

This study aimed to determine the influence of breastfeeding on the intellectual capacity of children from a cohort in a developing country, with a control for the main confounding factors.
MethodsA prospective cohort study was performed including all infants born in the hospitals of a medium-size city, and a random sample of these newborns was monitored at 30, 90, and 180 days of life, and at age 8 years. Several aspects of breastfeeding were assessed in the follow-up and, at 8 years, general intellectual capacity was assessed through the Raven's Colored Progressive Matrices test. The statistical analyses used Student's t-test, ANOVA, and linear regression and logistics, considering p-values less than 0.05 as statistically significant associations.
ResultsAt age 8 years, 560 children were assessed with Raven's Colored Progressive Matrices test. The average score was 22.56 points, with a standard deviation of 5.93. The difference in the averages found between the breastfed and non-breastfed groups at six months of age was 1.33 (p=0.008). Mother's and child's skin color, social and economic class, maternal education and smoking, and breastfeeding at six months of age (p=0.007) were still associated with the outcome.
ConclusionsChildren that were breastfed for six months or more had better performance in the general intellectual assessment, even after adjusting for the main confounding factors.
O objetivo deste estudo foi determinar a influência do aleitamento materno na capacidade intelectual de crianças pertencentes a uma coorte de um país em desenvolvimento, controlando para os principais fatores de confusão.
MétodosFoi realizado um estudo de coorte prospectiva com todos os recém-nascidos nos hospitais de uma cidade de porte médio e acompanhou-se uma amostra aleatória destes aos 30, 90 e 180 dias de vida e aos 8 anos. No acompanhamento foram avaliados diversos aspectos da amamentação e, aos 8 anos, foi realizada avaliação da capacidade intelectual geral aplicando-se o Teste de Raven. As análises estatísticas utilizaram Teste T, ANOVA e regressão linear e logística, considerando como associações estatisticamente significativas aquelas cujo valor de p foi inferior a 0,05.
ResultadosAos 8 anos 560 crianças participaram da avaliação com o Teste de Raven. A média da pontuação das crianças no teste foi de 22,56 pontos com desvio padrão de 5,93. A diferença de médias entre os grupos em aleitamento materno ou não, aos seis meses, foi de 1,33 (p=0,008). Permaneceram associadas ao desfecho, após regressão linear e logística, a cor materna e da criança, classe socioeconômica, escolaridade e tabagismo maternos e o aleitamento materno aos 6 meses de idade (p=0,007).
ConclusõesAs crianças que mamaram por seis meses ou mais tiveram melhor desempenho na avaliação intelectual geral, mesmo após ajuste para os principais fatores de confundimento.
Breastfeeding (BF) has clear short-term benefits for children's health, as the reduction in morbidity and mortality due to infectious diseases.1–3 However, there is still some controversy on its long-term consequences. In 2007, the World Health Organization (WHO) published a systematic review and meta-analysis that assessed the long-term benefits of BF. The authors concluded that BF may contribute to intellectual development, but they suggest that only long-term observations can provide a more accurate estimate of the impact of BF on cognitive development.4
A literature review published by Jain et al. in 2002 tried to determine the extent of the positive effects of BF on the intellect.5 The research retrieved 40 publications and, of these, 68% concluded that BF promotes intelligence, but many studies showed methodological flaws. Only two with term newborns presented good quality and, of these, only one concluded that the effect of BF on intelligence was significant.
Cognitive performance is a complex process influenced by several genetic and environmental factors that interact with each other, and BF is most likely one of these factors.6 A critical process in neural development is myelination, which is very rapid in the first two years after birth and, thereafter, continues at a slower pace throughout childhood and adolescence.7 Arachidonic acid (AA) and docosahexaenoic acid (DHA) are important lipid components for the development of cell membranes, mainly retinal and central nervous system cells. These long-chain fatty acids are present in breast milk, but not in most infant formulas.8 AA and DHA accumulate in the brain and retina faster during the last trimester of pregnancy and in the first months after birth.4
Infants need enough stimulation and predictability in their environment to maximize the initial period of rapid brain growth and neuroplasticity. An improper diet or a significant lack of stimulation – mainly verbal stimulation – during the first months may result in negative effects on the child's future cognitive progress.7 In addition to chemical effects, BF increases mother-baby bonding, which may contribute to the infant's intellectual development.4
There is strong evidence in the literature,4,9 albeit inconclusive, that BF promotes cognitive performance. Randomized studies are not feasible from an ethical point of view, making it difficult to prove this association. The vast majority of studies have been performed in developed countries; studies to verify this association are still scarce in developing countries. This study aimed to assess, in a birth cohort, the relationship between BF and intellectual performance of 8-year-old children.
