
To describe the profile of women with children aged under 4 months living in the Brazilian state capitals and in the Federal District according to their working status and to analyze the influence of maternity leave on exclusive breastfeeding (EBF) among working women.
MethodsThis was a cross-sectional study with data extracted from the II National Maternal Breastfeeding Prevalence Survey carried out in 2008. Initially, a descriptive analysis of the profile of 12,794 women was performed, according to their working status and maternity leave and the frequency of maternity leave in the Brazilian regions and capitals. The study used a multiple model to identify the influence of maternity leave on EBF interruption, including 3766 women who declared they were working and were on maternity leave at the time of the interview. The outcome assessed in the study was the interruption of the EBF, classified by the WHO.
ResultsRegarding the working status of the mothers, 63.4% did not work outside of their homes and among those who worked, 69.8% were on maternity leave. The largest prevalence among workers was of women older than 35 years of age, with more than 12 years of schooling, primiparous and from the Southeast and South regions. The lack of maternity leave increased by 23% the chance of EBF interruption.
ConclusionMaternity leave contributed to increase the prevalence of EBF in the Brazilian states capitals, supporting the importance of increasing the maternity leave period from four to six months.
Descrever perfil das mulheres com filhos menores de 4 meses residentes nas capitais brasileiras e no Distrito Federal segundo situação de trabalho e analisar a influência da licença-maternidade sobre o aleitamento materno exclusivo entre as mulheres trabalhadoras.
MétodosTrata-se de um estudo transversal com dados extraídos da II Pesquisa Nacional de Prevalência do Aleitamento Materno realizada em 2008. Inicialmente foi realizada análise descritiva do perfil das 10.995 mulheres participantes do estudo segundo situação de trabalho e de licença-maternidade, bem como a frequência de licença-maternidade nas regiões brasileiras e capitais. Em seguida, para identificar a influência da licença-maternidade na interrupção do aleitamento materno exclusivo, realizou-se modelo múltiplo, onde foram incluídas 3.766 mulheres que declararam trabalhar e estar em licença-maternidade no momento da entrevista. O desfecho adotado no estudo foi a interrupção do aleitamento materno exclusivo, classificado de acordo com a definição da Organização Mundial da Saúde.
ResultadosEm relação à situação de trabalho, 63,4% das mães entrevistadas no Brasil não trabalhavam fora do lar e dentre as que trabalhavam fora, 69,8% usufruíam da licença-maternidade. Verificou-se maior concentração de mulheres que trabalhavam fora entre aquelas com mais de 35 anos, mais de 12 anos de escolaridade, primíparas, das regiões Sudeste e Sul. Para as mulheres que não estavam em licença-maternidade, após ajuste para todas as co-variáveis, houve um aumento da prevalência de interrupção do aleitamento materno exclusivo (RP [IC95%] ajustada 1,23 [1,11 – 1,37]).
ConclusãoVerificou-se que as mulheres que não estavam em licença-maternidade de 120 dias apresentaram maior prevalência de interrupção do aleitamento materno exclusivo nas capitais brasileiras e Distrito Federal, no ano de 2008, reforçando a importância da ampliação da licença-maternidade para 6 meses.
Exclusive breastfeeding (EBF) offers many benefits for the health of infants and their mothers.1 However, it is estimated that only 37% of children under 6 months of age are exclusively breastfed worldwide, a reality that is far from that recommended by the World Health Organization (WHO), which has established an EBF prevalence goal of 50% by 2025.2 In Brazil, the II Maternal Breastfeeding Prevalence Survey (Pesquisa Nacional de Prevalência de Aleitamento Materno [PPAM]), carried out in 2008, found that 41% of children under 6 months of age were exclusively breastfed.3 Considering this scenario, identifying factors and strategies that may contribute to increase EBF is a worldwide challenge. Among the factors associated with early interruption of EBF, maternal work outside of the home has been identified as an obstacle.4–8
The International Labor Organization (ILO), in the beginning of the 20th century, held in Washington their third convention on women's employment before and after childbirth. In 1935, Brazil ratified the recommendations of this convention, which guaranteed return to work at six weeks of postpartum and two half-hour breaks to breastfeed during the working day.9 In 1988, the Brazilian Constitution established the women's right to a maternity leave lasting 16 weeks (120 days),10 longer than the 14-week international maternity leave recommendation (ILO n. 183/2000).11 I In 2008, Law n. 11,770 was passed, giving women the option to extend the maternity leave to 180 days (24 weeks).12
Concerns about maternal work and breastfeeding have increased due to the growing participation of women in the labor market,13,14 making it impossible for women to stop working for an unpaid period to dedicate themselves to the care of their children, which can lead to changes in the childcare and feeding patterns.
