
To evaluate the impact of the chronic kidney disease (CKD) on quality of life, from the children's and their parents’ perspective, respiratory muscle strength, lung function, and functional capacity in children and adolescents.
MethodCross-sectional study of children with CKD aged 8 to 17 years. Those incapable of taking the tests were excluded. After an interview, quality of life by Pediatric Quality of Life Inventory) (PedsQLTM), muscular strength, pulmonary function tests, and the 6-minute walking test (6MWT) were applied. Student's t-test, ANOVA (difference in means), and Pearson's coefficient of correlation were used. The level of significance was set at 5%.
ResultsOf the 40 patients, the mean distance walked at the 6MWT was 396 meters, and the mean final score at the quality of life test as perceived by the children and parents was 50.9 and 51, respectively. From the children's perspective, the transplanted patients had a higher quality of life score when compared to those undergoing hemodialysis (p<0.001); those who practiced physical activity had better quality of life when compared to the sedentary children (p<0.001). From the children's and the parents’ perspectives, the male gender had a higher quality of life score (p<0.05). There was a positive correlation between the distance walked at the 6MWT and age, height, final PedsQLTM, forced vital capacity (FVC), and forced expiratory volume in the first second (FEV1), as well as a negative correlation between FEV1/FVC and the distance walked.
ConclusionA significant reduction in the quality of life and the functional capacity was observed in children with CKD, influenced by the type of treatment, gender, and sedentary life style.
Avaliar repercussões da doença renal crônica (DRC) sobre a qualidade de vida na percepção das crianças e dos pais, força muscular respiratória, função pulmonar e capacidade funcional em crianças e adolescentes.
MétodoEstudo transversal de crianças e adolescentes com DRC de oito a 17 anos. Excluídas as incapazes de realizar os testes. Após entrevista, aplicou-se questionário de qualidade de vida (PedsQLTM), testes de força muscular, função pulmonar e teste de caminhada de 6 minutos (TC6min). Foi utilizado o teste t de Student e ANOVA (diferenças de médias) e o coeficiente de correlação de Pearson. Considerou-se nível de significância de 5%.
ResultadosDentre os 40 pacientes, a média da distância percorrida no TC6min foi de 396±71 metros, e a média do escore final de qualidade de vida percebida pelas crianças e pelos pais de 50,9 e 51, respectivamente. Na percepção das crianças, os transplantados apresentaram maior escore de qualidade de vida, comparados aos em hemodiálise (p<0,001), e aos com atividade física e melhor qualidade de vida, comparadas às sedentárias (p<0,001). Na percepção das crianças e dos pais, o sexo masculino apresentou maior escore de qualidade de vida (p<0,05). Houve correlação positiva entre a distância percorrida no TC6min e as variáveis idade, altura, PedsQLTM final da criança, capacidade vital forçada (CVF) e volume expiratório forçado no primeiro segundo (VEF1) e negativa entre VEF1/CVF e a distância percorrida.
ConclusãoObservou-se redução significativa na qualidade de vida e na capacidade funcional em crianças com DRC influenciadas pelo tipo de tratamento, sexo e sedentarismo.
Chronic renal failure (CRF) is characterized by slowly progressive, irreversible loss of kidney function.1 In children, chronic kidney disease (CKD) is associated with significant cardiovascular morbidity and mortality, hospitalizations, and common specific problems, such as impaired growth and biopsychosocial changes that have an impact on quality of life (QoL).2
Data from the Brazilian Society of Nephrology in 2012 showed that 0.3% of children with CKD aged 1 to 12 years and 4.2% between 13 and 18 years undergo dialysis.1 In recent years, the number of patients on dialysis has doubled, with an increase of 8% per year, increasing from 18,000 patients in 2001 to 91,314 in 2011, resulting in significant healthcare costs.3
Studies have shown that children and adolescents with CKD may have alterations in QoL, muscle strength, lung function, and functional capacity.4,5
The assessment of health-related QoL is an important criterion when evaluating the effectiveness of treatments and interventions in healthcare, making it important to understand the existing association between the disease and QoL.6 Goldstein et al.,7 in 2008, developed the PedsQLTM questionnaire to specifically assess QoL in children and adolescents with CKD. This questionnaire assesses seven domains (general fatigue, kidney disease, treatment, interaction with family and friends, worry, physical appearance, and communication), and is applied to patients with CKD and their parents or guardians. Studies on QoL using the PedsQLTM have verified the impact of CKD on QoL of children and adolescents.7,8
The PedsQLTM version 3.0 was translated and culturally adapted into Brazilian Portuguese in 2011,9 but there are no published studies on its validation in Brazil.
