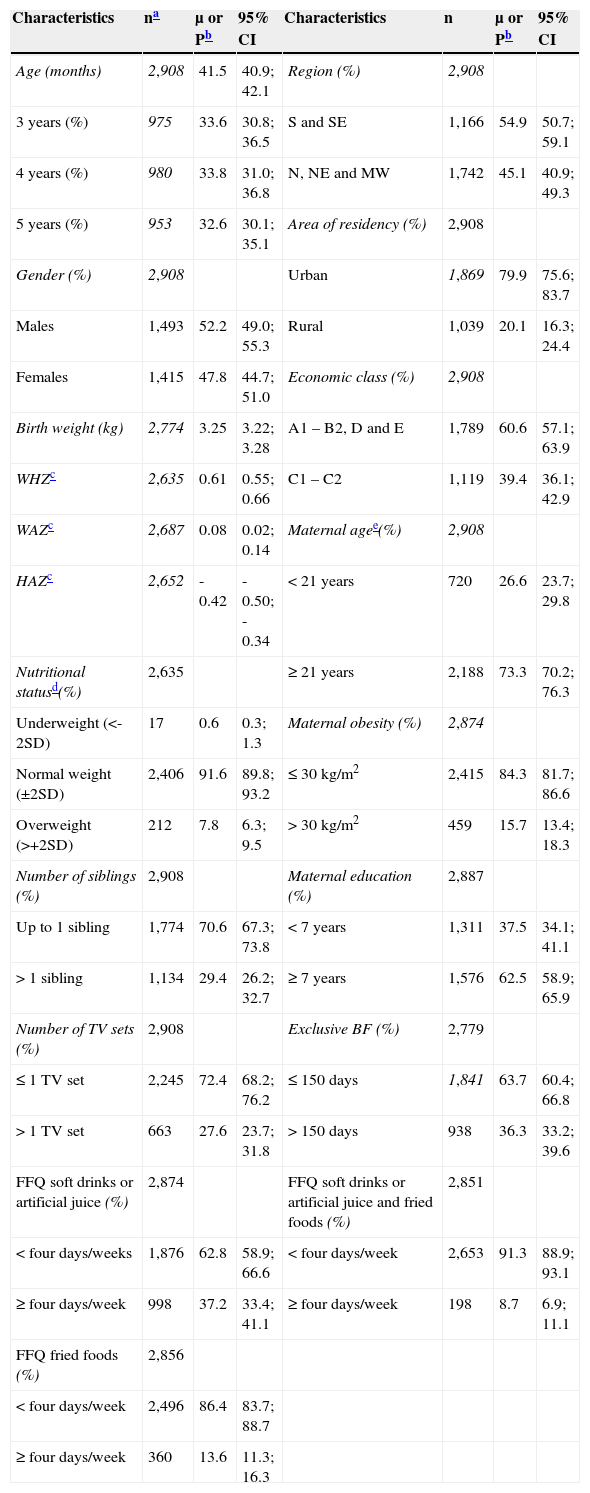
Prevalence and factors associated with overweight in 2006Of the 6,011 children younger than 5 years whose data were available in the PNDS-2006/07 database, 2,908 were preschoolers living in the same house as their mothers. Those with biologically plausible anthropometric data were considered for the analyses.19 The characteristics of the 2,635 analyzed preschoolers (90.6%), after exclusions due to anthropometric criteria, are described in Table 1. There was no statistically significant difference in age, gender, area of residence, region, and socioeconomic class among the children studied and those without anthropometric data.
