



To assess temporal trends of hospitalizations and deaths from pertussis in Brazilian children in the period of 1996–2013.
MethodsThis was a descriptive ecological study of temporal trends, based on the DATASUS database. The number of hospitalizations and deaths from pertussis in children up to 19 years of age from January 1996 to December 2013 was obtained. Descriptive statistics were applied for data analysis.
ResultsDuring the study period, a total of 19,047 hospital admissions from pertussis were recorded, of which 88.2% occurred in infants younger than 1 year. In the period 1996–2010, the mean annual number of admissions was 755, ranging from a maximum of 1179 in 2004 to a minimum of 400 in 2010. There was an increase of admissions in the last three consecutive years (2011, 2012, and 2013) with 1177, 2954 and 3589 hospitalizations, respectively. There were 498 deaths from pertussis throughout the study period, of which 96.8% occurred in children younger than one year. There was an increase in the number of deaths from pertussis in children in the years 2011, 2012, and 2013, with 40, 93, and 87 recorded deaths, respectively. The increase in hospitalizations and deaths from pertussis in children occurred in all regions of the country, with the highest increase observed in the Southeast, North and Northeast regions.
ConclusionsThere was a substantial increase in hospitalizations and deaths from pertussis in children for three consecutive years (2011, 2012, and 2013) in all Brazilian regions. The most affected age group was that of children younger than one year.
Avaliar tendência temporal de internações e óbitos por coqueluche em crianças brasileiras no período de 1996 a 2013.
MétodosTrata-se de um estudo ecológico descritivo de tendência temporal, baseado no banco de dados DATASUS. Foram extraídos os números de internações e de óbitos por coqueluche em crianças até 19 anos de idade no período de janeiros de 1996 a dezembro de 2013. A estatística descritiva foi aplicada para análise de dados.
ResultadosNo período estudado foram registradas 19.047 internações por coqueluche, das quais 88,2% foram lactentes menores de um ano. No período de 1996 a 2010, o número médio anual de internações foi de 755, oscilando entre o máximo de 1179 em 2004 e o mínimo de 400 em 2010. Houve um acréscimo de internações nos últimos três anos consecutivos (2011, 2012 e 2013), com 1177, 2954 e 3589 registros, respectivamente. Ocorreram 498 óbitos por coqueluche em todo o período estudado, dos quais 96,8% eram menores de um ano. Houve acréscimo no número de óbitos por coqueluche em crianças nos anos 2011, 2012 e 2013, com 40, 93 e 87 registrados, respectivamente. O aumento de internações e óbitos por coqueluche em crianças ocorreu em todas as regiões do país, havendo maior acréscimo nas regiões Sudeste e Norte-Nordeste.
ConclusõesHouve um aumento substancial de internações e de óbitos por coqueluche em crianças por três anos consecutivos (2011, 2012 e 2013) em todas as regiões brasileiras. A faixa etária mais atingida foi a de menores de um ano.
Pertussis is a highly infectious and contagious human respiratory disease caused by the coccobacillus Bordetella pertussis. Although it is a vaccine-preventable disease, pertussis remains an important cause of child morbidity and mortality worldwide, and a source of public health concern, even in countries where vaccination coverage is high.1–3 According to the World Health Organization (WHO), there were approximately 16 million cases of pertussis in the world in 2008, with 95% occurring in developing countries, causing about 200,000 infant deaths.1
In many developed countries with high vaccination coverage, pertussis has re-emerged in the last two decades with increasing incidence, especially among young infants not yet fully immunized, as well as adolescents and young adults who are potentially capable of transmitting the disease to younger children.2–5 Some hypotheses have been considered for the resurgence of the disease, such as loss of acquired immunity during the time after vaccination, reduced vaccine effectiveness, use of new diagnostic methods, improved epidemiological surveillance systems, and genetic changes in bacteria.2,5,6
In Brazil, data from the Ministry of Health's epidemiological surveillance show an increase in the incidence of pertussis since 2011, after over a decade of stability.7 Approximately 70% of cases were children younger than 1 year, with most younger than 3 months.