MethodsA prospective cohort study was performed including all infants born in all hospitals of the city of Pelotas, Rio Grande do Sul, Brazil, from September, 2002 to May, 2003; a random sample of 30% of these infants was followed-up at 30, 90, and 180 days old and at 8 years old. All newborns whose mothers lived in the urban area of Pelotas and had no contraindication to BF (such as severe infant malformations or HIV-positive mother) were included in the study. As the initial purpose of the cohort study was to assess the aspects of BF, newborns that needed hospitalization immediately after birth and were more than 24hours away from their mothers were excluded.
The initial cohort sample was based on a 95% confidence level and on an 80% statistical power for exposures ranging between 15% and 80%, and an increase of 15% in the initial sample was estimated for possible losses and control of potential confounding factors. For the associations assessed at age 8 years, a subsequent calculation was performed, showing the need for a 436-child sample. The research project was approved by the Ethics Committee of the Universidade Católica de Pelotas, and mothers or guardians signed an informed consent.
When visiting the eight-year-old children, the authors tried to locate children residing in Pelotas or that had moved to neighboring municipalities using data obtained in the last visit (address or telephone), searches in the information system of the Municipal Emergency Room and in the admission control system of the of the largest hospital of the city, in addition to searches on the Internet, social networks, and on a list of students enrolled in municipal schools. Children that were not located either after three attempts at the last visit address or using the strategies described above were deemed losses. Children clinically diagnosed with mental handicaps, with syndromes that may lead to developmental delay (children that were not able to perform the test), or with severe clinical complications preventing the assessment of intelligence were excluded from the development assessment. The located sample was compared with the original sample, and no statistically significant difference was found between the intended and the available samples.
Independent variables were obtained through collection of data from maternal medical records, and also through a standardized questionnaire applied to mothers or caregivers by trained interviewers during home visits. The socioeconomic class was defined pursuant to the classification of the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa – ABEP).10 Household income was reported by the interviewee in Reais, parental education was considered in terms of complete years of study, and parental age was reported in full years of life. Skin color was assessed through interviewer description as white or non-white. Maternal and partner smoking was reported by the interviewee. Data on gender of child, skin color, number of siblings, birth weight, and gestational age were obtained from maternal medical records when the child was born. The gestational age was obtained through the best data available in the records (last menstrual period, obstetric ultrasound, or pursuant to the physical characteristics of the newborn [Capurro Method]), and was further categorized into premature (<37 weeks) and term newborn (≥ 37 weeks). Birth weight was categorized into low weight (<2,500g) and normal (≥ 2,500g). Data on BF were collected in all visits and the BF variable was analyzed pursuant to its duration and the categories recommended by the WHO;11 BF at six months was considered as any breast milk intake, either directly from breast or extracted, regardless of the intake of any other food or liquid, including non-human milk. The interviewers were medical students.
In order to assess general intellectual capacity, Raven's Colored Progressive Matrices12 test was used and adapted to the Brazilian context. This test is indicated to assess intellectual development in school, in clinical diagnoses, and in anthropological and intercultural studies. It is comprised by three series of 12 items: A, Ab, and B. The items are arranged in an ascending order of difficulty in each series, and each series is more difficult than the previous one. Items are comprised by a drawing or matrix with a part missing, below which six alternatives are presented, one of which correctly completes the matrix. The examinee must choose one of the alternatives to complete the missing part.13 The test was applied individually during a second home visit for this purpose, and the answers were written down by the interviewer in standardized answer sheets. Raw scores obtained by the children in the test (ranging from 1 to 36 correct answers) were considered in the analysis. This score was transformed into a percentile pursuant to a reference table for correction in the test manual,12 where percentile ≤ 5 signifies intellectual deficiency; between 6 and 25, below-average intellectual capacity; between 26 and 74, average intellectual capacity; between 75 and 94, above-average intellectual capacity; and higher than 95, superior intellectual capacity. Subsequently, they were categorized into three groups: percentile ≤ 25, below-average or intellectual deficiency; 26 ≤ percentile ≤ 74, average intellectual capacity; and percentile ≥ 75, above-average or superior intellectual capacity. The tests were applied by psychology students, trained by a psychologist with testing experience.