The reduction in functional capacity and performance of physical and recreational activities can be influenced by physical deconditioning, muscle disuse atrophy, weakness, fatigue, lower-limb edema, and back pain, among others, hindering the performance of daily living activities by these children.10,11 Other factors may impair the muscular system of CKD patients, such as decreased protein-calorie intake and protein imbalance. The respiratory muscles may show decreased strength and endurance properties due to uremic myopathy.12–14
Respiratory muscle strength measurement aids in the early identification of muscle weakness, as well as identification of the severity, functional consequences, and evolution of pulmonary and neuromuscular disorders.15,16 A study has demonstrated that children and adolescents with CKD have significantly lower muscular strength values, when compared to healthy subjects.4
Walking tests are submaximal tests used in the assessment of functional capacity of children with physical exertion limitations. They are easy to perform, reproducible, low-cost, and show good correlation with the maximum oxygen consumption obtained at maximal exercise tests.17–19 A study has demonstrated that children with CKD have lower functional capacity when compared to healthy children.19
The present study aimed to evaluate the impact of CKD on QoL from the children's and their parents’ perception, respiratory muscle strength, pulmonary function, and functional capacity in children and adolescents.
MethodsThis was an observational cross-sectional study with children and adolescents with CKD, treated at the Pediatric Nephrology Unit of the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), in Pernambuco, which is a reference center for kidney disease and transplantation in Northeast Brazil.
The study was approved by the Ethics Committee on Human Research of IMIP (No. 3334-13), and those responsible for the children and adolescents signed AN informed consent before the study was initiated.
Children and adolescents, aged 8 to 17 years and with CKD, and one of their parents were included. Children incapable of performing the six-minute walk test (6MWT), those with difficulties in understanding directions to perform the maneuvers, and patients with complex congenital heart disease and severe pulmonary disease were excluded. Data collection was performed from December 2012 to April 2013.
Initially, demographic, anthropometric, and clinical data were recorded on standardized investigation forms containing the variables of interest for the study. Educational delay was defined as regular age-grade correspondence > two years, according to the criteria adopted by the Brazilian Ministry of Education; family income was calculated by the sum of individual incomes of the household's residents. The level of physical activity was assessed through the Habitual Level of Physical Activity (HLPA) questionnaire as sedentary lifestyle, regular physical activity (up to 2hours a week), and competitive/organized sports physical activity (more than 2hours a week).20 The type of treatment was categorized as conservative, peritoneal dialysis, hemodialysis, and renal transplantation.
Subsequently, the PedsQLTM QoL questionnaire was applied, after authorization of use by the MAPI Research Trust, responsible for the permissions to use the questionnaire, followed by lung function and respiratory muscle strength assessment and the 6MWT. The tests were conducted by the main researcher and an appropriately trained physical therapy student.
Quality of lifeQoL assessment was performed by applying the PedsQLTM questionnaire (version 3.0).9 It consists of 34 questions grouped into seven items comprising health-related perception in the areas of general fatigue, kidney disease, treatment, interaction with family and friends, worry, physical appearance, and communication, as perceived by parents and the children/adolescents. Values range from 0 to 4, with 0 representing “it is never a problem;” 1, “it is almost never a problem;” 2, “it is sometimes a problem;” 3, “it is often a problem;” and 4, “it is almost always a problem.” The questions are converted into scores, for which values are proportionally assigned, the sum ranges from 0 to 100 points. The higher the value of the final score, the better the QoL of patients.
Strength and lung functionMaximal respiratory pressures were measured through manovacuometry, using an analog manovacuometer (Comercial Médica®, São Paulo, Brazil). The test was performed with the child sitting comfortably to measure the maximal inspiratory pressure (MIP) through an inspiratory maneuver based on the functional residual capacity, whereas maximal expiratory pressure (MEP) was evaluated based on total lung capacity for a forced expiration, after clipping the nose. For both measures, three maneuvers were performed and the best of the three was chosen using the technique based on Wilson's study.21
Lung function assessment was performed by spirometry using a digital spirometer OneFlow® model (Clement Clarke International; Harlow, UK) and technical procedures, criteria for acceptability, and reproducibility followed the guidelines of the American Thoracic Society and European Respiratory Society (ATS/ERS).22 The forced expiratory volume in one second (FEV1), forced vital capacity (FVC), peak expiratory flow (PEF), and FEV1/FVC ratio were determined. The maneuver was performed three times and the highest value was used.
