
massage can help relieve pain, although empirical evidence is scarce and contradictory. This study aims to assess the effectiveness of a massage protocol in relieving pain in children hospitalized with cancer.
Methodsa randomized, controlled, and single-blind trial was performed in a sample of 52 children aged between 10 and 18 years who were hospitalized in a pediatric cancer ward. The intervention consisted of the implementation of a massage protocol with three sessions of 20 to 30minutes on alternate days over a one-week period. The effectiveness of the protocol was evaluated by assessing pain using the Brief Pain Inventory (BPI), while the effectiveness of each massage session was measured using the Visual Analogue Scale (VAS).
Resultsthe massage protocol was only effective in reducing the interference of pain in walking (p<0.05), although it also contributed to relieve pain and its impact on the children's activities. After each massage session, the intensity of the pain experienced by the child decreased (p<0.001).
Conclusionsdespite the small sample size, massage therapy appears to be a useful intervention in reducing pain in children with cancer. However, there are still questions regarding the effectiveness of this massage protocol. The authors recommend its use due to its contribution to the promotion of the child's well-being and quality of life.
a massagem é uma intervenção que pode contribuir para o alívio da dor, embora as evidências empíricas sejam escassas e contraditórias. O objetivo deste trabalho foi avaliar a eficácia de um protocolo de massagem no alívio da dor na criança internada, com patologia oncológica.
Métodosatravés de um estudo randomizado e controlado com cegamento simples, foram estudadas 52 crianças, com idades compreendidas entre os 10 e os 18 anos, internadas num serviço de oncologia pediátrica. A intervenção consistiu na aplicação de um protocolo de massagem de três sessões com duração entre 20 a 30 minutos em dias alternados durante uma semana. A eficácia do protocolo foi medida através da avaliação da dor com a aplicação do Inventário Resumido de Dor e a eficácia de cada sessão de massagem pela Escala Visual Analógica (EVA).
Resultadoso protocolo de massagem apenas se revelou eficaz na diminuição da interferência da dor no andar (p<0,05), apesar de ter contribuído para o alívio da dor e sua interferência nas atividades da criança. Após cada sessão de massagem a intensidade da dor sentida pela criança diminuiu (p<0,001).
Conclusõesapesar da reduzida dimensão da amostra, a massagem parece ser uma intervenção útil no alívio da dor da criança que sofre de patologia oncológica, embora permaneçam dúvidas quanto à eficácia deste protocolo de massagem. Todavia, os autores recomendam a sua utilização pela sua contribuição na promoção do bem-estar e qualidade de vida da criança.
Pain is an unpleasant and subjective experience that involves sensory, affective, cognitive, social, and behavioral components; it is a major cause of human suffering and loss of quality of life. Health professionals have an ethical, deontological, and clinical responsibility to play a main role in the management of care provided to children and their families to contribute to effective pain control.
Unconventional therapies are currently an unavoidable reality in the world of health care, and they have been widely used in Eastern cultures. The search for the best evidence in pain control has led researchers to the discovery of their benefits, so they can be associated to existing therapies, as another element that favors a better quality of life.
There have been few studies on the use of massage in children with cancer.1 The myth that massage may contribute to the dissemination of metastasis has been a major obstacle to its implementation.2 However, a review study that evaluated the prevalence of unconventional therapies in children found a prevalence of use of massage therapy in children with cancer that ranged between 7% and 66%.3
The little scientific evidence in this area suggests the positive effect of massage on several dimensions of physical and/or psychological symptoms in children and adolescents with different health problems.4,5 However, studies with randomized controlled experimental designs are scarce, the methodologies used are varied, and children with cancer are a particularly understudied group of patients. In a search performed in the Cochrane Library database using the keywords pain, massage, child, and cancer, and no other restriction criteria, only four studies were retrieved, one review study and three randomized controlled trials, which illustrates this problem.