Thus, it becomes essential to identify the impact of maternity leave on breastfeeding protection, aiming to strengthen and create new public policies. Therefore, this study aimed to describe the profile of women with children aged under 4 months residing in the Brazilian capitals and in the Federal District according to their working status and to analyze the influence of maternity leave on EBF among women working outside of the home.
MethodsThis is a cross-sectional study, whose data were obtained from the II PPAM carried out in 2008. This survey collected information from children under 1 year of age who were brought for the second phase of the 2008 multi-vaccine campaign in all Brazilian capitals and in the Federal District (Distrito Federal [DF]). The PPAM was carried out using conglomerate samples, by drawing lots in two stages and probability proportional to the size of the conglomerates.
In the first stage, the vaccination units were selected by drawing lots, and in the second, the children were systematically selected in each unit, also by drawing lots. The sample size considered information on the distribution of vaccinated children in each vaccination unit in 2007 and the prevalence of EBF obtained at the I PPAM, carried out in 1999 in the 26 capitals and in the DF.15 Details on the sampling procedures have been described in previous publications.3,16 To reach the aims of this study, children under 4 months of age was analyzed, the age range in which it would be possible for mothers to be on maternity leave in 2008.
The data collection tool was applied to the children's caregivers during the vaccination campaign. The questionnaire contained closed questions about the characteristics of the children and their mothers, about infant feeding in the last 24h, and about the healthcare services they attended. The mothers also stated, at the time of the interview, whether they were working outside of the home or not, and whether they were on maternity leave. The data were entered into a web application by team members in each municipality.
Initially, a descriptive analysis was performed on the profile of the 10.995 women participating in the study, according to their working status and maternity leave, as well as the frequency of maternity leave in Brazilian regions and capitals. Subsequently, to identify the influence of the maternity leave on EBF interruption, a multiple model was developed, which included only the 3766 women who reported working outside of the home or being on maternity leave at the time of the interview. The outcome adopted in the present study was EBF interruption, classified according to the WHO definition.17
The main independent variable was whether the working mother was or not on maternity leave at the time of the interview. The following variables were analyzed: maternal age (<20, 20–35, >35 years), maternal schooling (0–8, 9–12, >12 years of schooling), primiparity (yes/no), type of delivery (vaginal/forceps, cesarean section), the child's gender (female/male), low birth weight (yes/no), health care (Public Network – Sistema Único de Saúde [SUS]; Private Service/Health Insurance), pacifier use in the last 24h (yes/no), and the child's age (0–60 days and 61–120 days).
Poisson regression was used to estimate the prevalence ratio (PR) and 95% confidence intervals (95% CI), with robust variance for bivariate and multiple analyses. Variables that showed p<0.20 in the bivariate analysis were introduced in the multiple model. In the multiple model, variables that showed p<0.05 were considered to be associated with the outcome. A linear trend test was performed for the variables in which there was a theoretical assumption of a dose–response association. Although the child's age was a control variable, a multiple model was tested with the age variable categorized from month to month. In this analysis, there was no relevant adjustment in the prevalence ratio of the response variable, and thus, this approach was not explored (data not shown).
The II PPAM database was exported to the Stata software (Stata Statistical Software: Release 9. StataCorp., 2005, College Station, TX, USA) for data analysis. The sample complexity was considered at all analytical stages of the analysis.15
The research protocol was approved by the Ethics Committee of Instituto de Saúde de São Paulo (Protocol n. 001/2008, of 05/06/2008), after consulting the National Commission for Research Ethics (Comissão Nacional de Ética em Pesquisa [CONEP]).