6-Minute Walking TestSubmaximal functional capacity was evaluated using the 6MWT according to the ATS standardization,22 on a flat, 30-meter corridor. The children/adolescents were instructed to walk as far as possible in six minutes without running, and the test could be interrupted at any time. The children/adolescents were verbally encouraged, minute-by-minute, according to the test standardization, and after six minutes they were asked to stop where they were in order to record the distance walked in meters. The parameters evaluated pre- and post-test included heart rate (HR) and pulse oxygen saturation (SpO2) by pulse oximetry model OXP-10 (EMAI Equipamentos Médicos Hospitalares, São Paulo, Brazil), systemic blood pressure through a sphygmomanometer model CE0050 (Tycos/WelchAllyn, Skaneateles Falls, USA), respiratory rate (RR) (counted by chest wall incursions per minute), and the modified Borg scale score to measure dyspnea.23
The criteria for test interruption were: severe dyspnea or fatigue expressed by the patient, SpO2<85%, or refusal to continue the examination. Based on the reference values suggested by Priesnitz et al.24 for healthy children, the predicted walked distance at the 6MWT for the children was calculated using the formula 6MWT=145.343+[11.78 x age (years)]+[292.22 x height (m)]+[0.611 x (HRFinal - HRInitial)] - [2,684 x weight (kg)] to evaluate test performance. This reference was used because it is from a study on healthy Brazilian children. Based on these values, the difference of means between the distance walked by the patient at the 6MWT (WD) and the predicted distance (PD) was obtained.
Values were expressed as means and their standard deviations for quantitative variables. The Kolmogorov-Smirnov test was used to ensure normality for quantitative variables. Student's t-test was used to verify whether the two groups differed significantly based on the comparison of their means, and ANOVA was used for the comparison of more than two groups. Student's t-test was used for comparison of paired means. Pearson's correlation coefficient was used to assess correlation. Data were analyzed in SPSS 13.0 for Windows (IBM Corp, Armonk, USA) and Excel 2007 (Microsoft, Microsoft Excel,Washington, USA). A significance level of 5% was used in all tests.
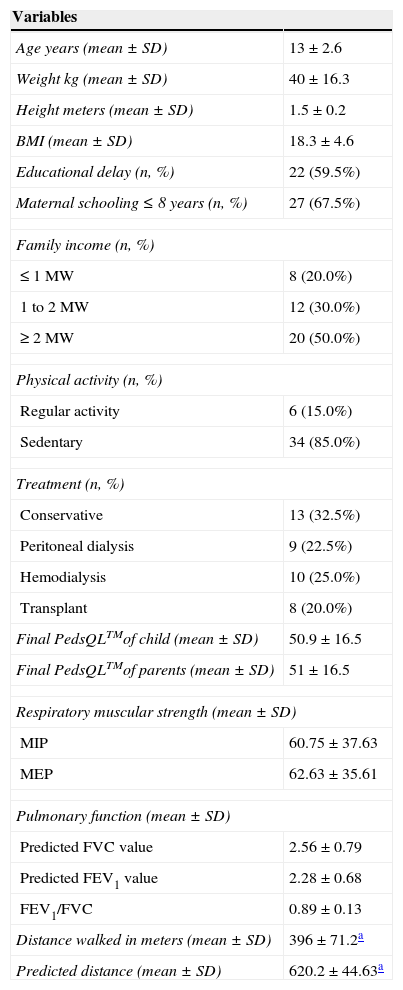
ResultsOf the total 127 children and adolescents with CKD treated at the Pediatric Nephrology Unit of IMIP, 40 were included in the study and 87 were excluded (31 due to incapacity to perform the 6MWT, 46 due to difficulties in understanding how to perform the respiratory tests, and ten for having complex heart disease or severe chronic lung disease). Of the 40 eligible patients, the mean age±SD was 13±2.6 years, 52.5% were males, 59.5% had educational delay, and 85% did not practice any physical activity. The mean final QoL score was 50.9±16.5 for the children and 51±16.5 for the parents. The mean walked distance in meters at the 6MWT was 396±71, whereas the mean walked distance predicted by the formula was 620.2±44 meters, with a significant difference (p<0.001), representing 63.7% of the predicted values (Table 1).