Some authors5–9 have attributed to massage therapy a significant role in relieving pain; reducing stress, anxiety, depression, anger, fatigue, constipation, and blood pressure; inducing a relaxation state; improving blood circulation and lymphatic flow; increasing muscle tone and range of motion; and even benefits in recovery from injuries and psychopathological symptoms. The findings of the few studies performed indicate the benefits of massage in inducing physiological relaxation and reducing anxiety and pain.1,4,10 However, the results are not consistent and there have been studies that indicated the absence of massage effect on these and other symptoms such as nausea, fatigue, and sleep disorders.10,11
The experience of the use of massage in oncology is preliminary, but safe.2 It may, however, be contraindicated if the child has a fever; it is not advisable to massage irradiated sites or inflamed skin lesions, and soft gliding movements and slight pressure are required due to the bleeding risk in thrombocytopenic children.6
The objective of this study was to evaluate the effectiveness of a massage protocol implementation aimed at relieving pain in hospitalized children with cancer.
MethodsThis was a prospective, longitudinal, randomized, controlled, and single-blinded study, i.e., the evaluator was unaware of group distribution, which occurred in a pediatric oncology service between November of 2010 and March of 2011.
This study was approved by the Hospital Board of Directors and Ethics Committee, and was conducted in accordance with the Declaration of Helsinki of the World Medical Association. Participation in the study was preceded by the informed consent given by the legal guardian of the child and/or adolescent.
The study population consisted of children and adolescents aged between 10 and 18 years, diagnosed with cancer and undergoing treatment (chemotherapy, antibiotics, or steroid corticoid therapy). Children whose diagnosis was not established; critically-ill; in the first three days after surgery; in contact isolation; with fever; with risk of bleeding (platelet count less than 10,000); or with changes in consciousness level or cognitive disorders were excluded. The selection of participants was randomized into two groups (intervention and control), with a sample of 26 children per group.
Ten nurses who worked at the service participated in data collection; five collected data (control group), and the remaining five performed the massage protocol (intervention group).
Four training sessions were performed to standardize the massage technique implementation, clarify the data collection methodology, and apply the protocol in the intervention and control groups.
Intervention protocolPain assessment was performed in all children upon admission at the service (day 1) and on the last day of the protocol (day 6). In the control group (CG), the usual care for management of pain or other symptoms was performed. The intervention group (IG) was submitted to three massage sessions on alternate days during one week (days 1, 3 and 5). Each massage session lasted between 20 and 30minutes, and consisted in applying slight pressure using sliding and circular movements and straight line movements to warm up and massage the skin, starting on the dorsal-lumbar region, followed by the hands, legs, and feet, using sweet almond oil heated in a water bath. Throughout the procedure, the nurse's hands were always kept in contact with the child and/or adolescent. Pain severity was evaluated in the half-hour before and after each massage session.
Pain assessment toolsThe tools used to assess pain were those recommended by Dworkin et al.12 The Visual Analog Scale (VAS) was used to assess pain intensity before and after each massage session and the Brief Pain Inventory (BPI),13 to evaluate pain and interference with the child's activities on days 1 and 6. This tool was adapted for use in children aged 10 to 18 years. This adaptation consisted in eliminating the question on mean pain in the previous week and pain interference with enjoyment of life, due to the difficulty in answering it experienced by many children and/or adolescents.
When asked about pain interference with activities, the following were considered as examples: general activity (personal hygiene care, teeth brushing, and changing pajamas); disposition (will/willingness to do or continue doing something that the child started or will start); ability to walk (ambulation); recreational activities (studying, participating in plays, games and other activities in group, and playing); and interaction with others (other children, volunteers, teachers, aides, nurses, family). The question regarding pain interference with recreational activities replaced that of interference with normal work activities.