Due to the difficulties in the clinical diagnosis and lack of availability of sensitive and specific laboratory tests, pertussis remains an underdiagnosed and underreported disease.6,8,9 Accurate data on the incidence rate of this disease are difficult to obtain, particularly in developing countries. Therefore, studies on hospital morbidity and mortality from pertussis can provide important additional information in assessing the current national epidemiological situation of the disease.
This study aimed to describe temporal trends in hospital admissions through the Brazilian Unified Health System (Sistema Único de Saúde [SUS]) and deaths from pertussis in Brazilian children up to 19 years of age, from 1996 to 2013. The direct costs of hospitalization from pertussis through SUS in 2013 were also calculated.
MethodsThis was a descriptive ecological study of temporal trends, based on the database of the Brazilian Unified Health System Informatics Department (DATASUS). This study involved only public-domain data that do not identify the participants and, therefore, did not require approval by the Research Ethics Committee.10 The numbers of hospitalizations and number of deaths from pertussis, as well as the number of hospitalizations from all causes in children aged up to 19 years were obtained from January 1996 to December 2013. The choice of the studied period, 1996–2013, is justified as the Tenth Revision of the International Classification of Diseases (ICD-10) was implemented in Brazil in 1996. Data on the total amount paid by SUS for hospitalizations from pertussis in 2013, the mean amount paid per admission, and the length of hospitalization (in days) for this disease were also obtained.
Data extraction was performed by one individual, using a standardized form. The extracted data were verified by another researcher. The line graphs were used to plot the temporal trends of hospitalizations and deaths from pertussis in the studied period, with absolute numbers plotted on the vertical axis and years of observation on the horizontal axis. Descriptive statistics were applied for data analysis using the program Stata (StataCorp. 2009. Stata Statistical Software: Release 11. College Station, TX, USA).
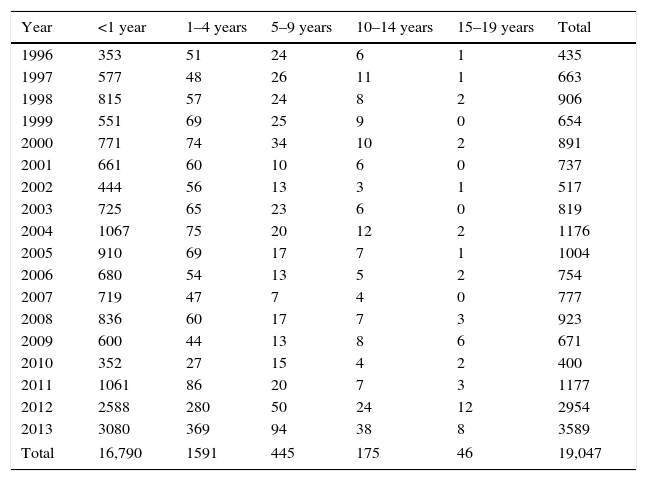
ResultsDuring the study period, a total of 19,047 admissions from pertussis were recorded in children younger than 19 years of age in Brazil. Of the total admissions, 88.2% (16,790 records) were of children younger than 1 year and only 1.2% (221 records) were adolescents aged 10–19 years (Table 1).
Number of hospital admissions from pertussis in Brazilian children up to 19 years of age, 1996–2013.