Data quality was assessed and controlled through the application of a questionnaire restricted to a 10%-random sample of all children. Epi-Info 6.0 and Stata 11.0 were used to analyze data. The theoretical model, detailed in Fig. 1, was created considering the hierarchical relationship between the variables in order to identify potential confounding factors.

Initially, the frequencies of the independent variables were obtained to characterize the study sample. Then, a bivariate analysis between the exposure factors and the outcome was performed using Student's t-test for dichotomous exposures and ANOVA for ordinal exposures. Linear regression (to assess the outcome as average) and logistic regression (when the outcome was assessed on a dichotomous basis: percentile <75 versus ≥ 75, characterizing below-average or average intellectual capacity, versus superior intellectual capacity) were used for the multivariable analysis, and variables with p<0.10 were maintained in the model as they were deemed potential confounding factors. In the final analysis, only variables with p <0.05 were associated with the outcome in a statistically significant manner.
ResultsDuring the study period, 3,449 children were born, 81% of whom lived in the urban area of Pelotas. 951 infants were visited at age 30 days (2.3% loss); 940 infants at age 90 days (3.4% loss), and 931 infants at age six months (4.3% loss). The results of these visits were described in a previous publication.14 616 children were located at 8 years old, provided that 560 children participated of the second visit for the application of the Raven's Colored Progressive Matrices. The following were excluded from the assessment: 38 (6.2%) children who were not located after three attempts, 8 (1.3%) who presented some disease or clinical complication preventing them from taking the test, and 10 (1.6%) who refused to take the test.
Of the 560 monitored binomials, 296 (52.9%) mothers breastfed their babies up to at least the sixth month of life. Approximately half of the sample (247 – 44.1%) was exclusively breastfed up to three months of life, and only 45 (8%) mothers breastfed their children for less than 30 days. At six months, only 88 (15.7%) infants were exclusively breastfed. No statistically significant difference was found in BF rates at six months between the different social classes (p=0.47) and the different maternal education (p=0.88).
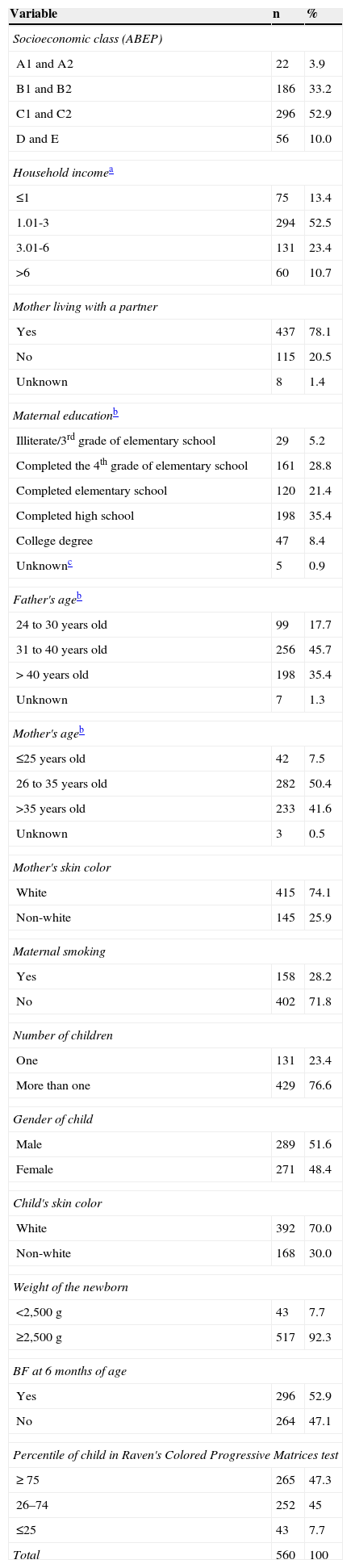
Sociodemographic and economic characteristics of the sample, as well as other maternal and infant data, are presented in Table 1. As to gestational age, 89.5% were term infants and, as to nutritional condition, 51.4% of the children at age 8 years were eutrophic.