Statistical analysisStatistical analysis was performed with the PASW Statistics software, release 18.0 for Windows®. The normality of the distributions was analyzed by the Shapiro-Wilk test and analysis of the histogram, and it was observed that none had a normal distribution. The descriptive study of data was carried out for categorical variables by absolute frequencies, relative percentages, and for continuous variables by statistical measures of order, and minimum and maximum limits. The differences between the groups (intervention and control) and in the groups (first and sixth days) were analyzed for categorical variables by the chi-squared test, and for continuous variables, by Mann-Whitney's U test for independent samples (between the groups) and Wilcoxon's test for paired samples (within the groups). Statistically significant differences were considered in all tests when p ¿ 0.05.
ResultsThe sample consisted of 52 children aged between 10 and 18 years, with a median of 13.5 years in the IG and 12 years in the CG. There was a predominance of the male gender (20 patients; 76.9%) in the IG, and of the female gender (14 patients; 53.8%) in the CG. The most prevalent cancer types in both groups were leukemias, lymphomas, and sarcomas.
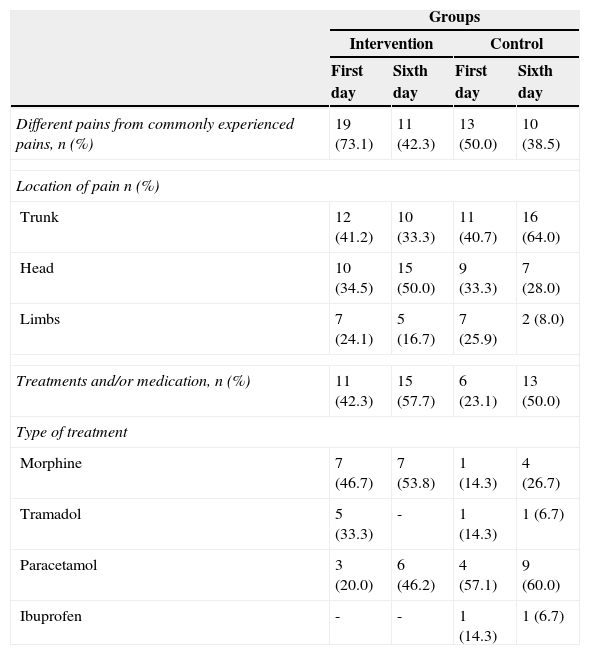
Most children reported pain that was different from the usual in the previous week before starting the protocol (day 1), in both groups: 19 patients (73.1%) in the IG and 13 patients (50.0%) in CG. At the end of the protocol (day 6), a decrease in pain complaints was observed in both groups, 11 patients (42.3%) in IG and 10 patients (38.5%) in the CG. The pain was located mainly in the trunk and head; pain increase in the head was reported by 15 children (50.0%) from the IG on day 6, and pain increase in the trunk was reported by 10 children (33.3%) from the CG.
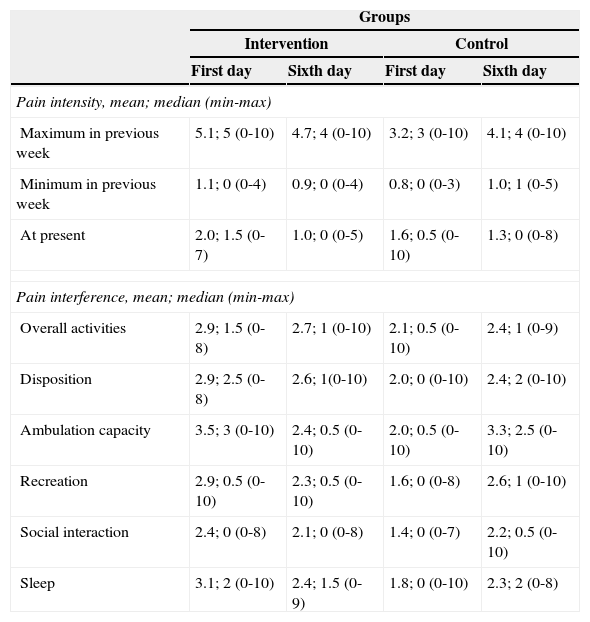
The median of maximum pain intensity felt by the child and/or adolescent in the previous week, on day 1 was higher in the IG, at a level of 5 (0-10), compared with the CG, at a level of 3 (0-10). The largest difference in the median of minimal pain from the previous week was observed among children in the control group on day 1 and 6, 0 (0-3) and 1 (0-5), respectively.