| Year | <1 year | 1–4 years | 5–9 years | 10–14 years | 15–19 years | Total |
|---|---|---|---|---|---|---|
| 1996 | 353 | 51 | 24 | 6 | 1 | 435 |
| 1997 | 577 | 48 | 26 | 11 | 1 | 663 |
| 1998 | 815 | 57 | 24 | 8 | 2 | 906 |
| 1999 | 551 | 69 | 25 | 9 | 0 | 654 |
| 2000 | 771 | 74 | 34 | 10 | 2 | 891 |
| 2001 | 661 | 60 | 10 | 6 | 0 | 737 |
| 2002 | 444 | 56 | 13 | 3 | 1 | 517 |
| 2003 | 725 | 65 | 23 | 6 | 0 | 819 |
| 2004 | 1067 | 75 | 20 | 12 | 2 | 1176 |
| 2005 | 910 | 69 | 17 | 7 | 1 | 1004 |
| 2006 | 680 | 54 | 13 | 5 | 2 | 754 |
| 2007 | 719 | 47 | 7 | 4 | 0 | 777 |
| 2008 | 836 | 60 | 17 | 7 | 3 | 923 |
| 2009 | 600 | 44 | 13 | 8 | 6 | 671 |
| 2010 | 352 | 27 | 15 | 4 | 2 | 400 |
| 2011 | 1061 | 86 | 20 | 7 | 3 | 1177 |
| 2012 | 2588 | 280 | 50 | 24 | 12 | 2954 |
| 2013 | 3080 | 369 | 94 | 38 | 8 | 3589 |
| Total | 16,790 | 1591 | 445 | 175 | 46 | 19,047 |
Fig. 1A shows the temporal trend in the number of hospitalizations from pertussis in Brazilian children. In the period 1996–2010, the mean annual number of admissions was 755, ranging from a maximum of 1179 in 2004 to a minimum of 400 in 2010. There was an increase in the number of admissions in the last three consecutive years (2011, 2012, and 2013), with 1177, 2954, and 3589 records, respectively. The mean annual number of hospitalizations from pertussis in the period of 2011 to 2013 increased by 242% in relation to the previous period. In contrast, the total number of general admissions in children during the study period decreased each year (Fig. 1B). The increase in admissions from pertussis in the last three years occurred in all geographic regions of the country, but was more evident in the Southeast, North, Northeast, and South regions (Fig. 2).
 Number of hospital admissions from pertussis in Brazilian children, 1996–2013. (B) Total number of hospitalizations in Brazilian children, 1996–2013.")

In the period from 1996 to 2013, 498 deaths from pertussis were recorded in children younger than 19 years in Brazil, of which 96.8% (482 records) occurred in children younger than 1 year. A growing temporal trend in the number of deaths from pertussis in Brazilian children can be observed in the last three years, with 40, 93, and 87 deaths recorded in 2011, 2012, and 2013, respectively (Fig. 3). This trend occurred in all regions of the country, with the highest increase in the Southeast, North and Northeast regions. In 2010, the number of deaths from pertussis was lower than ten in the Southeast, North and Northeast regions, and lower than five in the South and Midwest regions. This number increased to 40, 26, 10 and 11 in 2013 in the Southeast, North, Northeast, South, and Midwest regions, respectively.

In 2013, approximately five million reais (R$ 5,000,000) were paid by SUS for hospitalizations from pertussis in children in Brazil. Those aged less than 1 year accounted for approximately 90% of total costs with hospital admissions from this disease. Moreover, this is the age group that had the highest mean hospital stay (7.3 days), resulting in higher mean amounts paid per admission (R$ 1365.26).
DiscussionThe present study disclosed a substantial increase in the numbers of hospitalizations and deaths from pertussis in Brazilian children in the last three years (2011, 2012, and 2013). This increase occurred in all geographic regions of the country, although it was more evident in the Southeast, North and Northeast regions. Children aged less than 1 year accounted for most of the deaths, hospitalizations, and related costs from pertussis.
The results of this study corroborate data from the Ministry of Health epidemiological surveillance, which show an increase in confirmed cases of pertussis in Brazil in the last three years.7 The incidence rate was 1.2, 2.8, and 3.1 per 100,000 inhabitants in 2011, 2012, and 2013, respectively, compared with the mean of 0.7 per 100,000 inhabitants from 1996 to 2010. The highest increase in the incidence of pertussis occurred in infants younger than 1 year, especially those aged less than 3 months. This phenomenon has already occurred in many developed countries over the past two decades, prompting the implementation of new vaccination strategies against pertussis, such as the cocoon strategy, vaccination of pregnant women, vaccination of adolescents and adults, as well as of health professionals.2,11–15
The cocoon strategy consists in vaccinating all individuals living with the infant (parents, grandparents, siblings, and caregivers), because in 75% of cases, the source of disease transmission is a member of the family, with the mother representing the main source of contagion.2,11,14 The vaccination of pregnant women aims to introduce the production of high antibody titers against pertussis, allowing the transplacental transfer of these antibodies to the fetus, resulting in indirect vaccine protection in the first months of life, when the child is not yet old enough to receive or complete the vaccination schedule.2,12,14,15
Due to the lack of convincing evidence on the efficacy and cost-effectiveness of these strategies, either alone or in combination, there is substantial variation between countries in Europe, North America, and the Pacific regarding the implementation of these new vaccination strategies.2 A booster dose using the acellular vaccine is given to adolescents aged 11–17 years in most developed countries, such as Germany, Australia, Austria, Belgium, Canada, USA, France, Finland, Italy, and Switzerland, except for Great Britain, the Netherlands, and Poland.16–18 The cocoon strategy has been implemented in Germany, Australia, Belgium, USA, France, Finland, Great Britain, the Netherlands, and Switzerland.16–18 In some countries, the cocoon strategy is combined with vaccination of adults and health professionals.