Characteristics of Brazilian preschoolers – National Woman and Child Demographic and Health Survey – 2006/07.
| Characteristics | na | μ or Pb | 95% CI | Characteristics | n | μ or Pb | 95% CI |
|---|---|---|---|---|---|---|---|
| Age (months) | 2,908 | 41.5 | 40.9; 42.1 | Region (%) | 2,908 | ||
| 3 years (%) | 975 | 33.6 | 30.8; 36.5 | S and SE | 1,166 | 54.9 | 50.7; 59.1 |
| 4 years (%) | 980 | 33.8 | 31.0; 36.8 | N, NE and MW | 1,742 | 45.1 | 40.9; 49.3 |
| 5 years (%) | 953 | 32.6 | 30.1; 35.1 | Area of residency (%) | 2,908 | ||
| Gender (%) | 2,908 | Urban | 1,869 | 79.9 | 75.6; 83.7 | ||
| Males | 1,493 | 52.2 | 49.0; 55.3 | Rural | 1,039 | 20.1 | 16.3; 24.4 |
| Females | 1,415 | 47.8 | 44.7; 51.0 | Economic class (%) | 2,908 | ||
| Birth weight (kg) | 2,774 | 3.25 | 3.22; 3.28 | A1 – B2, D and E | 1,789 | 60.6 | 57.1; 63.9 |
| WHZc | 2,635 | 0.61 | 0.55; 0.66 | C1 – C2 | 1,119 | 39.4 | 36.1; 42.9 |
| WAZc | 2,687 | 0.08 | 0.02; 0.14 | Maternal agee(%) | 2,908 | ||
| HAZc | 2,652 | -0.42 | -0.50; -0.34 | < 21 years | 720 | 26.6 | 23.7; 29.8 |
| Nutritional statusd(%) | 2,635 | ≥ 21 years | 2,188 | 73.3 | 70.2; 76.3 | ||
| Underweight (<-2SD) | 17 | 0.6 | 0.3; 1.3 | Maternal obesity (%) | 2,874 | ||
| Normal weight (±2SD) | 2,406 | 91.6 | 89.8; 93.2 | ≤ 30 kg/m2 | 2,415 | 84.3 | 81.7; 86.6 |
| Overweight (>+2SD) | 212 | 7.8 | 6.3; 9.5 | > 30 kg/m2 | 459 | 15.7 | 13.4; 18.3 |
| Number of siblings (%) | 2,908 | Maternal education (%) | 2,887 | ||||
| Up to 1 sibling | 1,774 | 70.6 | 67.3; 73.8 | < 7 years | 1,311 | 37.5 | 34.1; 41.1 |
| > 1 sibling | 1,134 | 29.4 | 26.2; 32.7 | ≥ 7 years | 1,576 | 62.5 | 58.9; 65.9 |
| Number of TV sets (%) | 2,908 | Exclusive BF (%) | 2,779 | ||||
| ≤ 1 TV set | 2,245 | 72.4 | 68.2; 76.2 | ≤ 150 days | 1,841 | 63.7 | 60.4; 66.8 |
| > 1 TV set | 663 | 27.6 | 23.7; 31.8 | > 150 days | 938 | 36.3 | 33.2; 39.6 |
| FFQ soft drinks or artificial juice (%) | 2,874 | FFQ soft drinks or artificial juice and fried foods (%) | 2,851 | ||||
| < four days/weeks | 1,876 | 62.8 | 58.9; 66.6 | < four days/week | 2,653 | 91.3 | 88.9; 93.1 |
| ≥ four days/week | 998 | 37.2 | 33.4; 41.1 | ≥ four days/week | 198 | 8.7 | 6.9; 11.1 |
| FFQ fried foods (%) | 2,856 | ||||||
| < four days/week | 2,496 | 86.4 | 83.7; 88.7 | ||||
| ≥ four days/week | 360 | 13.6 | 11.3; 16.3 |
BF, breastfeeding; CI, confidence interval; FFQ, Food Frequency Questionnaire; H/A, height-for-age; MW, Midwest; N, north; NE, Northeast; P, prevalence; S, South; SD, standard deviation; SE, Southeast; W/H, weight-for-height; W/A, weight-for-age; μ, mean; WHZ, weight-for-height Z-score.