Regarding the pain felt at the time, the difference was greater in IG between days 1 and 6, 1.5 (0-7) and 0.0 (0-5), respectively.
On day 6, the number of children who received pharmacological treatment for pain relief increased in both groups: 13 in the IG (50.0%) and 15 in the CG (57.7%). A greater use of opioids was observed in the IG (morphine and tramadol), while the use of non-opioid (paracetamol and ibuprofen) was higher in the CG (Table 1).
Different pains from those commonly experienced in the previous week and their management.
| Groups | ||||
|---|---|---|---|---|
| Intervention | Control | |||
| First day | Sixth day | First day | Sixth day | |
| Different pains from commonly experienced pains, n (%) | 19 (73.1) | 11 (42.3) | 13 (50.0) | 10 (38.5) |
| Location of pain n (%) | ||||
| Trunk | 12 (41.2) | 10 (33.3) | 11 (40.7) | 16 (64.0) |
| Head | 10 (34.5) | 15 (50.0) | 9 (33.3) | 7 (28.0) |
| Limbs | 7 (24.1) | 5 (16.7) | 7 (25.9) | 2 (8.0) |
| Treatments and/or medication, n (%) | 11 (42.3) | 15 (57.7) | 6 (23.1) | 13 (50.0) |
| Type of treatment | ||||
| Morphine | 7 (46.7) | 7 (53.8) | 1 (14.3) | 4 (26.7) |
| Tramadol | 5 (33.3) | - | 1 (14.3) | 1 (6.7) |
| Paracetamol | 3 (20.0) | 6 (46.2) | 4 (57.1) | 9 (60.0) |
| Ibuprofen | - | - | 1 (14.3) | 1 (6.7) |
When analyzing the mean pain intensity and interference with the activities of the child and/or adolescent, the IG presented a decrease in mean values of pain and interference in the activities between day 1 and 6; the opposite was observed in the CG, with the exception of the pain felt at the time, 1.6 and 1.3. The greatest differences regarding pain interference with activities among children and/or adolescents enrolled in the CG were in sleep 1.8; 0 (0-10) and 2.3; 2 (0-8); recreational activities 1.6; 0 (0-8) and 2.6; 1 (0-10); and interaction with other people 1.4; 0 (0-7) and 2.2; 0.5 (0-10). In the IG, the largest differences regarded the ambulatory capacity; 3.5; 3 (0-10) and 2.4; 0.5 (0-10). On day 1, differences were observed among children and/or adolescents in the IG and CG regarding disposition 2.9; 2.5 (0-8) and 2.0; 0 (0-10), in general activity between 2.9; 1.5 (0-8) and 2.1; 0.5 (0-10) (Table 2).
Pain intensity and interference with previous week activities.