In Brazil, although the Brazilian Society of Pediatrics and the Brazilian Society of Immunization recommend the vaccination of adolescents against pertussis, this vaccine has not yet been included in the SUS Basic Immunization Calendar for this population.19,20 In November 2014, the Ministry of Health introduced the adsorbed diphtheria, tetanus, and acellular pertussis vaccine (DTaP) in the SUS National Vaccination Calendar for pregnant women and health professionals who treat newborns in maternity wards and neonatal intensive care units.21 The impact of this vaccine strategy on child morbimortality from pertussis and the cost-effectiveness of vaccination should be assessed at the national level.
In addition to increased morbimortality from pertussis in young infants, these patients may present with atypical disease symptoms, which complicates and delays diagnosis and treatment.6,22,23 Therefore, special attention should be paid to this population, which requires greater awareness of the medical team about the risk of disease and the use of diagnostic tests. Pertussis should also be included in the differential diagnosis of prolonged cough in adults and adolescents, especially in non-atopic patients.23 As important as the diagnosis is the early treatment of patients and antimicrobial prophylaxis for contacts, preventing the dissemination of the disease to susceptible individuals.24
In 2013, approximately five million reais (R$5,000,000) were paid by SUS for hospitalizations from pertussis in children in Brazil. This amount represents a significant financial burden on the health system of the country. Outpatient and emergency care costs associated with older children, adolescents, and adults, as well as indirect costs related to the disease, should be even higher.
Some limitations should be considered when interpreting the results of this study. According to the Epidemiological Surveillance Guide of the Ministry of Health,25 diagnostic confirmation of pertussis must be made by laboratory testing, through the culture of Bordetella pertussis bacteria or by isolation through polymerase chain reaction (PCR). Confirmation can also be attained using clinical or clinical-epidemiological criteria.
Therefore, the diagnosis of pertussis depends on the technical and operational conditions of the epidemiological surveillance system in each geographical area to detect, report, investigate, and confirm cases. When the confirmation depends only on clinical data, diagnostic errors may occur because pertussis may be misdiagnosed as other conditions caused by other agents that produce pertussis syndrome.6,9,26 These situations can lead to over- or underreporting of cases. Due to the relatively small number of deaths and hospitalizations from pertussis, the present study used the absolute number of occurrences rather than mortality and hospitalization incidence rates. However, the absolute number of disease occurrence can be influenced by the variation in the population over time. The simple increase in the population could have contributed to the higher number of hospitalizations and deaths. However, the significant increase in absolute numbers of hospitalizations and deaths from pertussis that occurred in the last three years does not support this hypothesis. Additionally, proportional mortality and hospitalization from pertussis were not included because the constant reduction in mortality and the number of overall hospital admissions in Brazilian children over the recent decades could affect these measures. Another limitation is related to the incapacity to make inferences about the causes of the trends found by the study.
Even considering the above limitations, it can be concluded that there was a substantial increase in hospitalizations and deaths from pertussis in children for three consecutive years (2011, 2012, and 2013) in the country as a whole and in all Brazilian regions. The most affected age group was that of children younger than one year. These results emphasize the importance of epidemiological surveillance and implementation of new vaccination strategies against pertussis in Brazil. Greater attention should be given to the Southeast, North, and Northeast regions, which have shown a higher increase in the numbers of hospitalizations and deaths due to pertussis in recent years.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Mançaneira JF, Benedetti JR, Zhang L. Hospitalizations and deaths due to pertussis in children from 1996 to 2013. J Pediatr (Rio J). 2016;92:40–5.




