




To investigate the psychometric properties of the short or multimodal treatment study version of the Swanson, Nolan, and Pelham, Version IV (SNAP-IV) scale, which measures attention-deficit/hyperactivity disorder and oppositional defiant disorder symptoms.
MethodsParticipants were 765 parents of children from 4 to 16 years old (641 non-attention-deficit/hyperactivity disorder and 124 attention-deficit/hyperactivity disorder children) from Belo Horizonte, Brazil, who reported sociodemographic characteristics and answered the SNAP-IV. Parents of the clinical sample also underwent the K-SADS-PL interview.
ResultsAge was significantly associated with SNAP-IV hyperactivity-impulsivity problems (r=−0.14), but not with inattention or oppositional defiant disorder. Sex was a significant influence on attention-deficit/hyperactivity disorder and oppositional defiant disorder severity (all p<0.001), with boys showing higher scores in the full sample, but not within the attention-deficit/hyperactivity disorder group. Exploratory and confirmatory factor analysis supports a three-factor structure of the SNAP-IV scale. Moderate-to-strong correlations were found between SNAP-IV and K-SADS-PL measures. All SNAP-IV scales showed very high internal consistency coefficients (all above 0.91). SNAP-IV inattention scores were the most predictive of attention-deficit/hyperactivity disorder diagnosis (AUC: 0.877 for the averaging rating method and the raw sum method, and 0.874 for the symptom presence/absence method).
ConclusionThe parent SNAP-IV showed good psychometric properties in a Brazilian school and clinical sample.
Investigar as propriedades psicométricas da versão curta ou MTA da escala Swanson, Nolan e Pelham, versão IV (SNAP-IV), que mede os sintomas do transtorno de déficit de atenção/hiperatividade e transtorno desafiador de oposição.
MétodosOs participantes incluíram 765 pais de crianças de 4 a 16 anos (641 crianças sem transtorno de déficit de atenção/hiperatividade e 124 com transtorno de déficit de atenção/hiperatividade) de Belo Horizonte, Brasil, que relataram características sociodemográficas e responderam ao SNAP-IV. Os pais da amostra clínica também foram submetidos à entrevista com K-SADS-PL.
ResultadosA idade foi significativamente associada aos problemas de hiperatividade-impulsividade no SNAP-IV (r=−0,14), mas não à desatenção ou aos transtornos desafiadores de oposição. O sexo foi uma influência significativa na gravidade do transtorno de déficit de atenção/hiperatividade e transtorno desafiador de oposição (todos os p<0,001), os meninos apresentaram escores mais altos na amostra completa, mas não no grupo de transtorno de déficit de atenção/hiperatividade. A análise fatorial exploratória e confirmatória apoia uma estrutura de três fatores da escala SNAP-IV. Foram encontradas correlações moderadas a fortes entre as medidas dos instrumentos SNAP-IV e K-SADS-PL. Todas as escalas do SNAP-IV mostraram coeficientes de consistência interna muito altos (todos acima de 0,91). Os escores de desatenção do SNAP-IV foram os mais preditivos do diagnóstico de transtorno de déficit de atenção/hiperatividade (AUC – área sob a curva ROC: 0,877 para o método de classificação da média e o método da soma bruta e 0,874 para o método de presença ou ausência de sintomas).
ConclusãoA avaliação do SNAP-IV pelos pais apresentou boas propriedades psicométricas em uma escola brasileira e amostra clínica.