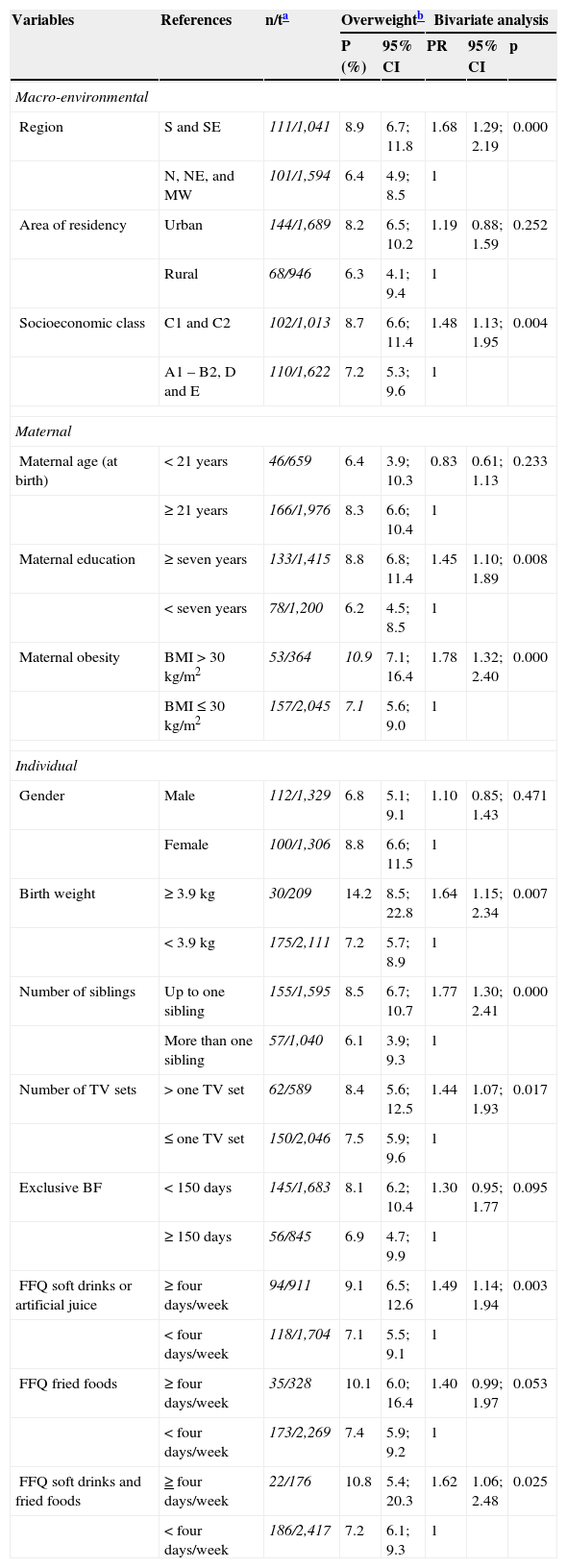
Table 2 presents the prevalence and bivariate analyses of factors associated with overweight in preschoolers in 2006. Regarding the macro-environmental variables, higher prevalence of overweight was observed among children residing in the South and Southeast regions of the country (8.9%) and belonging to economic class C1-C2 (8.7%). These factors had a PR of 1.68 and 1.48, respectively (p < 0.005)
Prevalence of overweight among Brazilian preschool children and bivariate analysis, according to the studied exposure variables - National Woman and Child Demographic and Health Survey – 2006/07.