ResultsThe study involved 12,794 women with children under 4 months of age, from which 10.995 mother replied regarding the work variable. Half of the sample consisted of women with male children and the infants’ mean age was 59.5 days. It was verified that 37.4% of the children were born in a hospital accredited as a “Child-Friendly Hospital”; low birth weight occurred in 8.7% of the cases and pacifier use was reported for 36.4% of the children. In the analyzed sample, 51% of the children were exclusively breastfed. Half of the mothers were primiparous, 18.4% were under 20 years of age, and 47.6% of the mothers had 9–12 years of schooling. Regarding the working status at the moment of the interview, it was verified that 63.4% of the women interviewed in Brazil did not work outside of the home. Of those working outside of the home, 69.8% were on maternity leave.
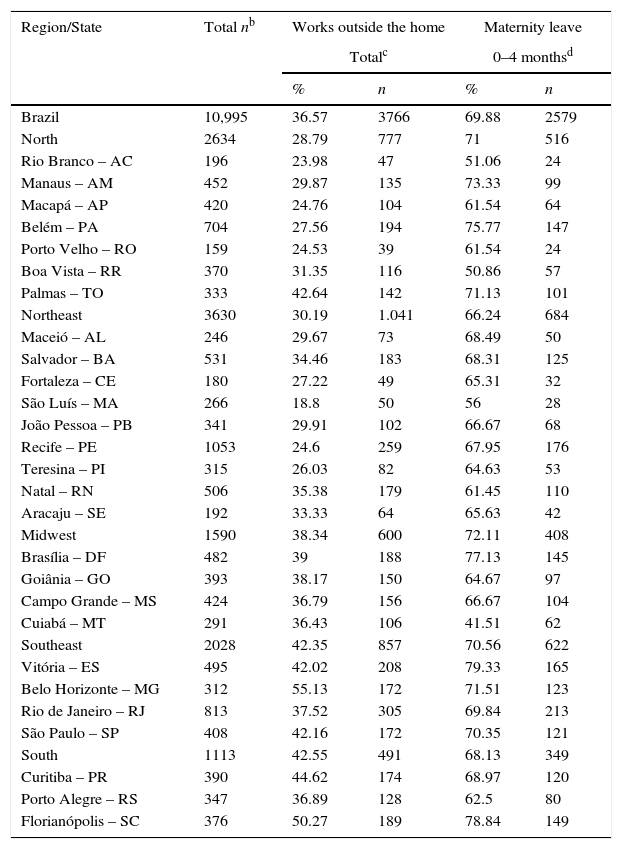
Table 1 shows the distribution of women in Brazilian capitals and in the DF regarding their working status and maternity leave. It was important to characterize the profile of women according to the working status to understand the characteristics of those who did not work outside of the home. There was a great variability among the capitals in relation to the working status at the time of the interview, and it was verified that less than 25% of the women reported working outside of the home in some of the capitals located in the North and Northeast regions. The same variability was observed in relation to the prevalence of women on maternity leave, with the Southeast and South regions showing the highest percentages of women working outside of the home.
Frequency of maternity leavea and maternal working status, stratified by Brazilian regions and by capital of each state. II Maternal Breastfeeding Prevalence Survey in the Brazilian Capitals and Federal District, 2008.