Attention deficit/hyperactivity disorder (ADHD) figures among the most common (up to 8% of school-age children) and well-validated neurobehavioral conditions of childhood.1 ADHD is associated with enduring functional impairment, including academic and occupational impairment, accidental injuries, risky behavior, negative family and peer relations, and comorbid psychopathology.1,2 Individuals with ADHD are more likely to experience social disadvantages3 and, untreated, the condition places a substantial economic burden on society.3–5
ADHD, such as other prevalent forms of psychopathology, can be understood as a dimensional phenomenon.1,6–9 It is defined by developmentally extreme and impairing symptoms of inattention-disorganization and hyperactivity-impulsivity.10 Although the dichotomization of ADHD as a diagnosis (clinical vs. non-clinical) based on thresholds related to functional impairment may facilitate binary choices, it is done at the cost of decreased reliability.1,8 Even long-term treatment success and modality choice on ADHD is dependent on accounting for symptom severity, with early preventive identification and intervention (i.e., before impairment consolidation) more likely to yield the best outcomes.10–12 Therefore, from an evidence-based perspective and for pragmatic reasons, the categorical ADHD diagnosis must go along with documentation of ADHD symptom severity.
The short (26-item version) or Multimodal Treatment Study for ADHD (MTA) version of the Swanson, Nolan, and Pelham, Version IV (SNAP-IV) is one of the most used instruments for measuring ADHD symptom severity.13,14 MTA-SNAP-IV directly assess the core symptoms of ADHD and oppositional defiant disorder (ODD)14–17 as described in the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., which are virtually the same as for ADHD and ODD symptoms in the last DSM edition, DSM-5.10 From studies on ADHD genetics and prevalence to ADHD treatment response and related outcomes, SNAP-IV has been shown to be a valuable tool for research and clinical practice in ADHD.18–23 Notwithstanding, one criticism for broad use of SNAP-IV is the sparse investigation of its psychometric properties.13,24
Studies including school and clinical-based samples from Florida,13 Taiwan,25 Tokyo,26 and Buenos Aires27 have shown good psychometric parameters for the parent and/or teacher forms of the SNAP-IV. In Brazil, the SNAP-IV scale was translated into Brazilian Portuguese and adapted regarding content and semantic equivalency.28 However, no study has thoroughly evaluated its psychometric properties in the Brazilian population. The present study investigated the psychometric properties of the SNAP-IV scale – parent form – to establish its validity (internal structure and convergent correlations), reliability (internal consistency), and accuracy in screening for ADHD in a school and clinical-based sample from Belo Horizonte, Brazil.
MethodsEthical disclosureThis study is part of broader research about ADHD in a Brazilian sample (CAAE 02899412.9.0000.5149) and was approved by the local ethics board of the Federal University of Minas Gerais. All parents gave written consent for participation, and the children themselves gave assent for participation. The study was conducted following the principals of the Declaration of Helsinki and the relevant Brazilian legislation.
ParticipantsParticipants were 765 parents (∼89% mothers) of children from 4 to 16 years old. From those, 641 parents were recruited from eight public schools. Several schools were contacted by phone, and for those school principals who agreed to a meeting, the study's objectives and design were presented. Data collection happened in schools after a signed institutional endorsement letter was received. Families of one or more children attending from the first to the ninth grades at elementary school (5 or 6–14 years) received a set of documents and questionnaires (a letter describing the research objectives and design, consent forms, a questionnaire asking for sociodemographic and health information, and the SNAP-IV scale). Only data from children whose parents did not report any psychiatric, neurological, or genetic problem in a sociodemographic questionnaire were included in the school-based sample. One hundred twenty-four children with attention deficit/hyperactivity disorder (ADHD) followed in a specialized public outpatient clinic were also included. Participants of the clinical group underwent a semi-structured psychiatric diagnostic interview with the Brazilian version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL)29 and were diagnosed with ADHD following the DSM-IV criteria. At the time of the K-SADS-PL interview, 47 (38%) children were under some pharmacological treatment (psychostimulant n=19, antipsychotics n=4, antidepressant n=3, more than one medication n=16, medication not reported n=5). For those under medical treatment, the interview was conducted investigating symptoms before medication.