| Variables | References | n/ta | Overweightb | Bivariate analysis | |||
|---|---|---|---|---|---|---|---|
| P (%) | 95% CI | PR | 95% CI | p | |||
| Macro-environmental | |||||||
| Region | S and SE | 111/1,041 | 8.9 | 6.7; 11.8 | 1.68 | 1.29; 2.19 | 0.000 |
| N, NE, and MW | 101/1,594 | 6.4 | 4.9; 8.5 | 1 | |||
| Area of residency | Urban | 144/1,689 | 8.2 | 6.5; 10.2 | 1.19 | 0.88; 1.59 | 0.252 |
| Rural | 68/946 | 6.3 | 4.1; 9.4 | 1 | |||
| Socioeconomic class | C1 and C2 | 102/1,013 | 8.7 | 6.6; 11.4 | 1.48 | 1.13; 1.95 | 0.004 |
| A1 – B2, D and E | 110/1,622 | 7.2 | 5.3; 9.6 | 1 | |||
| Maternal | |||||||
| Maternal age (at birth) | < 21 years | 46/659 | 6.4 | 3.9; 10.3 | 0.83 | 0.61; 1.13 | 0.233 |
| ≥ 21 years | 166/1,976 | 8.3 | 6.6; 10.4 | 1 | |||
| Maternal education | ≥ seven years | 133/1,415 | 8.8 | 6.8; 11.4 | 1.45 | 1.10; 1.89 | 0.008 |
| < seven years | 78/1,200 | 6.2 | 4.5; 8.5 | 1 | |||
| Maternal obesity | BMI > 30 kg/m2 | 53/364 | 10.9 | 7.1; 16.4 | 1.78 | 1.32; 2.40 | 0.000 |
| BMI ≤ 30 kg/m2 | 157/2,045 | 7.1 | 5.6; 9.0 | 1 | |||
| Individual | |||||||
| Gender | Male | 112/1,329 | 6.8 | 5.1; 9.1 | 1.10 | 0.85; 1.43 | 0.471 |
| Female | 100/1,306 | 8.8 | 6.6; 11.5 | 1 | |||
| Birth weight | ≥ 3.9 kg | 30/209 | 14.2 | 8.5; 22.8 | 1.64 | 1.15; 2.34 | 0.007 |
| < 3.9 kg | 175/2,111 | 7.2 | 5.7; 8.9 | 1 | |||
| Number of siblings | Up to one sibling | 155/1,595 | 8.5 | 6.7; 10.7 | 1.77 | 1.30; 2.41 | 0.000 |
| More than one sibling | 57/1,040 | 6.1 | 3.9; 9.3 | 1 | |||
| Number of TV sets | > one TV set | 62/589 | 8.4 | 5.6; 12.5 | 1.44 | 1.07; 1.93 | 0.017 |
| ≤ one TV set | 150/2,046 | 7.5 | 5.9; 9.6 | 1 | |||
| Exclusive BF | < 150 days | 145/1,683 | 8.1 | 6.2; 10.4 | 1.30 | 0.95; 1.77 | 0.095 |
| ≥ 150 days | 56/845 | 6.9 | 4.7; 9.9 | 1 | |||
| FFQ soft drinks or artificial juice | ≥ four days/week | 94/911 | 9.1 | 6.5; 12.6 | 1.49 | 1.14; 1.94 | 0.003 |
| < four days/week | 118/1,704 | 7.1 | 5.5; 9.1 | 1 | |||
| FFQ fried foods | ≥ four days/week | 35/328 | 10.1 | 6.0; 16.4 | 1.40 | 0.99; 1.97 | 0.053 |
| < four days/week | 173/2,269 | 7.4 | 5.9; 9.2 | 1 | |||
| FFQ soft drinks and fried foods | ≥ four days/week | 22/176 | 10.8 | 5.4; 20.3 | 1.62 | 1.06; 2.48 | 0.025 |
| < four days/week | 186/2,417 | 7.2 | 6.1; 9.3 | 1 | |||
BF, breastfeeding; BMI, body mass index; CI, confidence interval; FFQ, Food Frequency Questionnaire; MW, Midwest; N, north; NE, Northeast; P, prevalence; PR, prevalence ratio; S, South; SE, Southeast.
Regarding maternal variables, the children of obese mothers had a prevalence of overweight of 10.9%. This prevalence corresponded to a 78% higher frequency of overweight (p = 0.000) among preschoolers that were children of obese mothers when compared to those whose mothers had a BMI ≤ 30kg/m2. In addition, maternal education ≥ seven years was also positively associated with their children's overweight (PR 1.45; p < 0.01).