| Region/State | Total nb | Works outside the home | Maternity leave | ||
|---|---|---|---|---|---|
| Totalc | 0–4 monthsd | ||||
| % | n | % | n | ||
| Brazil | 10,995 | 36.57 | 3766 | 69.88 | 2579 |
| North | 2634 | 28.79 | 777 | 71 | 516 |
| Rio Branco – AC | 196 | 23.98 | 47 | 51.06 | 24 |
| Manaus – AM | 452 | 29.87 | 135 | 73.33 | 99 |
| Macapá – AP | 420 | 24.76 | 104 | 61.54 | 64 |
| Belém – PA | 704 | 27.56 | 194 | 75.77 | 147 |
| Porto Velho – RO | 159 | 24.53 | 39 | 61.54 | 24 |
| Boa Vista – RR | 370 | 31.35 | 116 | 50.86 | 57 |
| Palmas – TO | 333 | 42.64 | 142 | 71.13 | 101 |
| Northeast | 3630 | 30.19 | 1.041 | 66.24 | 684 |
| Maceió – AL | 246 | 29.67 | 73 | 68.49 | 50 |
| Salvador – BA | 531 | 34.46 | 183 | 68.31 | 125 |
| Fortaleza – CE | 180 | 27.22 | 49 | 65.31 | 32 |
| São Luís – MA | 266 | 18.8 | 50 | 56 | 28 |
| João Pessoa – PB | 341 | 29.91 | 102 | 66.67 | 68 |
| Recife – PE | 1053 | 24.6 | 259 | 67.95 | 176 |
| Teresina – PI | 315 | 26.03 | 82 | 64.63 | 53 |
| Natal – RN | 506 | 35.38 | 179 | 61.45 | 110 |
| Aracaju – SE | 192 | 33.33 | 64 | 65.63 | 42 |
| Midwest | 1590 | 38.34 | 600 | 72.11 | 408 |
| Brasília – DF | 482 | 39 | 188 | 77.13 | 145 |
| Goiânia – GO | 393 | 38.17 | 150 | 64.67 | 97 |
| Campo Grande – MS | 424 | 36.79 | 156 | 66.67 | 104 |
| Cuiabá – MT | 291 | 36.43 | 106 | 41.51 | 62 |
| Southeast | 2028 | 42.35 | 857 | 70.56 | 622 |
| Vitória – ES | 495 | 42.02 | 208 | 79.33 | 165 |
| Belo Horizonte – MG | 312 | 55.13 | 172 | 71.51 | 123 |
| Rio de Janeiro – RJ | 813 | 37.52 | 305 | 69.84 | 213 |
| São Paulo – SP | 408 | 42.16 | 172 | 70.35 | 121 |
| South | 1113 | 42.55 | 491 | 68.13 | 349 |
| Curitiba – PR | 390 | 44.62 | 174 | 68.97 | 120 |
| Porto Alegre – RS | 347 | 36.89 | 128 | 62.5 | 80 |
| Florianópolis – SC | 376 | 50.27 | 189 | 78.84 | 149 |
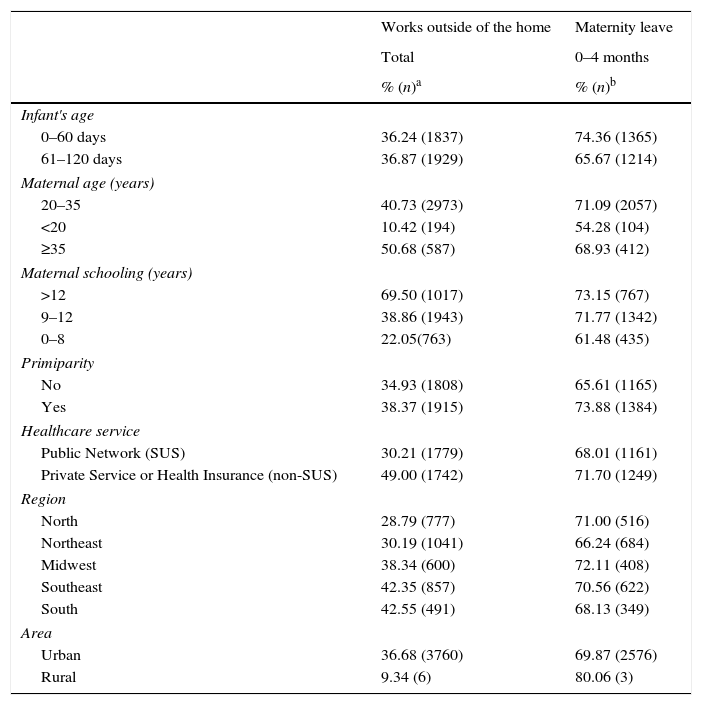
Table 2 presents the sociodemographic profile and the type of healthcare service used by the women according to their working status and maternity leave. There was a higher concentration of women working outside of the home among those older than 35 years of age, with more than 12 years of schooling, primiparous, living in the Southeast and South regions and in urban areas. It is interesting to observe the low percentage of working women who used SUS. The maternity leave frequency was higher among women aged 20–35 years, with more than 12 years of schooling, primiparous, those who had health insurance or used the private healthcare network, and those living in the Midwest and North regions.