Characteristics of 40 children with chronic kidney disease treated at a referral center for pediatric nephrology, 2013, Brazil.
| Variables | |
|---|---|
| Age years (mean±SD) | 13±2.6 |
| Weight kg (mean±SD) | 40±16.3 |
| Height meters (mean±SD) | 1.5±0.2 |
| BMI (mean±SD) | 18.3±4.6 |
| Educational delay (n, %) | 22 (59.5%) |
| Maternal schooling ≤ 8 years (n, %) | 27 (67.5%) |
| Family income (n, %) | |
| ≤ 1 MW | 8 (20.0%) |
| 1 to 2 MW | 12 (30.0%) |
| ≥ 2 MW | 20 (50.0%) |
| Physical activity (n, %) | |
| Regular activity | 6 (15.0%) |
| Sedentary | 34 (85.0%) |
| Treatment (n, %) | |
| Conservative | 13 (32.5%) |
| Peritoneal dialysis | 9 (22.5%) |
| Hemodialysis | 10 (25.0%) |
| Transplant | 8 (20.0%) |
| Final PedsQLTMof child (mean±SD) | 50.9±16.5 |
| Final PedsQLTMof parents (mean±SD) | 51±16.5 |
| Respiratory muscular strength (mean±SD) | |
| MIP | 60.75±37.63 |
| MEP | 62.63±35.61 |
| Pulmonary function (mean±SD) | |
| Predicted FVC value | 2.56±0.79 |
| Predicted FEV1 value | 2.28±0.68 |
| FEV1/FVC | 0.89±0.13 |
| Distance walked in meters (mean±SD) | 396±71.2a |
| Predicted distance (mean±SD) | 620.2±44.63a |
Values expressed as mean and standard deviation (SD) and numbers (n) and percentage (%). BMI, body mass index; MW, minimum wage; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; PedsQLTM, quality of life questionnaire.
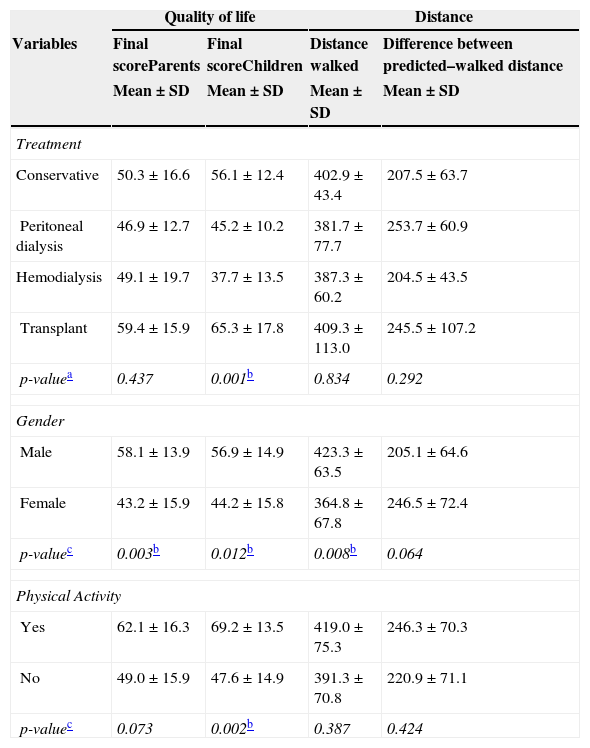
When comparing QoL and the type of treatment, it was observed that transplanted patients had the highest scores (65.3) when compared to the group submitted to hemodialysis (37.7; p<0.001) from the children's perception. Additionally, there was a significant association between QoL and gender from the parents’ and children's perception, where males had a better final QoL score (58.1 and 56.9, respectively). Regarding QoL and physical activity, it was observed that those who performed regular physical activity had a better QoL when compared to sedentary individuals (p=0.002) from the children's perception.
Comparing the means between the walked distance and the gender of the child, it was observed that the distance walked by males was higher than females (p=0.008) (Table 2).