Children born weighing ≥ 3.9kg showed a 14.2% prevalence of overweight at the time of the survey, representing a frequency of overweight 64% higher than those children whose birth weight was < 3.9kg (p < 0.01). Similar prevalence and PR were observed among children who consumed soft drinks or artificial juices or fried foods on at least four days per week. However, when considering the preschoolers who consumed soft drinks or sugary drinks and fried foods on four or more days per week, a synergistic association was identified with the increased prevalence and strength of association with overweight, which, however, was not maintained in the multivariate analysis.
Being an only child or having only one sibling, when compared to those children with two or more siblings, showed a PR of 1.77 (p = 0.000). The number of TV sets in the home was also associated with higher prevalence of overweight, identifying as a risk group the homes where there were two or more TV sets (PR 1.44, p < 0.05). When comparing children who received EBF for a period < 150 versus ≥ 150 days, the former had a 30% higher PR (p < 0.10).
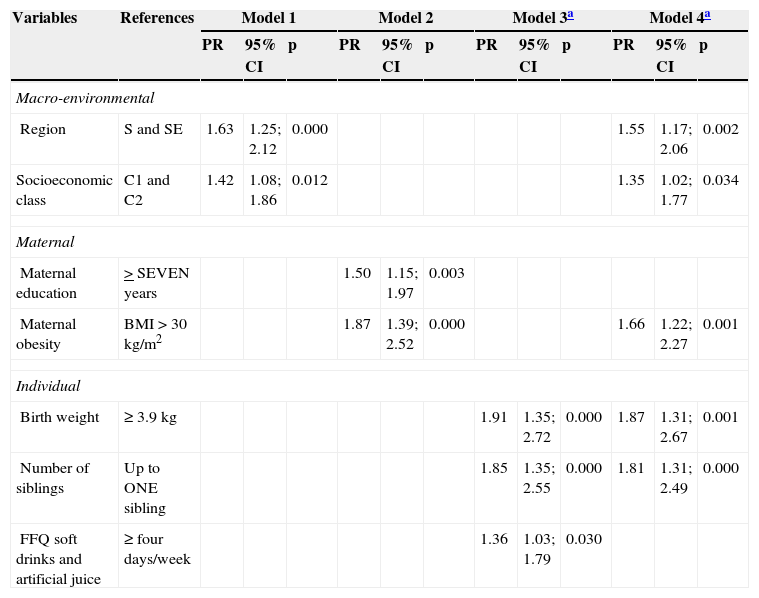
In the analysis according to the hierarchical level between risk factor and overweight (Table 3), it was observed that the following remained in the macro-environmental multivariable model (model 1): socioeconomic class C (PR 1.42 [95% CI: 1.08 to 1.86]) and regions S and SE (PR 1.63 [95% CI: 1.25 to 2.12]); regarding model 2, maternal education ≥ seven years (PR 1.50 [95% CI: 1.15 to 1.97]) and obesity (PR 1.87 [95%CI: 1.39 to 2.52]). Among the seven individual variables chosen for model 3, three remained in the multivariate model of individual factors: birth weight ≥ 3.9kg (PR 1.91 [95% CI: 1.35 to 2.72]), being an only child or to having only one sibling (PR 1.85 [95% CI: 1.35 to 2.55]), and consumption of soft drinks or artificial juices four or more times a week (PR 1.36 [95% CI: 1.03 to 1.79]).