AssessmentSNAP-IV – the authors used the MTA-SNAP-IV, adapted for Brazil.28 It is a questionnaire with 26 items corresponding to the criterion A of the DSM-IV for ADHD and the symptoms of ODD. Parents rate their children's inattentive (items 1–9), hyperactive-impulsive (items 10–18), and defiant (items 19–26) behaviors using a 4-point Likert scale ranging from 0 (not at all) to 3 (very much). The scores were computed using three different scoring methods. The first one is a more traditional scoring method, where the total score of each dimension is averaged by the number of items (sum/9 for inattention and hyperactivity-impulsivity and sum/8 for ODD symptoms). The second scoring method was the sum of items in each dimension, producing a raw score ranging from 0 to 27 for inattention and hyperactivity-impulsivity and from 0 to 24 for the dimension of ODD. A third method involved the categorization of each SNAP-IV item as present or absent. The items scored as 0 (‘not at all’) and 1 (‘just a little’) were computed as absent (0 points), and scores equivalent to 2 (‘quite a bit’) and 3 (‘very much’) were computed as present (1 point). The latter generates a maximum score of 9 for inattention and hyperactivity-impulsivity, and of 8 for the dimension of ODD.
K-SADS-PL – parents underwent a semi-structured psychiatric diagnostic interview with the Brazilian version K-SADS-PL29 and current inattentive and hyperactive-impulsive symptoms were registered. All questions from the screening and supplement sections were investigated, and the summary checklist of evidence for ADHD (DSM-IV) was completed. The sum of inattentive and hyperactive-impulsive symptoms from the summary diagnose checklist can vary from 0 to 9 for each ADHD dimension.
Brazilian Economic Classification Criteria (CCEB) – an instrument of economic classification that provides evidence about the purchasing power and general situation of households through questions about the possession of durable goods and the educational level of the head of the household. A subject score can vary from 0 to 46 and is classified in one of six classes: A (average income of U$ 6694.87), B1 (average income of U$ 2966.03), B2 (average income of U$ 1555.13), C1 (average income of U$ 866.99), C2 (average income of U$ 520.83), and DE (average income of U$ 246.15) (ABEP, 2014). The distribution of classes in this sample was 26 (3.4%) A, 78 (10.2%) B1, 273 (35.7%) B2, 234 (30.6%) C1, 107 (14.0%) C2, and 47 (6.1%) DE.
Statistical and psychometric analysisThe association of sociodemographic characteristics with SNAP-IV variables was described through correlation analysis (Spearman correlation for age and socioeconomic level) and group comparisons (for gender).
The latent structure of SNAP-IV items was assessed by factor analysis (principal axis factoring and direct oblimin rotation design). The factor extraction criterion was eigenvalues larger than 1. The expected latent structure (inattention: items 1–9, hyperactivity/impulsivity: items 10–18, and ODD symptoms: items 19–26) was also tested by confirmatory factor analysis using the diagonally weighted least-squares estimator (WLSMV) for ordinal data. The root mean square error of approximation (RMSEA), confirmatory fit index (CFI), and Tucker–Lewys index (TLI) were used as goodness-of-fit indicators.
The convergent validity of the SNAP-IV scores was investigated by association (Spearman correlation) with the K-SADS-PL data. Reliability was assessed by estimating internal consistency. The authors computed three different indexes (i.e., Cronbach's alpha, Gutmann's λ, and MacDougall's omega) for each SNAP-IV subscale.
The accuracy of SNAP-IV for the classification of ADHD patients was assessed by receiver operator characteristic (ROC) curve analysis. For each subscale area under the curve, standard error and confidence intervals were calculated. As a cutoff score, values were chosen that offered the best balance between sensitivity and specificity (ratios closer to 1). The authors performed the ROC analysis for the three SNAP-IV scoring methods computed.