Comparison of means of quality of life, walked distance, and difference between the predicted and the walked distance, subdivided by type of treatment, gender, and physical activity in children and adolescents with chronic kidney disease.
| Quality of life | Distance | |||
|---|---|---|---|---|
| Variables | Final scoreParents | Final scoreChildren | Distance walked | Difference between predicted–walked distance |
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | |
| Treatment | ||||
| Conservative | 50.3±16.6 | 56.1±12.4 | 402.9±43.4 | 207.5±63.7 |
| Peritoneal dialysis | 46.9±12.7 | 45.2±10.2 | 381.7±77.7 | 253.7±60.9 |
| Hemodialysis | 49.1±19.7 | 37.7±13.5 | 387.3±60.2 | 204.5±43.5 |
| Transplant | 59.4±15.9 | 65.3±17.8 | 409.3±113.0 | 245.5±107.2 |
| p-valuea | 0.437 | 0.001b | 0.834 | 0.292 |
| Gender | ||||
| Male | 58.1±13.9 | 56.9±14.9 | 423.3±63.5 | 205.1±64.6 |
| Female | 43.2±15.9 | 44.2±15.8 | 364.8±67.8 | 246.5±72.4 |
| p-valuec | 0.003b | 0.012b | 0.008b | 0.064 |
| Physical Activity | ||||
| Yes | 62.1±16.3 | 69.2±13.5 | 419.0±75.3 | 246.3±70.3 |
| No | 49.0±15.9 | 47.6±14.9 | 391.3±70.8 | 220.9±71.1 |
| p-valuec | 0.073 | 0.002b | 0.387 | 0.424 |
Values expressed as mean and standard deviation (SD).
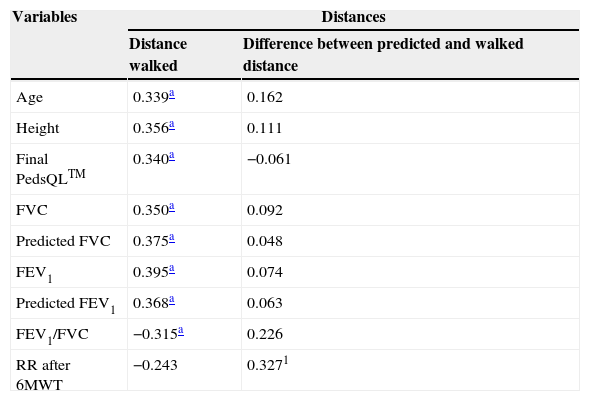
When analyzing the correlation between the distance walked in the 6MWT and the study variables, there was a significant positive correlation, i.e., the higher the values of the variables, the better the test performance regarding variables age, height, final PedsQLTM, FVC, predicted FVC, FEV1, and predicted FEV1. A negative correlation between FEV1/FVC and the walked distance was also observed, that is, the higher the ratio, the lower the test performance. The respiratory rate evaluated after the 6MWT showed a positive correlation with the difference between the walked and the expected distance (Table 3). The other variables analyzed in this study showed no significant correlation.
Correlation between the walked distance, difference between the predicted and the walked distance, and study variables in children with chronic kidney disease.
| Variables | Distances | |
|---|---|---|
| Distance walked | Difference between predicted and walked distance | |
| Age | 0.339a | 0.162 |
| Height | 0.356a | 0.111 |
| Final PedsQLTM | 0.340a | −0.061 |
| FVC | 0.350a | 0.092 |
| Predicted FVC | 0.375a | 0.048 |
| FEV1 | 0.395a | 0.074 |
| Predicted FEV1 | 0.368a | 0.063 |
| FEV1/FVC | −0.315a | 0.226 |
| RR after 6MWT | −0.243 | 0.3271 |
PedsQLTM, quality of life questionnaire; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; RR, respiratory rate.
The present study demonstrates that children and adolescents with CKD have a significant reduction in QoL and functional capacity. This study used the PedsQLTM QoL questionnaire version 3.0, as it is specific for children and adolescents with CKD, and is probably more sensitive to detect possible alterations in the health of these patients. In addition, the authors did not find studies in the literature associated to better QoL as perceived by parents of children and adolescents with CKD that had used the PedsQLTM.
In this study, the mean final QoL score perceived by the children was 50.9, a significantly lower result when compared to those recorded by Goldestein et al.,7 in a study performed in the United States (72.5), and by Park et al.,8 in Korea (69.4). The lower score in the present study may be due to the fact that the evaluated children had low socioeconomic status.