| Groups | ||||
|---|---|---|---|---|
| Intervention | Control | |||
| First day | Sixth day | First day | Sixth day | |
| Pain intensity, mean; median (min-max) | ||||
| Maximum in previous week | 5.1; 5 (0-10) | 4.7; 4 (0-10) | 3.2; 3 (0-10) | 4.1; 4 (0-10) |
| Minimum in previous week | 1.1; 0 (0-4) | 0.9; 0 (0-4) | 0.8; 0 (0-3) | 1.0; 1 (0-5) |
| At present | 2.0; 1.5 (0-7) | 1.0; 0 (0-5) | 1.6; 0.5 (0-10) | 1.3; 0 (0-8) |
| Pain interference, mean; median (min-max) | ||||
| Overall activities | 2.9; 1.5 (0-8) | 2.7; 1 (0-10) | 2.1; 0.5 (0-10) | 2.4; 1 (0-9) |
| Disposition | 2.9; 2.5 (0-8) | 2.6; 1(0-10) | 2.0; 0 (0-10) | 2.4; 2 (0-10) |
| Ambulation capacity | 3.5; 3 (0-10) | 2.4; 0.5 (0-10) | 2.0; 0.5 (0-10) | 3.3; 2.5 (0-10) |
| Recreation | 2.9; 0.5 (0-10) | 2.3; 0.5 (0-10) | 1.6; 0 (0-8) | 2.6; 1 (0-10) |
| Social interaction | 2.4; 0 (0-8) | 2.1; 0 (0-8) | 1.4; 0 (0-7) | 2.2; 0.5 (0-10) |
| Sleep | 3.1; 2 (0-10) | 2.4; 1.5 (0-9) | 1.8; 0 (0-10) | 2.3; 2 (0-8) |
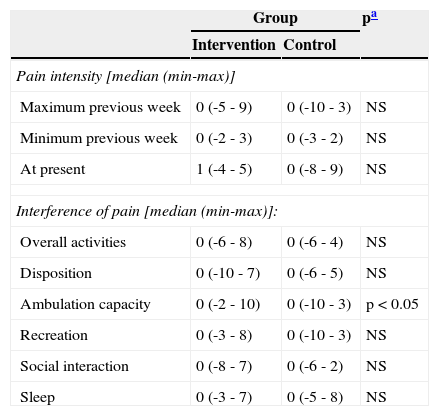
There were no statistically significant differences when comparing the IG and CG on day 1 and 6. However, analysis of the differences between day 1 and 6 between the IG and the CG shows statistically significant lower pain interference with the ambulatory capacity (Table 3).
Differences between groups regarding pain intensity and interference in activities.
| Group | pa | ||
|---|---|---|---|
| Intervention | Control | ||
| Pain intensity [median (min-max)] | |||
| Maximum previous week | 0 (-5 - 9) | 0 (-10 - 3) | NS |
| Minimum previous week | 0 (-2 - 3) | 0 (-3 - 2) | NS |
| At present | 1 (-4 - 5) | 0 (-8 - 9) | NS |
| Interference of pain [median (min-max)]: | |||
| Overall activities | 0 (-6 - 8) | 0 (-6 - 4) | NS |
| Disposition | 0 (-10 - 7) | 0 (-6 - 5) | NS |
| Ambulation capacity | 0 (-2 - 10) | 0 (-10 - 3) | p<0.05 |
| Recreation | 0 (-3 - 8) | 0 (-10 - 3) | NS |
| Social interaction | 0 (-8 - 7) | 0 (-6 - 2) | NS |
| Sleep | 0 (-3 - 7) | 0 (-5 - 8) | NS |
NS, non-significant.
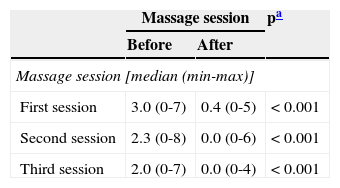
All children and/or adolescents presented significant pain relief after each massage session (Table 4).
Pain intensity before and after each massage session.
| Massage session | pa | ||
|---|---|---|---|
| Before | After | ||
| Massage session [median (min-max)] | |||
| First session | 3.0 (0-7) | 0.4 (0-5) | < 0.001 |
| Second session | 2.3 (0-8) | 0.0 (0-6) | < 0.001 |
| Third session | 2.0 (0-7) | 0.0 (0-4) | < 0.001 |
Although there was a decrease in pain intensity and its interference with the child and/or adolescent's activities in the previous week, it was only statistically significant for the interference with the capacity of ambulation. This result is consistent with other studies, whose results indicated a non-significant improvement.6,9,10 Post-White et al.,1 studying children with cancer between 1 and 18 years, using weekly massage sessions for four weeks, observed a decrease in heart rate and anxiety in children younger than 14 years, but no significant change in blood pressure, cortisol, pain, nausea, fatigue; also, similarly to the present study, children and parents reported that massage helped them feel better.