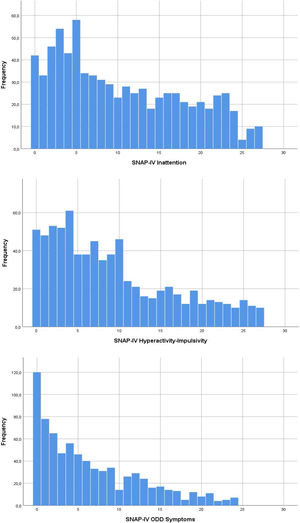
ResultsTable 1 shows the sample characteristics. Age was significantly associated with SNAP-IV hyperactivity-impulsivity (r(763)=−0.14, p<0.001), but not with inattention (r(763)=−0.03, p=0.407) or oppositional defiant behaviors (r(763)=−0.02, p=0.560). Socioeconomic level was not related to ADHD or ODD dimensions in this sample (inattention: r(763)=0.05, p=0.217, hyperactivity-impulsivity: r(763)=0.03, p<0.470, oppositional: r(763)=−0.003, p=0.939). Supplementary Fig. 1 shows the distribution of SNAP-IV scores.
Participant's description characteristics.
| All (n=765) | School sample (n=641) | ADHD sample (n=124) | |
|---|---|---|---|
| Age (years), mean (SD) | 9.30 (2.51) | 9.40 (2.56) | 8.74 (2.14) |
| Male, n (%) | 428 (56) | 331 (52) | 97 (78) |
| SES, mean (SD) | 23.72 (7.44) | 22.79 (6.93) | 28.52 (8.10) |
| ADHD presentation | |||
| Inattentive, n (%) | 47 (6.1) | – | 47 (38) |
| Hyperactive-impulsive, n (%) | 10 (1.3) | – | 10 (8) |
| Combined, n (%) | 67 (8.8) | – | 67 (54) |
| Psychiatric comorbidity | |||
| Oppositional defiant disorder | 34 (4.4) | – | 34 (27) |
| Mood/anxiety disorder | 42 (5.5) | – | 42 (34) |
ADHD, attention deficit/hyperactivity disorder; SES, socioeconomic level as measured by the Brazilian Economic Classification Criteria (higher values indicate higher purchasing power and better general conditions of the household). Since no clinical investigation was directly performed with the school sample, the unknown proportion of children with psychiatric diagnoses is represented by dashes rather than zeros.
There was a significant difference in scores’ intensity between girls and boys for all SNAP-IV measures (inattention: U=48697.0, p<0.001, r=−0.28, hyperactivity-impulsivity: U=54564.5, p<0.001, r=−0.21, oppositional: U=54611.0, p<0.001, r=−0.19) in the full sample. However, no significant differences by gender were found in the ADHD group for inattention (p=0.345), hyperactivity-impulsivity (p=0.569) or ODD symptoms (p=0.327). Table 2 shows SNAP-IV scores for the present sample.
Mean±standard deviation and 95th percentiles [in brackets] of SNAP-IV-parent report scores by gender and sample group.
| School sample (n=641) | ADHD sample (n=124) | |||||
|---|---|---|---|---|---|---|
| Mean scorea | Raw scoreb | Symptoms scorec | Mean scorea | Raw scoreb | Symptoms scorec | |
| Inattention | ||||||
| Male | 1.14±0.77 [2.56] | 10±7 [23] | 3±3 [9] | 2.11±0.60 [2.89] | 19±5 [26] | 7±2 [9] |
| Female | 0.78±0.68 [2.22] | 7±6 [20] | 2±3 [8] | 2.25±0.53 [3.00] | 20±5 [27] | 8±2 [9] |
| Total | 0.97±0.75 [2.44] | 9±7 [22] | 2±3 [8] | 2.14±0.58 [2.89] | 19±5 [26] | 7±2 [9] |
| Hyperactivity/impulsivity | ||||||
| Male | 1.00±0.78 [2.56] | 9±7 [23] | 3±3 [9] | 1.78±0.85 [3.00] | 16±8 [27] | 5±3 [9] |
| Female | 0.75±0.65 [2.11] | 7±6 [19] | 2±2 [7] | 1.70±0.82 [2.78] | 15±7 [25] | 5±3 [9] |
| Total | 0.88±0.73 [2.44] | 8±7 [22] | 2±3 [8] | 1.76±0.84 [3.00] | 16±8 [27] | 5±3 [9] |
| Oppositional | ||||||
| Male | 0.82±0.75 [2.38] | 7±6 [19] | 2±2 [7] | 1.28±0.83 [2.75] | 10±7 [22] | 3±3 [8] |
| Female | 0.62±0.70 [2.00] | 5±6 [16] | 1±2 [6] | 1.03±0.74 [2.13] | 9±6 [17] | 3±2 [6] |
| Total | 0.72±0.73 [2.25] | 6±6 [19] | 1±2 [7] | 1.23±0.81 [2.63] | 10±6 [22] | 3±3 [8] |
ADHD, attention deficit/hyperactivity disorder.