Profile of the women according to the working status and maternity leave situation. II Maternal Breastfeeding Prevalence Survey in the Brazilian Capitals and Federal District, 2008.
| Works outside of the home | Maternity leave | |
|---|---|---|
| Total | 0–4 months | |
| % (n)a | % (n)b | |
| Infant's age | ||
| 0–60 days | 36.24 (1837) | 74.36 (1365) |
| 61–120 days | 36.87 (1929) | 65.67 (1214) |
| Maternal age (years) | ||
| 20–35 | 40.73 (2973) | 71.09 (2057) |
| <20 | 10.42 (194) | 54.28 (104) |
| ≥35 | 50.68 (587) | 68.93 (412) |
| Maternal schooling (years) | ||
| >12 | 69.50 (1017) | 73.15 (767) |
| 9–12 | 38.86 (1943) | 71.77 (1342) |
| 0–8 | 22.05(763) | 61.48 (435) |
| Primiparity | ||
| No | 34.93 (1808) | 65.61 (1165) |
| Yes | 38.37 (1915) | 73.88 (1384) |
| Healthcare service | ||
| Public Network (SUS) | 30.21 (1779) | 68.01 (1161) |
| Private Service or Health Insurance (non-SUS) | 49.00 (1742) | 71.70 (1249) |
| Region | ||
| North | 28.79 (777) | 71.00 (516) |
| Northeast | 30.19 (1041) | 66.24 (684) |
| Midwest | 38.34 (600) | 72.11 (408) |
| Southeast | 42.35 (857) | 70.56 (622) |
| South | 42.55 (491) | 68.13 (349) |
| Area | ||
| Urban | 36.68 (3760) | 69.87 (2576) |
| Rural | 9.34 (6) | 80.06 (3) |
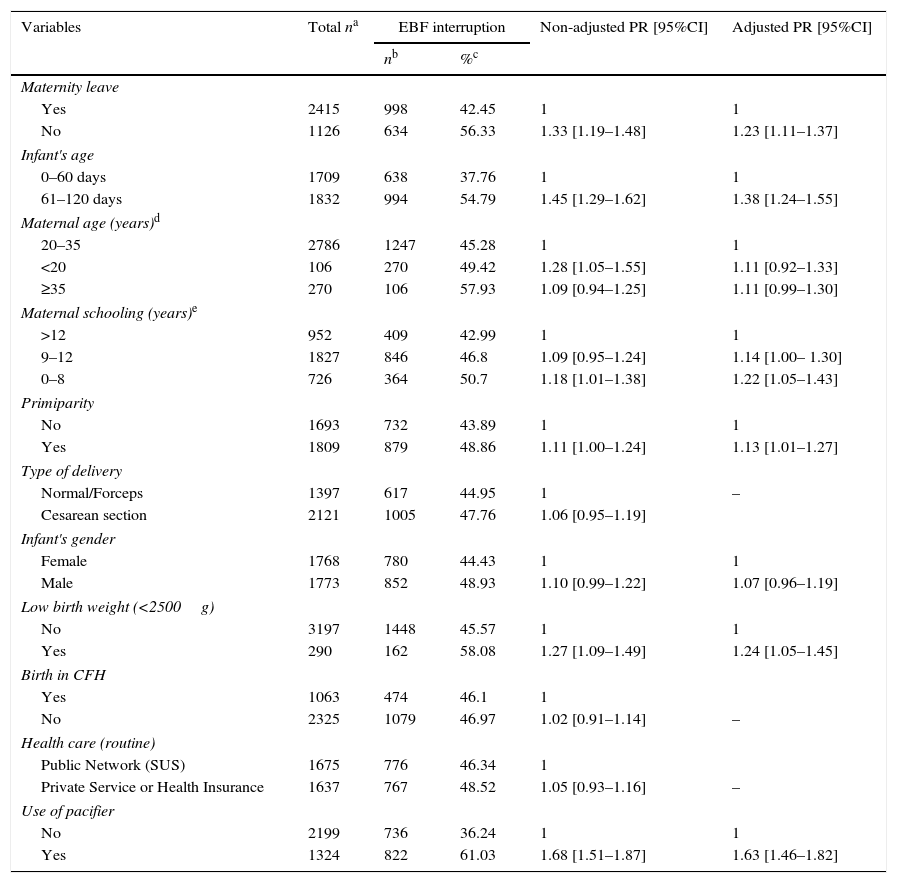
Table 3 shows the results of the gross and adjusted analysis of the association between maternity leave and EBF interruption for the working mothers’ population. For the women not in the LMAT, after adjust in all co-variables, there was an increase in the prevalence of the interruption of the AME (RP [IC95%] adjusted 1,23 [1,11 – 1,37]). Children with low birth weight who used pacifiers and children of primiparous mothers also had a greater chance of EBF interruption. Moreover, a dose–response component was observed between maternal schooling and EBF interruption, i.e., the lower the woman's educational level, the greater the risk of EBF interruption (p=0.01).