Sample distribution pursuant to socio-demographic, maternal, and children characteristics – Pelotas (RS), Brazil, 2012.
| Variable | n | % |
|---|---|---|
| Socioeconomic class (ABEP) | ||
| A1 and A2 | 22 | 3.9 |
| B1 and B2 | 186 | 33.2 |
| C1 and C2 | 296 | 52.9 |
| D and E | 56 | 10.0 |
| Household incomea | ||
| ≤1 | 75 | 13.4 |
| 1.01-3 | 294 | 52.5 |
| 3.01-6 | 131 | 23.4 |
| >6 | 60 | 10.7 |
| Mother living with a partner | ||
| Yes | 437 | 78.1 |
| No | 115 | 20.5 |
| Unknown | 8 | 1.4 |
| Maternal educationb | ||
| Illiterate/3rd grade of elementary school | 29 | 5.2 |
| Completed the 4th grade of elementary school | 161 | 28.8 |
| Completed elementary school | 120 | 21.4 |
| Completed high school | 198 | 35.4 |
| College degree | 47 | 8.4 |
| Unknownc | 5 | 0.9 |
| Father's ageb | ||
| 24 to 30 years old | 99 | 17.7 |
| 31 to 40 years old | 256 | 45.7 |
| > 40 years old | 198 | 35.4 |
| Unknown | 7 | 1.3 |
| Mother's ageb | ||
| ≤25 years old | 42 | 7.5 |
| 26 to 35 years old | 282 | 50.4 |
| >35 years old | 233 | 41.6 |
| Unknown | 3 | 0.5 |
| Mother's skin color | ||
| White | 415 | 74.1 |
| Non-white | 145 | 25.9 |
| Maternal smoking | ||
| Yes | 158 | 28.2 |
| No | 402 | 71.8 |
| Number of children | ||
| One | 131 | 23.4 |
| More than one | 429 | 76.6 |
| Gender of child | ||
| Male | 289 | 51.6 |
| Female | 271 | 48.4 |
| Child's skin color | ||
| White | 392 | 70.0 |
| Non-white | 168 | 30.0 |
| Weight of the newborn | ||
| <2,500 g | 43 | 7.7 |
| ≥2,500 g | 517 | 92.3 |
| BF at 6 months of age | ||
| Yes | 296 | 52.9 |
| No | 264 | 47.1 |
| Percentile of child in Raven's Colored Progressive Matrices test | ||
| ≥ 75 | 265 | 47.3 |
| 26–74 | 252 | 45 |
| ≤25 | 43 | 7.7 |
| Total | 560 | 100 |
ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BF, breastfeeding.
Regarding the assessment with Raven's Colored Progressive Matrices, 43 (7.7%) children were intellectually below average or intellectually deficient. The average score of children in the test was 22.56 points, with a standard deviation of 5.93, which, for the age group, corresponds to a percentile of 60, i.e., average intellectual capacity.
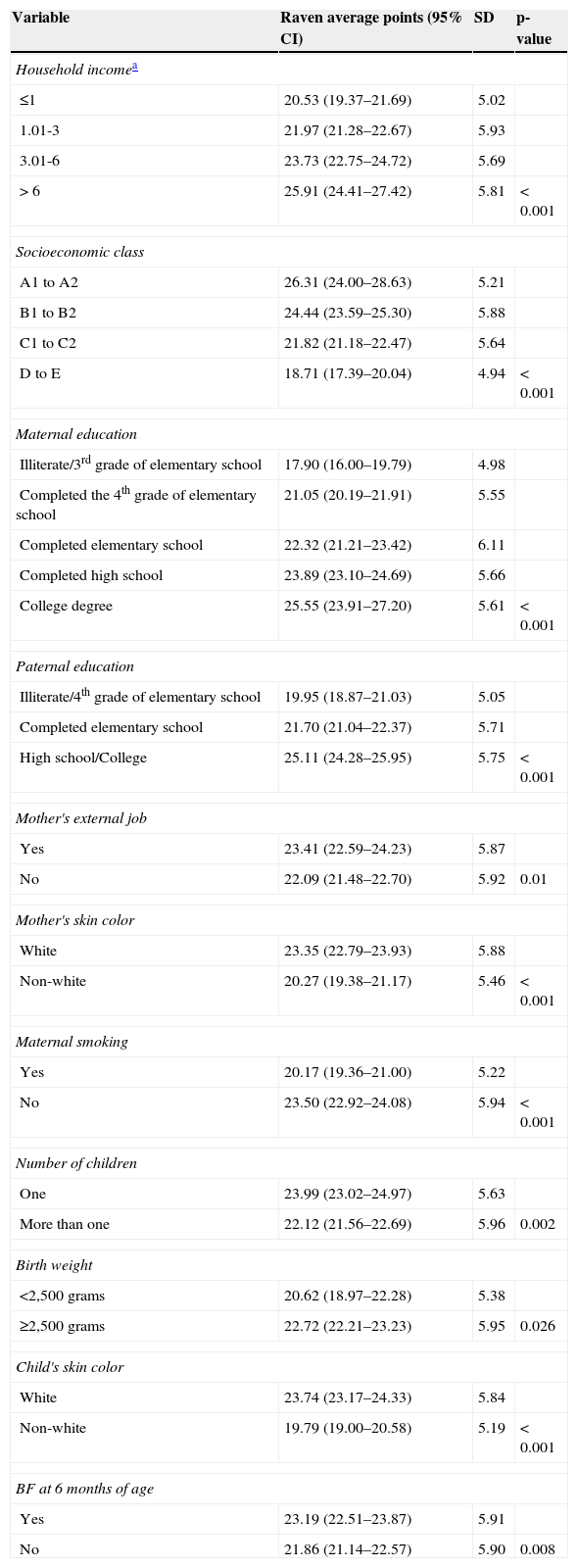