Exploratory factor analysis showed a three-factor structure composed of inattention, hyperactivity-impulsivity, and ODD symptoms. Only one item (item 10) revealed its higher factor loading on a different factor than expected (i.e., on inattention, not on hyperactivity-impulsivity) (Table 3). The confirmatory factor analysis suggests a good fit for the three-factor structure of the SNAP-IV scale (RMSEA: 0.072, CFI: 0.966, TLI: 0.963). The consistency of SNAP-IV factor structure was tested by splitting the overall sample into two randomly divided subsamples (n=382, n=383) and reanalyzing both datasets separately. Exploratory factor analysis showed the comparable results of both subsamples with the overall sample (Supplementary Table 1). Fit indexes from confirmatory factor analyses for random subsample 1 (RMSEA: 0.064, CFI: 0.973, TLI: 0.971) and random subsample 2 (RMSEA: 0.073, CFI: 0.966, TLI: 0.963) were satisfactory.
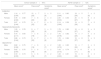
Factor analysis (item loads), reliability, and convergent validity of SNAP-IV subscales.
| SNAP-IV item/dimension | Inattention | Hyperactivity/impulsivity | ODD symptoms |
|---|---|---|---|
| SNAP.1 | 0.90 | 0.10 | 0.00 |
| SNAP.2 | 0.74 | −0.04 | 0.01 |
| SNAP.3 | 0.57 | −0.12 | 0.12 |
| SNAP.4 | 0.79 | −0.08 | 0.00 |
| SNAP.5 | 0.87 | 0.03 | 0.00 |
| SNAP.6 | 0.77 | 0.04 | 0.10 |
| SNAP.7 | 0.68 | −0.09 | −0.01 |
| SNAP.8 | 0.71 | −0.08 | 0.02 |
| SNAP.9 | 0.78 | 0.01 | 0.03 |
| SNAP.10 | 0.40 | −0.37 | 0.04 |
| SNAP.11 | 0.36 | −0.59 | −0.10 |
| SNAP.12 | 0.23 | −0.63 | 0.01 |
| SNAP.13 | 0.24 | −0.49 | 0.13 |
| SNAP.14 | 0.12 | −0.77 | −0.03 |
| SNAP.15 | −0.11 | −0.66 | 0.19 |
| SNAP.16 | 0.09 | −0.49 | 0.26 |
| SNAP.17 | 0.15 | −0.47 | 0.31 |
| SNAP.18 | 0.00 | −0.45 | 0.40 |
| SNAP.19 | 0.09 | −0.09 | 0.69 |
| SNAP.20 | −0.12 | −0.13 | 0.78 |
| SNAP.21 | 0.06 | −0.16 | 0.65 |
| SNAP.22 | −0.03 | −0.22 | 0.67 |
| SNAP.23 | 0.10 | −0.02 | 0.68 |
| SNAP.24 | 0.10 | 0.03 | 0.77 |
| SNAP.25 | 0.07 | 0.16 | 0.83 |
| SNAP.26 | 0.00 | 0.04 | 0.59 |
| Cronbach's α | 0.94 | 0.92 | 0.93 |
| Gutmann's λ | 0.94 | 0.92 | 0.93 |
| McDonalds’ ω | 0.94 | 0.92 | 0.93 |
| K-SADS-PL inattentiona | 0.59b | 0.25b | 0.11 |
| K-SADS-PL hyp-impa | 0.47b | 0.74b | 0.50b |
| SNAP-IV inattentiona | – | 0.73b | 0.60b |
| SNAP-IV hyperactivity/impulsivitya | 0.73b | – | 0.74b |
| SNAP-IV ODD symptomsa | 0.60b | 0.74b | – |
ODD, oppositional defiant disorder; K-SADS-PL, schedule for affective disorders and schizophrenia for school aged children – present and lifetime version; hyp-imp, hyperactivity-impulsivity. Values in bold font represent the highest load across the three factors.