Crude and adjusted analysis by Poisson regression of exclusive breastfeeding interruption among working women and covariables. II Maternal Breastfeeding Prevalence Survey in the Brazilian Capitals and Federal District, 2008.
| Variables | Total na | EBF interruption | Non-adjusted PR [95%CI] | Adjusted PR [95%CI] | |
|---|---|---|---|---|---|
| nb | %c | ||||
| Maternity leave | |||||
| Yes | 2415 | 998 | 42.45 | 1 | 1 |
| No | 1126 | 634 | 56.33 | 1.33 [1.19–1.48] | 1.23 [1.11–1.37] |
| Infant's age | |||||
| 0–60 days | 1709 | 638 | 37.76 | 1 | 1 |
| 61–120 days | 1832 | 994 | 54.79 | 1.45 [1.29–1.62] | 1.38 [1.24–1.55] |
| Maternal age (years)d | |||||
| 20–35 | 2786 | 1247 | 45.28 | 1 | 1 |
| <20 | 106 | 270 | 49.42 | 1.28 [1.05–1.55] | 1.11 [0.92–1.33] |
| ≥35 | 270 | 106 | 57.93 | 1.09 [0.94–1.25] | 1.11 [0.99–1.30] |
| Maternal schooling (years)e | |||||
| >12 | 952 | 409 | 42.99 | 1 | 1 |
| 9–12 | 1827 | 846 | 46.8 | 1.09 [0.95–1.24] | 1.14 [1.00– 1.30] |
| 0–8 | 726 | 364 | 50.7 | 1.18 [1.01–1.38] | 1.22 [1.05–1.43] |
| Primiparity | |||||
| No | 1693 | 732 | 43.89 | 1 | 1 |
| Yes | 1809 | 879 | 48.86 | 1.11 [1.00–1.24] | 1.13 [1.01–1.27] |
| Type of delivery | |||||
| Normal/Forceps | 1397 | 617 | 44.95 | 1 | – |
| Cesarean section | 2121 | 1005 | 47.76 | 1.06 [0.95–1.19] | |
| Infant's gender | |||||
| Female | 1768 | 780 | 44.43 | 1 | 1 |
| Male | 1773 | 852 | 48.93 | 1.10 [0.99–1.22] | 1.07 [0.96–1.19] |
| Low birth weight (<2500g) | |||||
| No | 3197 | 1448 | 45.57 | 1 | 1 |
| Yes | 290 | 162 | 58.08 | 1.27 [1.09–1.49] | 1.24 [1.05–1.45] |
| Birth in CFH | |||||
| Yes | 1063 | 474 | 46.1 | 1 | |
| No | 2325 | 1079 | 46.97 | 1.02 [0.91–1.14] | – |
| Health care (routine) | |||||
| Public Network (SUS) | 1675 | 776 | 46.34 | 1 | |
| Private Service or Health Insurance | 1637 | 767 | 48.52 | 1.05 [0.93–1.16] | – |
| Use of pacifier | |||||
| No | 2199 | 736 | 36.24 | 1 | 1 |
| Yes | 1324 | 822 | 61.03 | 1.68 [1.51–1.87] | 1.63 [1.46–1.82] |
PR, prevalence ratio; CFH, Child-Friendly Hospital; SUS, Brazilian Unified Health System.