In the bivariate analysis, the following variables were not significantly associated with the outcome: maternal (p=0.98) and paternal (p=0.95) age, gender of child (p=0.25), Z-score for weight (p=0.30), gestational age (p=0.19), and presence of partner (p=0.08), and were not presented on a table. Statistically significant associations are detailed in Table 2. No significant association was found between exclusive BF at one, three, and six months and the children's performance in the test.
Unadjusted analysis of independent variables and average points obtained in Raven's Colored Progressive Matrices Test – Pelotas (RS), Brazil, 2012.
| Variable | Raven average points (95% CI) | SD | p-value |
|---|---|---|---|
| Household incomea | |||
| ≤1 | 20.53 (19.37–21.69) | 5.02 | |
| 1.01-3 | 21.97 (21.28–22.67) | 5.93 | |
| 3.01-6 | 23.73 (22.75–24.72) | 5.69 | |
| > 6 | 25.91 (24.41–27.42) | 5.81 | < 0.001 |
| Socioeconomic class | |||
| A1 to A2 | 26.31 (24.00–28.63) | 5.21 | |
| B1 to B2 | 24.44 (23.59–25.30) | 5.88 | |
| C1 to C2 | 21.82 (21.18–22.47) | 5.64 | |
| D to E | 18.71 (17.39–20.04) | 4.94 | < 0.001 |
| Maternal education | |||
| Illiterate/3rd grade of elementary school | 17.90 (16.00–19.79) | 4.98 | |
| Completed the 4th grade of elementary school | 21.05 (20.19–21.91) | 5.55 | |
| Completed elementary school | 22.32 (21.21–23.42) | 6.11 | |
| Completed high school | 23.89 (23.10–24.69) | 5.66 | |
| College degree | 25.55 (23.91–27.20) | 5.61 | < 0.001 |
| Paternal education | |||
| Illiterate/4th grade of elementary school | 19.95 (18.87–21.03) | 5.05 | |
| Completed elementary school | 21.70 (21.04–22.37) | 5.71 | |
| High school/College | 25.11 (24.28–25.95) | 5.75 | < 0.001 |
| Mother's external job | |||
| Yes | 23.41 (22.59–24.23) | 5.87 | |
| No | 22.09 (21.48–22.70) | 5.92 | 0.01 |
| Mother's skin color | |||
| White | 23.35 (22.79–23.93) | 5.88 | |
| Non-white | 20.27 (19.38–21.17) | 5.46 | < 0.001 |
| Maternal smoking | |||
| Yes | 20.17 (19.36–21.00) | 5.22 | |
| No | 23.50 (22.92–24.08) | 5.94 | < 0.001 |
| Number of children | |||
| One | 23.99 (23.02–24.97) | 5.63 | |
| More than one | 22.12 (21.56–22.69) | 5.96 | 0.002 |
| Birth weight | |||
| <2,500 grams | 20.62 (18.97–22.28) | 5.38 | |
| ≥2,500 grams | 22.72 (22.21–23.23) | 5.95 | 0.026 |
| Child's skin color | |||
| White | 23.74 (23.17–24.33) | 5.84 | |
| Non-white | 19.79 (19.00–20.58) | 5.19 | < 0.001 |
| BF at 6 months of age | |||
| Yes | 23.19 (22.51–23.87) | 5.91 | |
| No | 21.86 (21.14–22.57) | 5.90 | 0.008 |
BF, breastfeeding; CI, confidence interval; SD, standard deviation.