Correlations between SNAP-IV scores and K-SADS-PL ADHD measures are shown in Table 3. The SNAP-IV inattentive dimension showed a strong correlation with the inattentive dimension of the K-SADS-PL and a moderate correlation with the K-SADS-PL hyperactivity-impulsivity. Hyperactivity-impulsivity in SNAP-IV showed a moderate correlation with the K-SADS-PL inattention and a strong correlation with hyperactivity-impulsivity as measured by the K-SADS-PL. The ODD symptoms showed no significant association with the K-SADS-PL inattention, but a strong correlation with the K-SADS-PL hyperactivity-impulsivity score was found.
Reliability analysis is depicted in Table 3. All SNAP-IV scales showed very high internal consistency coefficients (all above 0.91).
SNAP-IV inattention scores were highly predictive of ADHD diagnosis (area under the curve: 0.877 for the averaging rating method and the raw sum method, and 0.874 for the symptom presence/absence method). SNAP-IV hyperactivity-impulsivity symptoms showed moderate accuracy for ADHD classification (0.788 and 0.784), as well as for ODD symptoms (0.704 and 0.703). The accuracy data are shown in Table 4.
ROC curve analysis and cutoff scores for SNAP-IV measures.
| Area | SE | p | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| Meana/Raw scoreb | ||||||
| Inattention | 0.877 | 0.015 | <0.001 | ≥1.72/≥16 | 0.792 | 0.811 |
| Hyperactivity-impulsivity | 0.788 | 0.023 | <0.001 | ≥1.17/≥11 | 0.700 | 0.728 |
| ODD symptoms | 0.704 | 0.025 | <0.001 | ≥0.81/≥7 | 0.708 | 0.657 |
| Symptoms scorec | ||||||
| Inattention | 0.874 | 0.016 | <0.001 | ≥6 | 0.817 | 0.805 |
| Hyperactivity-impulsivity | 0.784 | 0.024 | <0.001 | ≥4 | 0.700 | 0.761 |
| ODD symptoms | 0.703 | 0.026 | <0.001 | ≥2 | 0.675 | 0.684 |
ROC, receiver operator characteristic; ODD, oppositional defiant disorder; SE, standard error.
Supplementary Table 2 shows the Brazilian version of SNAP-IV, as translated by Mattos et al.28
DiscussionThe results provided evidence of validity and reliability for the SNAP-IV scale in a Brazilian sample. Its internal structure, investigated by exploratory and confirmatory factor analysis, suggested a three-factor structure representing two dimensions of ADHD symptoms (inattention and hyperactivity-impulsivity) and one dimension of ODD. SNAP-IV subscales showed significant moderate-strong correlations with the K-SADS-PL dimensional data on inattention and hyperactivity-impulsivity. All subscales also showed high internal consistency and accuracy to classify an ADHD diagnosis, at least for the clinical sample.