Multivariate models for overweight among Brazilian preschool children according to hierarchical levels of studied exposure variables - National Woman and Child Demographic and Health Survey – 2006/07.
| Variables | References | Model 1 | Model 2 | Model 3a | Model 4a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PR | 95% CI | p | PR | 95% CI | p | PR | 95% CI | p | PR | 95% CI | p | ||
| Macro-environmental | |||||||||||||
| Region | S and SE | 1.63 | 1.25; 2.12 | 0.000 | 1.55 | 1.17; 2.06 | 0.002 | ||||||
| Socioeconomic class | C1 and C2 | 1.42 | 1.08; 1.86 | 0.012 | 1.35 | 1.02; 1.77 | 0.034 | ||||||
| Maternal | |||||||||||||
| Maternal education | > SEVEN years | 1.50 | 1.15; 1.97 | 0.003 | |||||||||
| Maternal obesity | BMI > 30 kg/m2 | 1.87 | 1.39; 2.52 | 0.000 | 1.66 | 1.22; 2.27 | 0.001 | ||||||
| Individual | |||||||||||||
| Birth weight | ≥ 3.9kg | 1.91 | 1.35; 2.72 | 0.000 | 1.87 | 1.31; 2.67 | 0.001 | ||||||
| Number of siblings | Up to ONE sibling | 1.85 | 1.35; 2.55 | 0.000 | 1.81 | 1.31; 2.49 | 0.000 | ||||||
| FFQ soft drinks and artificial juice | ≥ four days/week | 1.36 | 1.03; 1.79 | 0.030 | |||||||||
n model 1 = 2,635; n model 2 = 2,599; n model 3 = 2,405; n model 4 = 2,407.
BMI, body mass index; CI, confidence interval; FFQ, Food Frequency Questionnaire; PR, prevalence ratio; S, South; SE, Southeast.
When the three previous models were grouped (model 4), maternal education and the consumption of soft drinks or artificial juices did not maintain the association. However, macro-regions S and SE, economic class C, maternal obesity, birth weight > 3.9kg, and number of siblings ≤ one were independently associated with overweight in Brazilian preschoolers in PNDS 2006/07.
DiscussionA previous publication showed that the increased prevalence of overweight among children younger than five years of age that occurred between 1989 and 2006 was due to overweight increase among preschoolers, as the prevalence among infants decreased.20 In the present study, the secular trend of overweight was analyzed exclusively among Brazilian preschool children in the period of 1989-2006, identifying the social and economic factors associated with overweight in preschool children assessed in the 2006/07 survey.
In the 17 years preceding the PNDS-2006/07, there was a great increase in the prevalence of overweight and obesity among children aged 24 to 59 months of age. The fact that this observation was made by three methodologically comparable population surveys reinforces that the statistically significant differences found between the prevalence of overweight in the three periods represents a temporal process that reflects marked changes in living and nutrition conditions among Brazilian preschool children.
As described before, Taddei et al.13 used as a reference the growth curve from NCHS-1979, which was adopted by the Ministry of Health for nutritional surveillance of the population until the WHO curves were released in 2006, which were used in the present analyses. As these curves have a high degree of agreement with the WHZ ratio in preschoolers, any observed differences in prevalence estimates of overweight in the Brazilian pediatric population do not represent sufficient magnitude to alter the conclusions obtained from the evaluation of temporal trends.21,22 Such comparison would not be appropriate if the overweight among preschoolers had been evaluated by the weight-for-age Z-scores, where the differences are more marked.22
Due to access difficulties, interviews and measurements were not conducted in the rural Northern region in 1989 and 1996 surveys. In these same surveys, when comparing the sample sizes of the Southeast and Northeast regions to the South, Midwest and North, it is observed that the sample size is also higher in the first two.13 Evidently, the sample weighting process aims to minimize such differences among population groups; however, when comparing the size of the confidence intervals, the smaller sample size was attributed to the lack of statistical significance in the differences between the estimates of overweight and obesity prevalence, as the magnitude of the effect increases by more than two-fold in the regions.