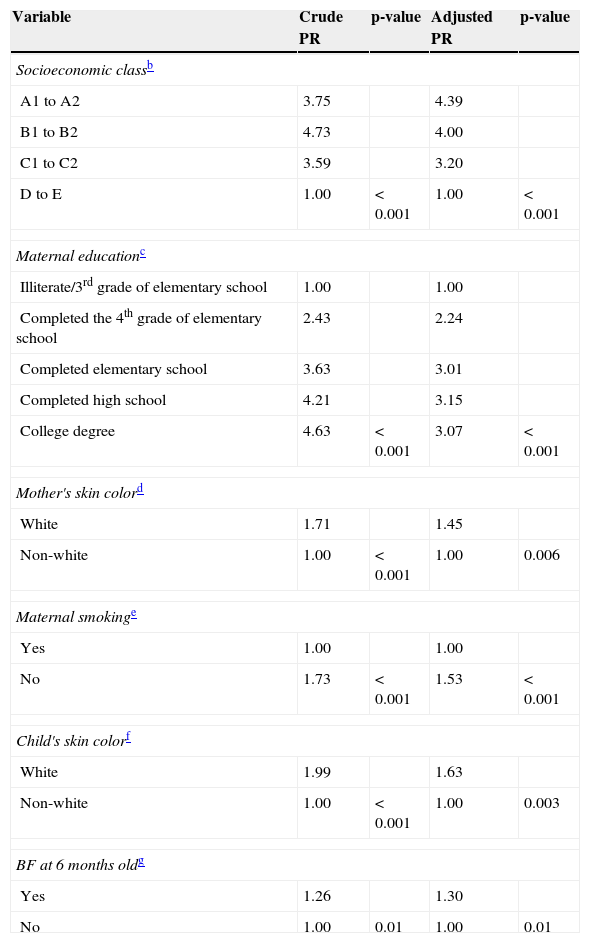
The following variables were included in the multivariable analysis: household income, socioeconomic class, parental education, mother's skin color, marital status, number of children, maternal smoking, working mothers, child's skin color, birth weight, and BF at six months old. Mother's and child's skin color, socioeconomic class, maternal education, maternal smoking, and BF at six months old (p=0.007) were still associated with the outcome.
By assessing performance on a dichotomous basis, children breastfed for six months or more showed better performance in the test (PR=1.26; p-value 0.01). In the logistic regression, by adjusting the aforementioned variables, the value obtained was 1.30, with a p-value of 0.01 (Table 3).
Unadjusted and adjusted analyses for intellectual capacity in a dichotomous outcome, considering the prevalence of the best performancea – Pelotas (RS), Brazil, 2012.
| Variable | Crude PR | p-value | Adjusted PR | p-value |
|---|---|---|---|---|
| Socioeconomic classb | ||||
| A1 to A2 | 3.75 | 4.39 | ||
| B1 to B2 | 4.73 | 4.00 | ||
| C1 to C2 | 3.59 | 3.20 | ||
| D to E | 1.00 | < 0.001 | 1.00 | < 0.001 |
| Maternal educationc | ||||
| Illiterate/3rd grade of elementary school | 1.00 | 1.00 | ||
| Completed the 4th grade of elementary school | 2.43 | 2.24 | ||
| Completed elementary school | 3.63 | 3.01 | ||
| Completed high school | 4.21 | 3.15 | ||
| College degree | 4.63 | < 0.001 | 3.07 | < 0.001 |
| Mother's skin colord | ||||
| White | 1.71 | 1.45 | ||
| Non-white | 1.00 | < 0.001 | 1.00 | 0.006 |
| Maternal smokinge | ||||
| Yes | 1.00 | 1.00 | ||
| No | 1.73 | < 0.001 | 1.53 | < 0.001 |
| Child's skin colorf | ||||
| White | 1.99 | 1.63 | ||
| Non-white | 1.00 | < 0.001 | 1.00 | 0.003 |
| BF at 6 months oldg | ||||
| Yes | 1.26 | 1.30 | ||
| No | 1.00 | 0.01 | 1.00 | 0.01 |
BF, breastfeeding; PR, prevalence ratio.