Regarding its internal structure, the present study's results for SNAP-IV are similar to Gau et al., who investigated the factor structure of SNAP-IV in a sample from China.25 They reported a good fit for a SNAP-IV structure of inattention, hyperactivity-impulsivity, and ODD symptoms. The same fit was observed by Bussing et al. in a north-American sample,13 and by Inoue et al. in a Japanese sample.26 These results suggest that the best fit comes from the three-factor model of SNAP-IV in distinct cultures. However, it should be noted that this structure might change according to the informant, since in at least one study a four-factor model better fit the questionnaire when teachers reported participants’ symptoms.30
Strong correlations were found between SNAP-IV inattention and hyperactivity-impulsivity measures with the correspondent K-SADS-PL variables, and moderate correlations with the opposite ADHD dimension. This association is expected since both scales are assessing the same phenomena based on parent reports. Still, this is considered evidence of construct validity for SNAP-IV. ODD symptoms showed a moderate correlation with the K-SADS-PL hyperactivity-impulsivity measure, but not with the inattentive dimension. Results may suggest that questionnaires such as the SNAP-IV are reliable when compared to face-to-face interviews such as the K-SADS-PL in measuring ADHD symptoms. Strong correlations between the SNAP-IV with other scales of child behavioral problems were reported by Gau et al.25 using the Child Behavior Checklist (CBCL).
The internal consistency in the current sample was similar to that of Gau et al., which reported Cronbach's alphas ranging from 0.88 to 0.90.25 The results are also in accordance to Bussing et al., who reported coefficients higher than 0.70 in all subscales,13 and to Inoue et al., who reported coefficients higher than 0.92 in all subscales.26
SNAP-IV's accuracy for ADHD classification is usually high, as seen in the present study's results (accuracy ranging from 0.70 to 0.87), even though only the clinical sample was investigated in this regard. Alda and Serrano-Troncoso reported SNAP-IV accuracy of 0.82 using the pediatrician's assessment of ADHD as criteria.31 A South-American study conducted in Argentina reported sensitivities ranging from 0.54 to 0.86 and specificity ranging from 0.65 to 0.79 for the SNAP-IV measures according to different cutoff scores.27 Gau et al. reported classification rates ranging from 0.69 to 0.75 for ADHD patients without medication and from 0.56 to 0.58 for patients currently medicated.25 Both medicated and unmedicated groups scored significantly higher than children with typical development. Bussing et al. reported accuracies from 0.71 to 0.85 in detecting children whose families and teachers expressed concerns and lower accuracy for children who met DSM-IV criteria for ADHD (0.58–0.76).13 However, it should be noted that, despite the relatively high accuracy for ADHD screening, SNAP-IV only documents the symptoms (inattention, hyperactivity-impulsivity, and ODD), while the clinical diagnosis of the disorder requires an assessment of its onset, progression, and functional impairment associated.
This study has limitations that should be addressed. Due to limitations in the study setting and design, it was not possible to include a retest condition for the SNAP-IV parent rating, thus not estimating its temporal stability by test–retest reliability. Other studies showed lower reliability estimates for this method when compared to internal consistency.25 A teacher's report of SNAP-IV data was not included. The teacher's report may increase SNAP-IV's screening power and might show different psychometric characteristics when compared to the parent's report, especially concerning the impulsivity symptoms.13,26 Since no formal investigation of psychiatric diagnosis in the school sample was performed, it was not possible to provide SNAP-IV accuracy for ADHD screening in the non-clinical sample, nor control for other mental health features. It is not possible to provide population norms for the test since this study enrolled a convenience sample.
The parent SNAP-IV showed robust psychometric properties in a Brazilian school and clinical sample. Thereby, this study adds to the few studies in the literature that have put SNAP-IV under thorough analysis. SNAP-IV's structure may vary according to the information source, but not according to distinct cultures in the world. The authors suggest that SNAP-IV may be a valuable instrument for assessing ADHD symptom severity, besides being helpful for diagnosis purposes.
Conflicts of interestThe authors declare no conflicts of interest.
INCT-MM (FAPEMIG: CBB-APQ-00075-09/CNPq 573646/2008-2).
Please cite this article as: Costa DS, de Paula JJ, Malloy-Diniz LF, Romano-Silva MA, Miranda DM. Parent SNAP-IV rating of attention-deficit/hyperactivity disorder: accuracy in a clinical sample of ADHD, validity, and reliability in a Brazilian sample. J Pediatr (Rio J). 2019;95:736–43.
Study conducted at Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil.