If there were doubts regarding the effectiveness of a massage protocol for pain control and for decreasing the interference of pain with some activities of the child and/or adolescent, it was demonstrated that massage sessions performed on alternate days for one week were effective in relieving the intensity of pain felt at the time that followed each massage session, which was significant and corroborates studies in adults.6 Massage therapy has known mechanical, reflex, and psychological effects. In the circulatory system, it facilitates drainage and mobilization of interstitial fluids. The friction of the manipulation causes an increase in skin temperature, which promotes relaxation, metabolic activity, release of tissue adhesions, and increase in the threshold of nociceptive message uptake. The psychological effects are inseparable from the established inter-relationship, which conveys affection, trust, and hope.
The IG and CG were equivalent; however, it was observed on day 6 (end of protocol) that children from the IG received more opioid drugs, while in the CG, non-opioid drugs were the main choice.
For ethical reasons, this variable cannot be controlled, but the fact that there were no significant differences between the groups reinforces the belief that, at least in this study, this protocol, despite having contributed to the reduction of pain and interference with the child and/or adolescent's activities, only showed to be effective in decreasing the interference of pain when ambulating. No plausible justification was found for this particular result; however, the relationship established with the child and/or adolescent and the family, with demonstrations of affection, hope, and confidence, beyond the pain relief felt at the end of each massage session, may have provided or facilitated moments when the child and/or adolescent felt willingness, motivation, and some capacity to ambulate.
Performing randomized controlled trials alone has challenges that are not always easy to overcome, and this difficulty increases when the subjects are children with cancer. Every child in the IG received three massage sessions on alternate days during the week, which was not always easy, because for many, and fortunately for the child/adolescent, hospitalization was shorter than six days.
The blind assessment required another group of staff nurses whose coordination was not always easy. A pretest/post-test study design with control group was chosen, but, for future studies, it will be important to compare results with cross-sectional design studies, which will make variable control easier.
Once the unfounded fear on the part of healthcare professionals of the supposed correlation between massage and the risk of metastases is overcome,1 there will be a greater openness to studies involving children and/or adolescents with cancer. These investigations are crucial to create evidence to support this practice. Two types of studies are important in this phase: qualitative studies that can assess the usefulness of the intervention as reported by Hughes et al.,6 and randomized controlled trials to evaluate the physiological effects of massage and the effectiveness of massage and protocols in pain control, using a placebo intervention as the comparison standard, beyond the standard intervention of the service and not only this one, as was the case in the present investigation.
Massage is an intervention that can be implemented in practice, whether by health professionals or parents, but specific guidelines are necessary for its implementation, including the rhythm, pressure, direction, duration, and frequency.
Advances in science and technology have provided a higher percentage of cure and survival in children and/or adolescents with cancer; however, they have not been exempted from pain, suffering, and impaired quality of life. The search for evidence cannot be focused only on interventions that save lives, but increasingly on those promoting the best quality of life. It is in this sense that massage therapy appears to have an important contribution.
LimitationsThe conclusions of this study are limited by the small sample size and low statistical power. The children's length of hospital stay, number of massage sessions performed, and stress of the team that implemented the study were factors that contributed to sample decrease. Study recruitment was not hampered by a lack of interest in massage, but limited by the fact that it occurred outside normal working hours. Additionally, the application of the BPI required a language adaptation to children aged 10 years or older, as it had been only validated for adults.
ConclusionDespite the small sample size, this study suggests that massage is helpful in relieving pain after each massage session. However, conducting sessions on alternate days for one week only was shown to be effective in decreasing the interference of pain during ambulation. Massage therapy appears to be a useful intervention for the relief of pain and its interference in the activities of the child/adolescent with cancer, although questions remain about the effectiveness of this protocol. The authors recommend its use due to its contribution in promoting well-being and improving quality of life.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Batalha LM, Mota AA. Massage in children with cancer: effectiveness of a protocol. J Pediatr (Rio J). 2013;89:595–600.