A better QoL in renal transplant patients compared to those on hemodialysis in the present study was also reported in a study conducted in Korea involving 92 children with CKD.8 Another study in Texas with 186 children and adolescents with CKD demonstrated that, in addition to better QoL, children submitted to renal transplantation had improved survival. This fact is justified by the authors for the high risk of complications in patients undergoing peritoneal dialysis and hemodialysis.5
Higher scoring in the final QoL score as perceived by male children and adolescents was also demonstrated for the perception of adolescents aged 15 to 18 years with CKD in a study by Maxwell et al.25
Better scoring in the final QoL score according to the perception of children that practiced physical activity was also observed by other authors. Akber et al.26 evaluated the level of physical activity through the use of pedometers in patients aged 7 to 20 years with CKD and observed that low levels of physical activity in this age group were associated with higher cardiovascular risks. The researchers also stated that low levels of physical activity were associated with poorer physical performance and worse self-reported QoL.26
Patients with CKD may have muscle dysfunction due to interrelated factors, such as decreased protein-calorie intake, muscle disuse atrophy, and protein imbalance. These factors lead to changes in type II muscle fibers and reduction of the capillary vascular bed, intravascular presence of calcification, and reduction of local blood flow, thus contributing to muscle alterations.27
Discordant data to those of the present study refer to muscle strength. The study by Coelho et al.4 in Minas Gerais, involving 30 children with CKD, found lower values in maximal expiratory pressure.
When assessing pulmonary function, a positive correlation was observed between FVC and FEV1 with functional capacity. Children with better vital capacity and FEV values showed better performance at the 6MWT, suggesting the influence of these variables on the test. In children with CKD, a decrease in spirometric variables is related to reversible airway obstruction and air trapping caused by accumulation of fluid near the small airways.28 A study conducted in France also demonstrated that children with CKD may have airflow limitation, where the reduction in FEV1 may be associated with decreased muscle strength, responsible for the delay in skeletal muscle fiber contraction.29
The positive correlation found between the final respiratory rate and the difference between the walked and predicted distances indicates worse performance at the test. This is consistent with a study of 30 children and adolescents with CKD, where an association was observed between shorter walked distance and an increase in the final respiratory rate, blood pressure, pulse oxygen saturation, and Borg perceived exertion, thus suggesting a worse performance in functional activities.4
Functional capacity assessed by the mean walked distance at the 6MWT found in the present study (396±71.2 meters) was lower than that observed in other studies, whose mean walked distances ranged from 515 to 560 meters. However, in all these studies, the values were significantly lower than those predicted.4,18,26 Several anthropometric, clinical, and biological factors can influence children with CKD to have poorer performance in physical activities, such as maternal education, body mass index (BMI), height, and age. A study demonstrated that children of mothers with higher educational level were more active when compared to children of less educated mothers.30
Regarding the correlations between walked distance and variables of interest in the study, it was observed that the older the children and adolescents were, the better their performance at the 6MWT, indicating better functional capacity. Another study also found a positive correlation between age and walked distance, demonstrating that the older the age, the better the functional capacity.26
Regarding the correlation between functional capacity assessed by the 6MWT, it can be observed that taller patients walked a significantly greater distance when compared with healthy children. A Belgian study of 25 children with CKD observed that height is an important factor for the distance walked during the 6MWT, explained by the fact that taller individuals have greater stride length and better performance at the test.18
Regarding gender, male individuals showed better performance at the 6MWT. The present data are consistent with a study conducted in China, which found higher exercise capacity and better performance at the 6MWT in healthy male children, probably as a result of their greater muscle mass.17 Conversely, a U.S. study with 44 participants assessed physical activity in CKD patients aged 7 to 20 years, and observed that females walked a greater distance than males in the 6MWT.26
The positive correlation between distance walked and QoL perceived by the children demonstrated that the greater the distance walked, the better the score; however, the authors did not find other studies related to these findings in the literature.
Despite the importance of this study, some limitations need to be highlighted, such as the sample size, which may not have had sufficient power to demonstrate all the studied differences, such as respiratory muscle strength. However, all eligible children with CKD from the Nephrology Pediatric Center of IMIP were included. It is noteworthy, however, that this study is the in Brazil to evaluate QoL through PedsQLTM in children and adolescents with CKD.
Finally, it is concluded that the study sample showed a significant reduction in QoL, functional capacity, and physical activity in children and adolescents with CKD. Positive associations were also found between functional capacity, pulmonary function, and QoL. However, no correlation was found between respiratory muscle strength and functional capacity, suggesting the need for new studies to better elucidate this finding.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Teixeira CG, Duarte MC, Prado CM, Albuquerque EC, Andrade LB. Impact of chronic kidney disease on quality of life, lung function, and functional capacity. J Pediatr (Rio J). 2014;90:580–6.
Study performed at Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Recife, PE, Brazil.