This is the first study of national scope that assesses the association between maternity leave and EBF prevalence and presents the results according to Brazilian regions and capitals, based on the data obtained in the II PPAM, in the Brazilian Capitals and Federal District, held in 2008 by the Ministry of Health.
A large variability was observed in relation to the prevalence of women on maternity leave; the Southeast and South regions showed the highest percentages of women working outside of the home. The increase in women's participation in the labor market in regions of high industrial concentration are aspects that have been observed in studies carried out in high and middle-income countries. Between 1960 and 2009, there was an increase in this participation, from 32% to 46% in the United States, from 25% to 47% in Canada, and from 21% to 41% in Latin America and the Caribbean.13,14 In Brazil, in 1996, approximately 21% of Brazilian households had a female head of the family, and in 2012, 37.4% of the families had a woman in charge of the household.18
Among working mothers, it was observed that those on maternity leave had a lower chance of EBF discontinuation in the first four months of the infant's life, after adjusting for other factors indicated in other studies as determinants or associated to EBF, such as maternal level of schooling, parity, low birth weight, and pacifier use.4–8,19
Corroborating the present findings, a study carried out by Venâncio et al.20 in 77 municipalities in the state of São Paulo also showed a higher percentage of EBF among mothers who were on maternity leave (54.6%) and a lower percentage (25.6%) among those who were working without maternity leave. Similarly, Vianna et al.,21 in a study carried out in 70 municipalities in the state of Paraíba, verified that maternity leave positively influenced the prevalence of EBF. A North-American study carried out by Mirkovic et al.,22 who analyzed the influence of maternity leave duration and working hours on breastfeeding duration, found that returning to work before 3 months of postpartum on a full-time basis reduced the chance of women reaching the period they had declared as being their intention to breastfeed. It is worth mentioning that studies have demonstrated the influence of maternity leave on the total duration of breastfeeding,23 in addition to benefits related to the reduction in infant mortality rates.24,25
The adoption of strategies and legislations to protect working women who breastfeed has been emphasized in several documents by international organizations, such as the Innocenti Declaration on Protection, Promotion, and Support of Breastfeeding (1990) and the Global Strategy for Infant and Young Child Feeding in Early Childhood.26 The Brazilian Ministry of Health has developed some strategies, such as the Breastfeeding Program Support for Working Women, which aims to stimulate managers of public and private companies to adhere to the six-month maternity leave, having a daycare at the workplace and a breastfeeding support room. Although Brazil has stood out in the international scenario as one of the countries that offers the longest maternity leave in weeks and the highest percentage of wages paid to the women,27 the seventh in a ranking of 202 countries surveyed by the United Nations, further actions are still required.
Breastfeeding among working women is a complex subject and permeated by many choices, often requiring more than employee benefits for the continuation of EBF.28 Several authors point out that EBF rates vary worldwide and that postpartum support technologies, such as breastfeeding support at workplaces, breaks during working hours for breastfeeding, maternity leave, and professional counseling and lactation management during this transition period of returning to work are positive factors for breastfeeding stimulation.29
Some study limitations are noteworthy. Secondary data were used, and the set of variables available was used to construct the model. Nonetheless, important variables pointed out in the literature related to the mother and child were included.30 Due to the cross-sectional design, the results shown here may be useful to formulate hypotheses and not to establish a causal association. In this sense, the authors verified that maternity leave can influence the duration of the EBF, but longitudinal studies are necessary to confirm this hypothesis. The data analyzed here were collected in 2008 and, thus, there is a temporal distance from the present, but there are no data of national scope on the subject, emphasizing the importance of this research.
It was observed that maternity leave is associated with an increase in the prevalence of EBF in the Brazilian capitals and the DF, reinforcing the importance that government and society offer strategies to encourage breastfeeding, such as the universal increase of maternity leave from 4 to 6 months.23,29 The result of this study may influence decisions that will benefit thousands of Brazilian women with the increase of maternity leave.
FundingThe data analyzed in the article were extracted from the II PPAM, carried out in 2008 and funded by the Brazilian Ministry of Health.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Monteiro FR, Buccini GS, Venâncio SI, Costa TH. Influence of maternity leave on exclusive breastfeeding. J Pediatr (Rio J). 2017;93:475–81.