This study evaluated general intellectual capacity through the application of Raven's Colored Progressive Matrices in 560 children from a birth cohort in the city of Pelotas. Studies available in the literature use several tests to assess intelligence. For this study, the Raven's Colored Progressive Matrices12 test was chosen because it is easily and quickly applied (15 to 20minutes), favoring participation, and is indicated for the determination of intellectual development in studies.13
In 1999, Anderson et al. performed a meta-analysis to evaluate the effect of BF on children's cognitive development. 11 studies that used different types of tests to measure the intelligence quotient were included in the analysis. The outcome used was the average difference in test scores between breastfed and non-breastfed groups. The result found was a difference of averages of 3.16 (95% CI; 2.35–3.98) in the intelligence quotient in favor of BF; however, the authors suggested that 2.0 to 2.4 points of difference in the test scores between the groups were due to confounding factors, and this was the greatest limitation of the study.9 In the present study, the difference in the averages found between the breastfed and non-breastfed groups at age six months was of 1.33 (p=0.008). The effect of BF became more obvious when comparing the performance in the test, classifying it in percentiles and assessing on a dichotomous basis: breastfed children had a 30% higher probability of being classified as above-average intellectual capacity when compared to those weaned before six months. Nonetheless, no significant association between type of BF (exclusive or not) and the outcome was observed.
This study demonstrated that BF up to the sixth month of life promoted an increase in intellectual capacity, even after adjustment for confounding factors. An advantage in relation to other investigations on the same subject is that, as a cohort study with prospective data collection, the recall bias regarding BF data was eliminated.
Regarding the best scores achieved by children who had proper birth weight and whose mothers did not smoke, findings were similar to those from other studies. However, unlike other studies,15 no association was found between gestational age and better cognitive development. This is warranted because the initial purpose of the cohort study was to assess data on BF and, therefore, infants who needed hospitalization immediately after birth and were over 24hours away from their mothers were excluded from the monitoring. Hence, premature infants who comprised the sample were only those born close to term or those that did not need long hospital care.
A study in Australia with 302 children did not find an association between duration of BF and children's intelligence quotient (IQ). Quality of home environment was the strongest IQ predictor at age 4 years.16 While maternal intellectual capacity was not assessed in the present study, maternal education remained directly associated with the outcome, even after adjustment for confounding factors. While the quality of home environment was not directly assessed, children with working mothers achieved a higher score in the test. A tendency of better intellectual capacity among children whose mothers had a partner participating in the family life (p=0.08) was also observed.
An observational study published in 2006 aimed to evaluate the influence of maternal IQ on children's IQ. A database from a 1979 US cohort was used. After adjustment for confounding factors and for maternal IQ, BF represented a small and non-significant increase in children's intellectual capacity.17 While maternal intellectual capacity was not assessed in the present study, maternal education remained directly associated with the outcome, even after adjustment for confounding factors.
One of the limitations of the present study was the great amount of losses in comparison with the previous visit; despite that, the visited sample at age 8 years was representative of the original population. Another limitation was the lack of a questionnaire to assess attention deficit, which may have adversely affected the interpretation of results in children with a low score.
The differential of this study is that it was one of the first to be performed in Brazil and, even after adjustment for potential confounding factors, important socioeconomic factors and BF at six months of age remained associated with the outcome. This finding reinforces the WHO recommendations to encourage mothers to breastfeed their children, especially in the first year of life,18 as it is known that, in addition to the physicochemical characteristics of breast milk, the skin-to-skin contact, the physical stimulation, and the mother's gaze toward the infant are significantly higher during BF compared to artificial feeding.19
BF, in addition to strengthening mother-baby bonding and providing already well-documented benefits to child health, also contributes to general intellectual capacity, even among those with lower socioeconomic conditions. Therefore, BF must be further stimulated in developing countries, where children are exposed to several risks, among which are a high prevalence of diseases, unfavorable and/or premature pregnancies, and living in adverse socioeconomic conditions.20,21
Conflicts of interestThe authors declare no conflicts of interest.
The authors thank the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS) and the Universidade Católica de Pelotas (UCPel) for Research Initiation Scholarships, as well as the Conselho Nacional de Pesquisa (CNPQ), for the Research Productivity Scholarship (EPA).
Please cite this article as: Fonseca AL, Albernaz EP, Kaufmann CC, Neves IH, de Figueiredo VL. Impact of breastfeeding on the intelligence quotient of eight-year-old children. J Pediatr (Rio J). 2013;89:346–53.