The increase in obesity among preschoolers was concomitant with the economic and political changes in Brazil during this period, such as the end of the military dictatorship, the transition to and consolidation of democracy, inflation control, and economic stabilization of the country. As in other parts of the world, such changes have made room for the private sector to redefine the lifestyle and dietary patterns of the population,23 generating consequences in the short and long term for the health and nutritional status of the population, especially among preschoolers, who do not have enough insight to make healthy food choices, and are influenced by advertising messages conveyed in different types of media, especially via television.24
From the individual's point of view, the maintenance of poor eating habits can be attributed to the fact that populations who underwent food deprivation and experienced high frequency of negative nutritional disorders tend to value overweight, without realizing that such a condition is deleterious to health.25 Additionally, the increased purchasing power of the population due to the period of economic stability,26 allowed the population, encouraged by the food industry, to increase the consumption of highly processed foods, high in simple sugars and saturated and trans-fats.23 These arguments are supported by the present results, as a higher frequency of preschoolers with overweight was observed in more developed Brazilian regions and among those belonging to the middle class.
The present results were also consistent with those in the literature regarding overweight at birth, maternal obesity, and excessive consumption of soft drinks or artificial juices as risk factors for overweight in preschool. A Chinese cohort, contemporary to the Brazilian survey of 2006, demonstrated that children born weighing > 4,000g are 3.06 (2.54 to 3.69) more likely to become overweight or obese between 3 and 6 years of age.27 Similarly, in a cohort from the United States of America, birth weight > 3.86kg increased the relative risk of overweight among children aged 4 and 5 years of age by 2.17 times (1.22 -3.87).28 In the same cohort, maternal obesity showed a risk of 6.27 (3.32 to 11.85) for childhood obesity. Reilly et al.29 found that maternal obesity increased the chance of being obese at age 7 by 4.66 times (3.28 to 6.64).
It is noteworthy that in the present analysis, overweight in preschool children was independently associated with the risk factors present in each of the three hierarchical levels. With the exception of maternal level of education and the consumption of soft drinks or artificial juices, all variables remained strongly associated with overweight in the final model, adjusted for gender and EBF. The models 3 and 4 for EBF were adjusted due to the increasing number of studies demonstrating its practice as protective against obesity; the cutoff of 150 days was based on a previous publication by the authors and the study by Griffiths et al.,30 who showed that children breastfed for less than four months showed a weight gain that was higher than those receiving EBF.
One possible hypothesis that could explain part of the decrease in overweight among infants, with a concomitant increase among preschoolers, would be that the increased length of EBF since the 1990s18,31 has protected infants from excessive weight gain, but the introduction of complementary foods and increased children's autonomy to make their food choices, in addition to unhealthy food environment at home determined by macro-environmental and maternal factors, have annulled the protective effect for overweight in preschoolers.
These factors present in early life have been consistently highlighted by well-designed prospective studies as predictors of overweight in later childhood, which in turn is a condition that tends to perpetuate itself until adulthood, generating ill individuals with lower productive capacity for society.3,7,18,29
ConclusionThe epidemic of overweight and obesity among preschool children in Brazil has increased dramatically over the past 17 years, and it was intensified in the second analyzed interval (1996-2006).
The risk analysis for overweight in preschoolers in 2006 identified that macro-regions South and Southeast, middle socioeconomic class, children of obese mothers or with birth weight ≥ 3.9kg, and having only one sibling or being an only child were factors independently associated with the risk of overweight.
Future strategies for overweight prevention and control in public health should consider communities that are characterized by the presence of these risk factors, as there is increasing evidence demonstrating the extent of the damage caused by overweight throughout life. From the clinical practice standpoint, the perception of these risks is simple and should be considered as an important aspect in the holistic care of the child's health.
FundingThe National Woman and Child Demographic and Health Survey – 2006/07 received financial support from the Brazilian Ministry of Health, and was conducted by Centro Brasileiro de Análises e Planejamento (CEBRAP). Author JS has a grant from the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), protocol No. 2011/17736-4. Author JT has a productivity grant from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silveira JA, Colugnati FA, Cocetti M, Taddei JA. Secular trends and factors associated with overweight among Brazilian preschool children: PNSN-1989, PNDS-1996, and 2006/07. J Pediatr (Rio J). 2014;90:258–66.




